Ophthalmology and Vision Care
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2836-2853 | Journal DOI: 10.61148/2836-2853/OVC


James Lim Wen Siang *, Ong Wu Zhuan, Ng Sok Lin
Department of Ophthalmology, Taiping Hospital, Perak, Malaysia.
*Corresponding Author: James Lim Wen Siang, Department of Ophthalmology, Taiping Hospital, Perak, Malaysia.
Received: January 22, 2022
Accepted: February 01, 2022
Published: February 04, 2022
Citation: James Lim Wen Siang. (2022) “Review of Endophthalmitis Cases in District Hospital: Case Series”, Ophthalmology and Vision Care, 2(1); DOI: http;//doi.org/01.2022/1.1026
Copyright: © 2022. James Lim Wen Siang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Purpose:
To describe a consecutive series of endophthalmitis of all causes and to report the socio-demography, predisposing factors, causative organism, treatment given and the visual outcome in these challenging cases.
Methods:
A 3-year retrospective review of patients diagnosed with endophthalmitis that received treatment and follow up from the period between January 2018 and December 2020.
Results:
A total of 16 eyes of 15 patients were studied. Male to female ratio was 4:1. Most (47%) patients were between 60 to79 years old with the mean age of 60 years old. There were 15(93.75%) cases of exogenous endophthalmitis and 1(6.25%) case of endogenous endophthalmitis. Nine cases (56.25%) were associated with microbial keratitis, 3 eyes (18.75%) had post traumatic endophthalmitis, 1 eye (6.25%) had acute postoperative endophthalmitis, 1 eye (6.25%) had post intravitreal injection and 1 case (6.25%) was due to blebitis. The mean duration of hospitalization was 12 days and the mean follow-up duration was 144 days. Culture and sensitivity were done in all cases where 9 eyes (56.3%) were found to be positive for growth. Gram negative bacteria were the most prevalent causative organism of endophthalmitis in this study. Most patients (81.3%) had visual acuity +1.0(Log MAR) during the presentation.
Intravitreal antibiotic given in 11 (68.8%) eyes and vitrectomy done in 7 (43.8%) eyes. Despite maximal treatment, the visual outcome remained poor (>6/60) in general and 5 eyes (31.3%) ended up with evisceration.
Conclusion:
Acute endophthalmitis is a rare but potentially devastating condition. Visual prognosis of endophthalmitis is generally poor and is an important cause of ocular morbidity. Hence, prevention is the key factor and prompt treatment is the key.
Introduction:
Infective endophthalmitis, a potentially devastating ocular disease is a major public health concern. It is characterized by significant and progressive inflammation of intraocular tissues and fluids. Broadly, it can be divided into exogenous and endogenous endophthalmitis [1]. Exogenous endophthalmitis is caused by microorganisms from the external environment, common causes included infective keratitis, trauma or intraocular surgery. [1-2]. On the other hand, endogenous endophthalmitis is due to hematogenous spread of microorganism from distant site in the body [1-2], usually occurred in immunocompromised or debilitated patients and is far less common than exogenous endophthalmitis that only accounted 2-6% of all endophthalmitis cases [3].
Materials & Methods:
This was a retrospective study of patients diagnosed with endophthalmitis which required hospital admission from the period between January 2018 and December 2020 in Taiping Hospital, Perak, Malaysia.
Taiping hospital is located in the northern region of Perak. Being the second largest hospital in Perak, it is an important referral center for other district hospitals in northern Perak.
The relevant data were traced and acquired from hospital’s medical records unit. Data collection was done to include the demographic data (age, race, gender, occupation) and clinical characteristics of the patients, which included the past surgical history of the studied eye, predisposing factor, presenting visual acuity (represented in Log MAR), presentation interval, any surgical intervention (if any), length of hospital admission, duration of outpatient follow up and final visual acuity at the latest follow up visit. Culture and sensitivity results (corneal scraping or intravitreal tapping) and treatment received were also analyzed.
Inclusion criteria:
Patients with endophthalmitis regardless of comorbidity that required hospital admission within the period of January 2018 until December 2020
Exclusion criteria:
Patients who defaulted follow up within less than 6 weeks after first presentation and patients with incomplete data.
Data analysis were performed using Statistical Package for Social Sciences (SPSS) version 26.0. Descriptive statistics were presented by mean (standard deviation), and categorical data were presented in numerical variables and frequency (percentage).
Results:
Demographics:
A total of 15 patients with endophthalmitis that required hospital admission were identified from the
patient database at Taiping Hospital.
