Nursing and Healthcare Research
OPEN ACCESS | Volume 3 - Issue 1 - 2026
ISSN No: 3065-7679 | Journal DOI: 10.61148/3065-7679/NHR


Kevinilo
Nottingham University Hospitals NHS Trust · Department of Trauma and Orthopaedics.
*Corresponding Author: kevinilo, Nottingham University Hospitals NHS Trust · Department of Trauma and Orthopaedics.
Received date: July 02, 2023
Accepted date: August 08, 2023
Published date: September 14, 2023
Citation: kevinilo (2023). “The Effect of Selective Dorsal Rhizotomy On Gait Outcomes for Children with Cerebral Palsy’’. Nursing and Healthcare Research, 1(1); DOI: 10.61148/OTJ/001.
Copyright: © 2023 kevinilo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Management of spasticity is often challenging in children with Cerebral Palsy (CP), however selective dorsal rhizotomy (SDR) shows promising results in reducing spasticity. There is no consensus regarding patient selection for SDR and there are few studies investigating gait outcomes.
Method: This is a prospective study of 13 pre-selected ambulant children with CP who were suitable for SDR. 3D gait analysis was performed prior to SDR and 2 years post-SDR to assess gait parameters and calculate the gait profile score (GPS).
Results: The mean age at initial assessment was 6 years and 8 months (range 2 years 11 months – 9 years 9 months). Pre-SDR mean GPS was 15.67° (range 10.80°-22.50°), and post-SDR mean GPS was 12.17° (range 7.40°-20.09°), demonstrating a mean improvement of 3.50° (range 0.40°-9.80°, p<0.01). Walking speed and step length were normalised to shank length. Mean normalised walking speed pre-SDR was 0.42s-1 (range 0.19-0.70 s-1) and post-SDR this increased to 0.48s-1 (range 0.13-0.82 s-1), indicating a mean improvement of 0.06s-1 (p=0.48). Mean normalised step length pre-SDR was 1.25 (range 0.80-1.60) and this also increased post-SDR to 1.37 (range 0.79-1.80), with a mean improvement of 0.11 (p=0.35).
Conclusion: This study has shown in a select group of children with cerebral palsy gait selective dorsal rhizotomy can improve gait parameters. It also highlights the importance of patient selection for this procedure.
Introduction
Abnormal development or damage to areas of the immature brain can lead to cerebral palsy (CP). Where the motor areas are affected, this leads to problems with movement regulation. CP is the most common cause of chronic childhood disability and has a wide range of severity[1]. In Europe, bilateral lower limb spasticity is the most common type of CP[2]. Severity of CP can be classified according to the Gross Motor Function Classification System (GMFCS)[3]. In the growing child, alterations in muscle tone and control can lead to deformities and contractures. These are significantly disabling for certain children with CP, resulting in worsening of their gross motor function[3].
Selective Dorsal Rhizotomy (SDR) is a neurosurgical procedure that involves division of sensory nerves in the lower spine which contribute to increased muscle spasticity [4]. It has been utilised to treat children with CP suffering from lower limb spasticity. There have been studies which show short term improvements in spasticity[5-8] but long term functional improvements are controversial. The heterogeneity of CP may be a reason why there are conflicting results for SDR in children with CP. Nonetheless, if SDR results in functional gains in mobility, this treatment could significantly improve quality of life and independence of such children.
In the UK, National Health Service (NHS) England commissioned the use of SDR in a specific selection of children with CP as part of a Commissioning through Evaluation (CtE) programme to gather evidence about its efficacy[9]. Our aim in this study was to investigate whether SDR positively influences gait parameters for a pre-selected group of children with CP.
Methods
This is a prospective study of children undergoing SDR through the commisionging through evaluation (CtE) programme at a local tertiary centre (Queens Medical Centre, Nottingham, United Kingdom). This centre is one of five centres in the UK that are commissioned to perform SDR on children with CP for the CtE programme. The selection criteria for SDR in children with CP is detailed in Table 1[9]. SDR was performed though a single level laminectomy at the level of the conus as described by Park[4]. The dura was then opened and sensory and motor nerve roots were isolated. Electrophysiology monitoring of hamstring, adductor longus, gastrocnemius and tibialis anterior were utilised. Approximately 60-70% of sensory root was divided from L1 to S1[10].
