International Surgery Case Reports
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Mohammadreza Emamhadi, 1,2, Fereshteh Arbabi-Bakhshayesh2,3*
1Department of Neurosurgery, Guilan University of Medical Sciences, Rasht, Iran.
2Nerve Repair and Limb Reconstruction Clinic, Rasht, Iran.
3School of medicine, Guilan University of Medical Sciences, Rasht, Iran.
*Corresponding author: Fereshteh Arbabi-Bakhshayesh, 3School of medicine, Guilan University of Medical Sciences, Rasht, Iran.
Received: April 05, 2026 | Accepted: May 20, 2026 | Published: May 25, 2026
Citation: Emamhadi M, Fereshteh A Bakhshayesh. (2026) “Nerve Transfer for Lumbosacral Plexus Injury: A Case Report”, International Surgery Case Reports, 8(2); DOI: 10.61148/2836-2845/ISCR/115.
Copyright: © 2026. Fereshteh Arbabi-Bakhshayesh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective: Lumbar plexus injuries result in lower limb paralysis, having devastating impacts on quality of life. In cases in which there is residual adductor function, a nerve transfer can restore more important muscle function. The purpose of this report is to describe the successful restoration of knee extension through a distal nerve transfer from the anterior branch of the obturator nerve to branches of the femoral nerve.
Methods: We describe a 19-year-old man with a right lower limb amputation and nearly complete left lower limb paralysis due to a lumbosacral plexus injury after a traffic accident. Since adductor function remained intact in the left thigh, we transferred the anterior branch of the obturator nerve to selective branches of the femoral nerve to reconstruct the quadriceps femoris muscle. A prosthetic leg was fitted for his amputated right limb.
Results: Adductor function remained intact throughout the recovery period. After 12 months, quadriceps strength reached grade M4, and he was able to walk independently.
Conclusion: In a lumbosacral plexus injury, the remaining strength can provide an opportunity to restore key muscle function through nerve transfer. The obturator nerve proved to be a safe donor. This case demonstrates that even in severe bilateral lower limb injuries, residual motor abilities can be utilized to restore meaningful function.
Lumbosacral injury, Femoral nerve palsy, Nerve transfer, Obturator nerve, Quadriceps reinnervation, Peripheral nerve surgery
Objective
Injury to the lumbosacral plexus can lead to lower limb paralysis and significantly limit mobility and quality of life. Conservative management may allow spontaneous improvement; however, functional restoration often remains limited, particularly in severe injuries. Surgical nerve transfers can help restore key muscle functions. The femoral nerve is critical for hip flexion and knee extension, and injury to the nerve can substantially impair walking and daily activities. When the obturator nerve is spared and available for distal nerve transfers, an obturator-to-femoral transfer provides shorter regeneration distances, faster recovery, and minimal donor-site morbidity, making it an effective treatment option.
Here, we describe a patient who suffered a severe lumbosacral plexus injury in the left lower extremity. On examination, all muscles in the left lower limb were paralyzed except for the hip adductors, which retained moderate strength (3/5 on the MRC scale). The right lower limb was amputated above the knee. An obturator-to-femoral nerve transfer was performed to restore quadriceps function, and a prosthesis was fitted for the amputated limb.
After completing a structured course of occupational therapy, the patient was able to walk independently.
2. Case Report
2.1 History and Examination
A previously healthy 19-year-old man was referred to our center five months after sustaining injuries in a motor vehicle collision. He had undergone an above-knee amputation of the right leg, and exhibited complete paralysis of the left lower limb. On examination, all muscle groups in the left leg were non-functional except for the hip adductors, which showed moderate strength (MRC grade 3/5). Sensation was absent throughout the limb, and the overall findings suggested an almost total injury to the lumbosacral trunk. After evaluating his neurological condition and treatment options, we elected to perform a nerve transfer. The anterior branch of the obturator nerve was used as the donor to reinnervate the rectus femoris and vastus lateralis branches of the femoral nerve (Figure 1).
