Journal of International Research and Reviews
OPEN ACCESS | Volume 2 - Issue 1 - 2026
ISSN No: 3068-370X | Journal DOI: 10.61148/3068-370X/JIRR


Shengjun Ma, Yang Fan, Xuechuan Han*
Department of Obstetrics and Gynecology, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Yinchuan, China.
*Corresponding author: Xuechuan Han, Department of Obstetrics and Gynecology, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Yinchuan, China.
Received: May 10, 2026 | Accepted: May 16, 2026 | Published: June 02, 2026
Citation: Ma S, Fan Y, Han X. (2026) “An Unusual Cause Of Abdominal Pain In Pregancy: Spontaneous Unilateral Adrenal Hemorrhage”, Journal of International Research and Reviews, 1(2); DOI: 10.61148/3068-370X/JIRR/010.
Copyright: © 2026. Xuechuan Han. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Spontaneous adrenal hemorrhage (SAH) is a rare but life-threatening complication of pregnancy, most commonly associated with Waterhouse-Friderichsen syndrome (adrenal hemorrhage is frequently due to meningococcal sepsis.We report an unusual case of SAH in a 30-year-old primigravida at 36 weeks and 3 days of gestation with no history of typical risk factors. The patient presented with sudden onset severe abdominal pain, nausea, and vomiting. Imaging studies revealed an 14.9×10 cm adrenal haemorrhage with no obvious mass or lesion underlying it. Emergency cesarean section.Interventional radiology were undergoed, and the patient was managed in the intensive care unit with blood transfusion and supportive care. She recovered without complications. This case highlights the importance of early recognition of SAH even in the absence of typical risk factors. Prompt diagnosis, multidisciplinary management, and timely surgical intervention are critical to improving maternal outcomes in this rare condition.
Spontaneous Adrenal Hemorrhage, Pregnancy Complication, Abdominal Pain in Pregnancy
The adrenal glands are a pair of endocrine organs located in the retroperitoneum on the upper poles of the kidneys.The suprarenal glands are one of the most well-perfused organs in the human body.Adrenal hemorrhage represents a rare disease of variable etiologies.Adrenal hemorrhage is an uncommon disorder characterized by bleeding into the suprarenal glands. The hematoma may be unilateral or bilateral.The clinical presentation can range from nonspecific abdominal pain to catastrophic cardiovascular collapse [1][2][3][4][5]. Furthermore, most cases of SAH at or near term have presented with gross haemodynamic instability, resulting in emergent caesarean delivery or intrauterine fetal death.
Since SAH is uncommon, The incidence of SAH has been reported from 0.14% to 1.1% and it usually involves the right gland. During pregnancy, idiopathic unilateral SAH has been reported rarely. The incidence of this condition during pregnancy is unknown. the optimal mode of delivery for those women in whom SAH occurs without haemodynamic instability is equivocal. We present a case of acute SAH at term.
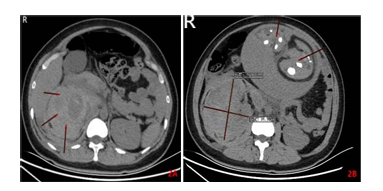
A 30-year-old gravida 1, para 0 presented to the birth suite of a peripheral centre at 36+3 following the acute onset of right-sided abdominal pain. Her pain was constant, sharp in nature, 7/10 in severity and located in the right upper quadrant with radiation into her back. She had associated nausea and four episodes of emesis but otherwise no headache, visual changes or history of elevated blood pressure. Her pregnancy had been otherwise uncomplicated. She had no history of pregnancy. On examination, her blood pressure was 98/74 mm Hg, pulse rate 122 bpm, temperature 36.9°C and oxygen saturation equal to 98% on room air. Her abdomen and uterine fundus were soft, with tenderness only in the left upper quadrant and flank. The uterine fundus was equivalent to her dates and fetal movements were felt. She had no vaginal bleeding and she was not contracting. Her cardiotocography was normal. Formal urine microscopy and culture was unremarkable, and she had no proteinuria. Full blood examination, renal function test, liver function test, inflammatory markers and coagulation studies were normal. She had a duplex Doppler of both lower limbs which was negative for deep vein thrombosis.An obstetric ultrasound confirmed fetal well-being. Abdominal ultrasound revealed a 19.3×6.3cm mass in the right upper quadrant thought to be either a degenerative fibroid or an adrenal mass pathology. This was followed by an CT which revealed an 14.9×10 cm adrenal haemorrhage with no obvious mass or lesion underlying it (figure1). Differential diagnosis:Adenoma, phaeochromocytoma, carcinoma, adrenal vein thrombosis, placental abruption, pyelonephritis, trauma, eclampsia/pre-eclampsia, embolism.