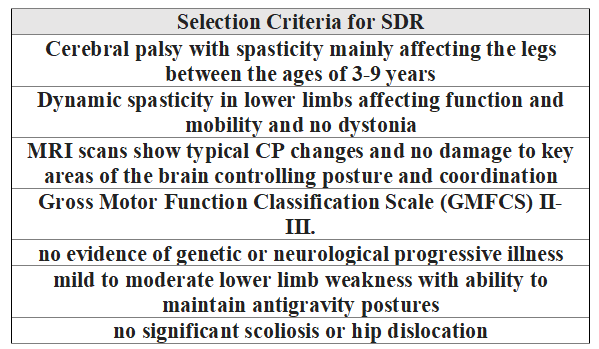
Table 1: Patient selection criteria for selective dorsal rhizotomy [11]
Gait analysis was performed at Royal Derby Hospital gait analysis laboratory. To assess gait parameters, a full kinematic gait analysis was performed on all children pre-SDR and 2 years post-SDR. 3-dimensional computerised gait analysis data was collected using a BTS (BTS S.p.A Italy) motion analysis system and a standardised marker model. The kinematic variables measured during gait analysis were used to calculate the Gait Profile Score (GPS). The GPS represents the root mean square difference of a specific set of kinematic parameters for each patient, compared with data from a local reference database and is measured in degrees of difference [12]. GPS provides an overall quantitative score for gait and is an improvement over other indices as it considers a number for gait variable scores [13]. Consequently, an improvement in GPS score following surgery would suggest an improvement in overall gait pattern, towards normal. Walking speed and step length were also recorded and investigated. In order to eliminate any improvements related to growth over the study period, these measurements were normalised to shank length. Units for walking speed therefore become s-1 (ms-1 /m), and step length becomes dimensionless (m/m). We chose to use shank length rather than height, as some children were unable to stand upright (due to weakness or flexion contractures) therefore obtaining an accurate height measurement was not possible. However, shank length can be measured in supine and is not affected by standing ability. Data analysis was performed using SPSS version 22 (IBM SPSS Statistics, IBM Inc., NY, USA). Non-parametric tests were used as the data were not normally distributed. Wilcoxon test was used to compare results and statistical significance was set at p<0.05.
Results:
A total of 13 children completed both sets of data collection (pre-SDR and 2 years post-SDR). The mean age at initial assessment was 6 years and 8 months (range 3 years 1 month – 9 years 9 months), with a male:female ratio of 9:4. The mean time from initial assessment to follow up was 28.7 months. The mean time from SDR to follow up was 24.7 months. No child received other surgical treatments between assessments.
For the whole group there was a statistically significant improvement in GPS post-SDR (Figure 1). Pre-SDR mean GPS was 15.67° (range 10.80°-22.50°), and post-SDR mean GPS was 12.17° (range 7.40°-20.09°), with a mean improvement of 3.50° (range 0.40°-9.80°, p<0.01). Examining the cohort we find that 12 out of the 13 children demonstrated an improvement in GPS following surgery.
Walking speed and step length were normalised to shank length (Table 2). Mean walking speed pre-SDR was 0.42s-1 (0.19-0.70), which increased to a mean of 0.48 s-1 (0.13-0.82 post-SDR, giving an improvement of 0.06 s-1, which was not statistically significant (p=0.48). Step length improved from a pre-SDR mean of 1.25 (0.80-1.60) to a post-SDR mean 1.36 (0.79-1.80), giving a mean improvement of 0.11m, but this again was not statistically significant (p=0.35).
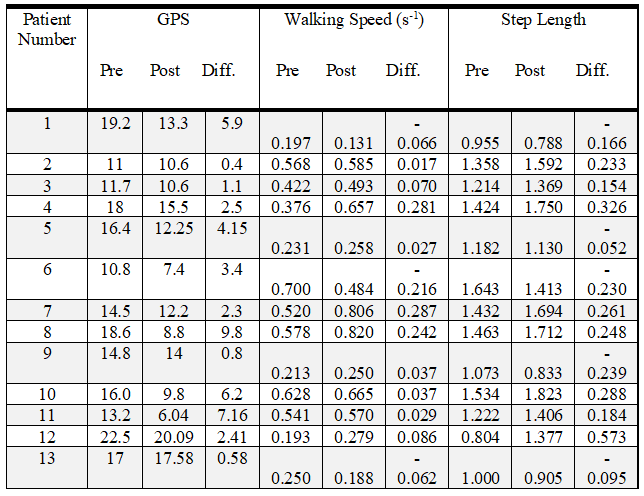
Table 2: Gait profile score, walking speed and step length results before and post-selective dorsal rhizotomy
Discussion:
SDR has been increasingly used to treat lower limb spasticity in children with CP over the last two decades. The aim of the procedure is to produce a permanent reduction in spasticity, although initially this neurosurgical procedure carried significant morbidity[14]. Improvements in its technique have shown SDR to have the potential for alleviating spasticity. SDR can decrease spasticity and increase range of motion[6, 15]. Although SDR has been performed for decades, the majority of studies assess short term outcomes and there is a lack of long term results, and very few have been randomised control trials. Most studies evaluating the outcomes of SDR include a relatively small number of children with CP. Furthermore, the outcome measures of these studies are heterogenic, with different studies assessing different indices of motor function and gait[16, 17]. A systematic review of interventions for CP by Novak et al showed that SDR did not improve general activities and participation[18]. This has been highlighted in other studies which show a variable improvement in gait and gross motor function[15, 19]. Additionally, studies have indicated that SDR does not prevent the need for any further surgical intervention [20].