2.2 Surgical Technique
With the patient in the supine position, a longitudinal incision was made just lateral to the palpable femoral artery to expose the femoral nerve. The motor branches supplying the rectus femoris and vastus lateralis were identified as the target nerves and subsequently transected. A second longitudinal incision was created along the proximal medial thigh to isolate the anterior branch of the obturator nerve, which was selected as the donor (Figure 2). Intraoperative stimulation confirmed robust muscle contraction, verifying the donor nerve’s functional integrity. The anterior branch of the obturator nerve was then divided and tunneled subcutaneously toward the femoral nerve. Under microscopic magnification, end-to-end coaptation was performed between the donor and recipient branches using 10-0 monofilament sutures.

Figure 1. Preoperatively, the patient presented with right leg amputation and left leg paralysis. Adduction function was preserved in the injury. Video available at https://drive.google.com/file/d/13hEOHNMqHa42jSeQiugWhkebGcnz3ZgC/view?usp=sharing
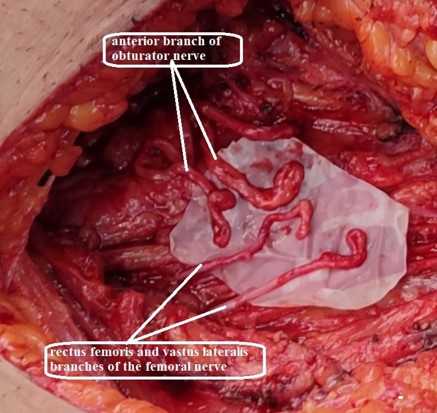
Figure 2. The distal stumps of the femoral nerve and the proximal stumps of the obturator nerve were prepared for coaptation.
2.3 Postoperative Course
Postoperatively, the patient’s lower limb was maintained in extension within a splint for four weeks, after which physical therapy and motor reeducation were initiated. Cortical reeducation focused on pairing active hip adduction with passive knee extension. Adductor strength remained preserved throughout the rehabilitation period. EMG studies demonstrated early reinnervation of the vastus lateralis and rectus femoris at five months. By seven months, quadriceps strength had improved to MRC grade 3, reaching M4 by the twelfth month postoperatively. Once the patient achieved active knee extension with stable M4 strength, an ankle–foot orthosis was provided for the left limb, and a prosthesis was fitted for the right lower extremity. Following a structured occupational therapy program, he regained functional independence and was able to ambulate for daily activities (Figures 3, 4).

Figure 3. Patient was able to extend his left leg with a strength of 4 out of 5 (Medical Research Council grade) 12 months post-surgery. A prosthetic limb was fitted for the right lower extremity. Video available at https://drive.google.com/file/d/1-cocncT6OcvCOqKWrIrEaCc-RvKgzyx_/view?usp=sharing

Figure 4. Patient was able to walk independently 12 months post-surgery. Video available at https://drive.google.com/file/d/1XK9wwnXMG94v0EODazrAfpTQ8bxzYBLy/view?usp=sharing
3. Discussion
The lumbosacral plexus is essential for lower limb movement; therefore, injury to these nerves can significantly impair a patient’s quality of life. Recovery following such injury is variable and depends on the severity of the lesion as well as the chosen treatment strategy. Conservative management has traditionally been preferred, as spontaneous complete or incomplete recovery may occur in some patients, and surgical intervention can be challenging and carries a risk of morbidity (1, 2). However, the potential value of surgical treatment should not be overlooked. Although restoration of distal foot function may be unattainable in severe injuries, reinnervation of a few proximal key muscles in the leg can dramatically enhance functional outcomes, allowing patients who might otherwise remain wheelchair-bound to regain the ability to stand and walk independently (2). Spontaneous recovery may occur; its onset can range from 3 months to up to 4 years after the injury. However, postponing surgery in hopes of natural recovery may negatively affect the final outcome. Motor endplates start to degenerate approximately 12 to 18 months after denervation; therefore, earlier intervention is associated with better functional recovery (3-5).