Of the 15 patients, 12 (86.6%) patients were males and 3 (13.4%) were females; the male to female ratio was 4:1. The distribution of cases according to age group is shown in Table 1. The age ranged from 36 to 80 years old with mean age of 59.5 years. Most of the patients predominantly fall in the age group of 60- 79 years old, and most of them (n=14, 93.3%) were Malay race and only 1(6.7%) was Chinese. Most of them were labourer (6, 40%) and retiree (6, 40%) as shown in Table 2.
A total of 16 eyes from 15 patients were included in this study. Seven cases (46.67%) involved the right eye, 7 cases (46.67%) involved the left eye, and 1 patient (6.67%) had bilateral eye involvement. Most of them (n=11, 68.8%) presented within up to 6 days following the onset of the symptoms.
|
Age Group (years) |
Male, n (%) |
Female, n (%) |
|
0-19 |
0 |
0 |
|
20-39 |
2 (13.33) |
0 |
|
40-59 |
4 (26.67) |
0 |
|
60-79 |
5 (33.33) |
2 (13.33) |
|
80 and above |
1 (6.67) |
1 (6.67) |
|
Total |
12 (80.0) |
3 (20.0%) |
|
Occupation |
Number (%) |
|
Labourer |
6 (40.0) |
|
Retiree |
6 (40.0) |
|
Police |
1 (6.7) |
|
Teacher |
1 (6.7) |
|
Businessman |
1 (6.7) |
Table 2: Occupation distributions
Clinical characteristics:
Out of the 15 studied patients, 3 (18.8%) of them had diabetes mellitus. Exogenous endophthalmitis (n=15, 93.75%) were predominantly involved in this study, while there was only 1 case (6.25%) of endogenous endophthalmitis. There were 9 (56.25%) eyes in which an infective keratitis complicated by acute endophthalmitis, followed by 3 (18.75%) cases of post traumatic endophthalmitis. One eye (6.25%) had cataract surgery done 2 weeks prior to symptoms onset, 1 (6.25%) eye received intravitreal anti-VEGF injection 4 days prior to symptoms onset and 1 (6.25%) eye had bleb associated infections.
Eight eyes (50%) had history of ocular surgery done in the affected eye before, 5 (31.3%) of them had cataract extraction with intraocular lens implantation, 2 (12.5%) had trabeculectomy done and 1 (6.3%) had penetrating keratoplasty done.
Thirteen (81.3%) eyes had vision worse than +1.0 (≥+1.0) during presentation and upon completing the treatment. This included 1 (6.25%) no perception to light (NPL) eye and 5 (31.25%) eyes that ended up with evisceration. Only 3 (18.8%) of them achieved vision better than +1.0 (<+1.0) in the end of treatment. Most of the patients (11, 68.8%) presented within 7 days after symptoms onset as shown in Table 4. The presentation interval ranged from 1-21 days with the mean of 6 days. Almost all (15, 93.8%) of them had no fundus view during the presentation. Duration of hospitalization ranged from 2 – 25 days with the mean of 11.7 days. In the other hand, the follow up duration ranged from 38-266 days with the mean of 144 days for each patient.
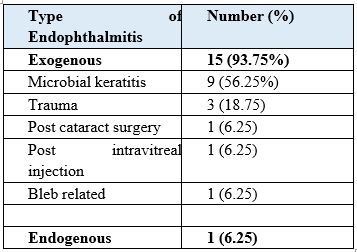
Table 3: Type and etiology of endophthalmitis
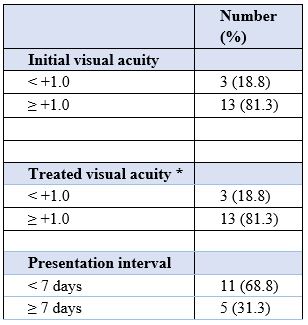
Table 4: Visual acuity and presentation interval
*Treated visual acuity included 5 eviscerated eyes
Microbiological Profile:
All the patients were investigated for culture and sensitivity from both the corneal tissue and vitreous sample. Nine (56.3%) of the 16 eyes were culture positive and 7(43.8%) eyes had no isolated organism. Organisms isolated from the culture positive group are shown in Table 5.