The explanation for SDR’s conflicting results is multifactorial, as highlighted in a recent review article[21]. The technique involved in SDR is not standardised and since it was described by Foerster in 1908, there have been improvements on this technique. The initial technique consisted of division of all dorsal nerve roots of L2-S1, which did reduce spasticity but consequently resulted in a loss of sensation, proprioception and muscle weakness. As a consequence, the technique was altered and involved identification of specific dorsal nerve rootlets which contributed to spasticity. Current techniques use sophisticated intraoperative ultrasonography and electromyography to identify nerve rootlets which require division. Up to 70% of sensory nerve roots are divided which is now performed through a single-level approach rather than an extensive exposure that was implemented previously. A meta-analysis has shown that the greater percentage of dorsal nerve rootlets divided improves gross motor function[22]. Conversely there is a greater risk of weakness, so as low as 25% of sensory nerve roots divided has been performed[8]. The variability in SDR technique may explain why some studies have shown inconclusive results.
Studies have shown that gait disorders progress during childhood[23, 24]. In this study, we have shown that there is improvement in gait performance 2 years post-SDR. GPS was seen to decrease following surgery, suggesting an improvement in overall gait pattern towards normal. This is in agreement with other studies which have reported short term gait improvements post SDR[5, 25]. A recent study by Oudenhoven et al found that overall gait quality improved in 36 spastic diplegic children 5 years post-SDR[17]. Although not all of their patients had a diagnosis of CP, it indicated that SDR can improve gait performance in children with other causes of spastic diplegia. In our study, there was only 1 child (out of 13) whose GPS did not increase 2 years post-SDR. This child had very limited walking ability prior to surgery, which remained similar following surgery. Furthermore, he presented with some musculoskeletal complications both prior to and following surgery, and it was noted that he continued to demonstrate significant spasticity following surgery which may explain the lack of improvement.
3D gait analysis has specifically been used in the assessment of children by the Oswestry SDR programme. They reported a long-term increase in GPS post-SDR in 17 pre-selected children[20]. Specifically, they also illustrated that GPS improvements post SDR were sustained over the adolescent growth spurt. These results suggest that SDR is beneficial in improvement gait in the children with CP. However, the Oswestry programme selection criteria differ as it includes quadriplegia, severe hemiplegia and hereditary spastic paraplegia. In their cohort of 17 children, 10 children required further surgical intervention following SDR. As management of spasticity is multifactorial the outcomes of SDR are also affected by other treatment modalities, especially physiotherapy. Research has shown an improvement in outcome when physiotherapy was combined with SDR, compared with physiotherapy treatment alone. [6]. It is also difficult to eliminate the confounding factor of natural development during growth in longer term studies, which may influence results [20]. The consensus currently is that SDR should be included in the range of treatment options for consideration in the management of spasticity in children with CP.
This study investigates a specific selection of children with CP and has shown that SDR has favourable outcomes in this cohort. This study agrees with previous studies which have shown that children GMFCS I-III will gain most improvement from SDR[26, 27]. We suggest that future studies focus on patient selection as recent studies with a specific selection criteria have also shown a positive outcome[28]. However, interpretation of this should consider the natural development of gait in these very young children and a comparison group of children who did not received SDR would have helped to determine the natural development of gait in this population over time at this young age. Nonetheless SDR in the younger age group can prevent contractures and it is known that gross motor function classically improves up to the age of seven years.[29]
Limitations
Although in the study we have shown that gait performance improves post-SDR, we have no comparative data available to compare GPS over time in similar children who did not undergo SDR. Also in this study, there is a 2-year gap between assessments. Taking into account the relatively young age of the participants, some of the progression may be secondary to gait and developmental maturation. A comparison group of children who did not receive SDR could help determine its true efficacy. In this study, we only focused on gait performance and did not look into whether this had an effect on functional ability.
Conclusion
This study highlights, through the use of 3D gait analysis, that gait parameters are improved in a pre-selected group of children with CP after SDR. Patient selection is important and longer-term comparison studies are required to investigate whether improvements are maintained and to determine which children are optimal for SDR.
Level of Evidence: Level 4 (case series)
What is known about the subject
Selective dorsal rhizotomy is a neurosurgical procedure which aims to reduce spasticity in children with cerebral palsy. The procedure is not widely available in the NHS as there are conflicting long term results. NHS England have commissioned the use of selective dorsal rhizotomy in a select group of children with cerebral palsy in order to assess its effectiveness
What this study adds
This study has shown in a select group of children with cerebral palsy selective dorsal rhizotomy can improve gait parameters.
This research received no specific grant from any funding agency in the public, commercial or not for profit sectors.
Conflict of Interest:
No author has any conflicting interests
KI contributed to the statistical analysis and manuscript preparation. SC prepared the manuscript. HE performed measurements. MR performed measurements. RR produced the study design and prepared the manuscript

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org