Figure1
Vaginal examination found her cervix to be 0 cm dilated and 2.5 cm long. A multidisciplinary team discussion was conducted and it was decided that she was suitable for cesarean section.During operation her Hb dropped to 76 mg/dL and she was transfused with 2 units of red blood cells.Given the evidence of ongoing bleeding, a second multidisciplinary team discussion was held. Interventional radiology were undergoed after cesarean section.Angiography and embolization of the bleeding lesion provided better outcomes.During follow-up in the Endocrine clinic after 3 months, additional tests were sent (cortisol level after 1 mg dexamethasone suppression test and repeated metanephrines), which were noted all to be negative. An abdomen CT was scan was performed and showed interval resolution of the previously seen right adrenal mass (Figure 2), which was likely representing pregnancy-related non-traumatic hemorrhage. The patient was counseled about her condition and reassured.
Figure2

Discussion
Adrenal hemorrhage is a relatively rare disorder, estimated to be present in roughly 0.14% to 1.8% of postmortem examinations.Overall, it is associated with a 15% mortality rate, which varies according to the severity of the underlying cause of hemorrhage. A 55-60% mortality rate has been reported in patients with Waterhouse-Friderichsen syndrome (adrenal hemorrhage is frequently due to meningococcal sepsis)[5][6]. However, the incidence may be much higher since the vague presentation, associated comorbid conditions, and variable lab findings can make diagnosis difficult.The exact pathophysiology of acute adrenal hemorrhage remains uncertain. It has been hypothesized that certain specific anatomic and physiological characteristics predispose to bleeding into the adrenals.
Adrenal hemorrhage can present in a myriad of clinical contexts, and diagnosis remains challenging. Disease familiarity and a high index of suspicion are required for early diagnosis and prompt treatment. Since critically ill individuals represent a subset of patients who are at risk of developing adrenal hemorrhage, early recognition is crucial in these subsets of patients. Most cases are discovered incidentally, however, nonspecific abdominal, or loin pain is an important presenting symptom. Other nonspecific symptoms include malaise, weakness, lethargy, nausea, vomiting, and diarrhea. Symptoms may correlate to the severity of hemorrhage, with extensive bilateral hemorrhage heralding the development of acute adrenal insufficiency.The examination may reveal signs of exsanguination, such as tachycardia and hypotension, or nonspecific findings like abdominal or flank tenderness [7][8][9][10].
Most patients have normal lab parameters, just as our case,possibly reflecting minor adrenal bleeding.Imaging remains the most important diagnostic tool, with computed tomography scan being an important modality. The appearance of imaging varies with the age of the hematoma. Adrenal hemorrhage on computed tomography scan appears as a round-to-ovoid lesion. There may be peri-adrenal fat stranding, and bleeding may extend into the peri-nephric space. Fresh hematomas demonstrate high attenuation, which decreases over time. Ultrasonography is the modality of choice in infants due to their small bodies and relatively large adrenal size.Magnetic resonance imaging (MRI) is the most accurate diagnostic modality. It can differentiate acute from chronic hematomas and ascertain an underlying tumor's presence.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org