Among the 9 culture positive cases, there was 1 case with multiple organisms isolated, i.e. Bacillus sp. with Klebsiella pneumoniae. In this study, Gram negative bacteria were identified as the commonest causative organism for endophthalmitis followed by gram positive bacteria and fungus. (Table 5)
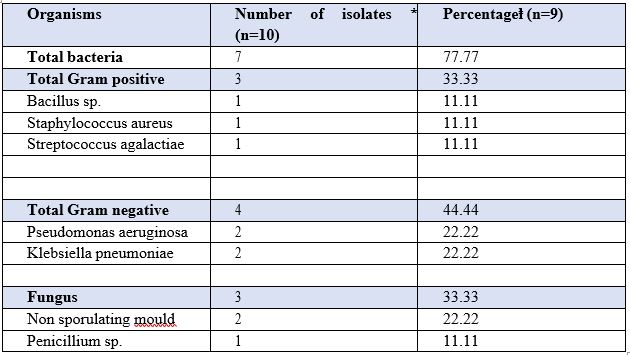
Table 5: Isolated organisms by culture
*Polymicrobial cultures
ⱡ Percentage of culture positive cases(n=9). Total is greater than 100% because of polymicrobial infections.
Among the 5 eyes (31.3%) that required evisceration, 100% of them were culture positive and all of them were due to microbial keratitis. Four (80%) of them were caused by bacteria, i.e. Streptococcus agalactiea, Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella pneumoniae and 1 (20%) was caused by fungus penicillium sp.
Treatment:
The first line on treatment included empirical topical antimicrobial agents and intravitreal antibiotic.
In this study, all eyes (16, 100%) were given topical antibiotic, 6 eyes (37.5%) were given topical antifungal. Systemic antibiotic was given in all (100%) of cases and systemic antifungal were added in 1 (6.25%) case.
Eleven (68.8%) of the eyes received intravitreal antibiotic injection, the number of injections ranged from 2-5 times with the mean of 2.6 times for each patient. The remaining 5 (31.25%) eyes had evisceration done within 24hours of presentation due to severe microbial keratitis complicated with endophthalmitis. Seven (43.8%) eyes underwent vitrectomy besides intravitreal antibiotic injection.
Discussion:
A good presenting visual acuity (<+1.0) was associated with a better visual outcome. Eyes with a primary visual acuity of light perception or less had the worst visual prognosis [8]. More than one third of patients (n=25, 38%) had nonfunctional vision (less than counting finger) after resolution of endophthalmitis [5]. Our study found that 81.3% of eyes had primary visual acuity of ≥ +1.0 and their vision remain poor upon completion of treatment.
In our study, most cases were associated with microbial keratitis. This finding is dissimilar to previous reports in which most cases developed endophthalmitis after ocular trauma [1] and after intraocular surgery [5]. Endophthalmitis is a major indication for evisceration or enucleation and corneal ulcer- related endophthalmitis has higher rate of evisceration compared to other causes of endophthalmitis [6,7]. In this study, all 5 eyes that were eviscerated were associated with culture positive microbial keratitis. Low socioeconomic status, living in remote areas with poor accessibility to health care center and lack of awareness of the adverse effect of keratitis possibly led to delayed presentation and delayed intervention, thence progressed into endophthalmitis [6]. The progression despite of prompt and appropriate management could be due to relatively virulent organisms with high antibiotic resistance pattern [7].
The causative organism for endophthalmitis may vary depending on the geographical location [1, 4]. This study is supported by Ramakrishnan et al [3] showing that bacteria is the most common causative organisms followed by fungus. Gram negative organism were more commonly isolated as compared to Gram positive organism in this study, in contrast with other studies which stated that Gram positive organism were more common [1,3].
Intravitreal antibiotics are the mainstay of treatment in the management of infective endophthalmitis [10]. Early vitrectomy for endophthalmitis leads to visual benefit in some cases [9]. In contrast, systemic antibiotic did not improve the final visual outcome [8]. In this study, all the salvageable eyes had received intravitreal antibiotic injection and 63.6% of them needed vitrectomy in the follow up but vitrectomy did not improve the final visual outcome.
The limitations of this study included that it was performed in a retrospective way and Taiping
Hospital is a district hospital that is still using a manual filing system for patients’ medical records.
There were difficulties in tracing the medical records, some data were missing, and the medical records are only kept for three years, all of which limited the study's sample size. A larger prospective multi-center researches should be conducted to gather more data and sample size, and eventually improve the management of endophthalmitis in future.
Conclusion:
Infective endophthalmitis had devastating sequelae that can cause blindness and even loss of eyeball. Despite advanced treatment, there appeared to be little in improvement in clinical outcome. Early diagnosis, intervention and aggressive treatment are crucial in controlling ocular inflammation to salvage the eye.
Conflicts of interest: The authors report no conflicts of interest.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org