The femoral nerve arises from the posterior divisions, and the obturator nerve from the anterior divisions, of the L2–L4 nerve roots. This anatomical separation occurs within the psoas major muscle, causing each nerve to follow a distinct course through the pelvis. Consequently, in lumbosacral plexus injuries that selectively involve the posterior divisions—such as those caused by trauma, tumors, or localized compression in the retroperitoneal or pelvic region—the femoral nerve may be affected, while the obturator nerve, originating from the anterior divisions, might remain intact. The femoral nerve is the largest branch of the lumbar plexus and innervates the quadriceps muscles, which are essential for knee extension. As a result, injury to this nerve can limit walking and greatly affect quality of life. Femoral nerve function can be restored either proximally at the lumbosacral plexus level or distally at the thigh to target the key motor branches. Proximal reconstruction can be done employing contralateral S1 nerve root transfer, as described by Li et al., or utilizing a sural nerve graft, as reported by Tung et al. Both approaches aim to restore proximal muscle strength and improve hip and knee stability (7, 8).
In contrast, distal reconstruction focuses on repairing or reinnervating the femoral and obturator nerves at the thigh level, which has been associated with greater MRC improvement regardless of whether neurolysis, grafting, or nerve transfer is performed (1). While proximal approach has been described in the literature (7, 8), in our experience, this may increase the risk of bleeding and skeletal instability following the primary trauma. Therefore, in this case, our surgical strategy focused on restoring femoral nerve function through a safer, more distal approach.
The choice of surgical management depends on the severity and location of the injury. Reconstructive options include direct end-to-end coaptation, nerve grafting, and nerve transfer. Direct coaptation is rarely performed, as the gap between the proximal and distal nerve ends is usually too large for a tension-free repair (9). Although controlled trials comparing nerve grafting and nerve transfer are lacking, clinical experience and accumulating evidence suggest that nerve transfer can offer better and faster outcomes in appropriately selected cases. The main advantage of distal nerve transfer lies in its single, tension-free coaptation site positioned close to the target muscle, compared with two coaptation sites in a nerve graft. Fewer suture lines minimize ischemic risk, scar tissue, and axonal loss, and reduce regeneration distance and time to reinnervation (9). Inaba et al., O’Brien et al., and Duraku et al. have all reported that nerve transfers achieve faster and more reliable results than nerve grafting, especially when the gap between the injury and target muscle is long (3, 5, 10).
Timing of surgery is another factor that influences the outcome. After injury, the distal segment undergoes Wallerian degeneration, and axonal regrowth proceeds at about 1 mm per day. In proximal lesions, this slow regeneration rate can lead to irreversible motor endplate atrophy if reinnervation is delayed (5). Significant recovery, when it occurs, is usually seen when surgery is performed within six to seven months after the injury and is less likely in complete palsies (4).
The obturator nerve (ON), particularly its anterior branch, is the most common donor for femoral nerve palsy (3, 11). Although it contains fewer axons than the femoral nerve, both experimental and clinical data support its adequacy for reinnervation (4, 12). Campbell et al. used the entire ON to maximize axonal input, while others have achieved comparable outcomes using only partial transfers, suggesting that full sacrifice of the nerve may not be necessary (3, 9). A cadaveric study by Tung et al. confirmed the technical feasibility of tension-free coaptation while preserving the posterior branch (6).
Recent systematic reviews reinforce these findings. Lee et al., in a review of 18 studies including 40 patients, reported that the obturator nerve was the donor in 94% of cases (55% anterior branch), with 79% achieving at least MRC grade 4 strength. Earlier surgery—within six months—was linked to better outcomes, and no donor-site gait impairment was observed (11). Similarly, Duraku et al. reported favorable recovery (MRC grade ≥3) in nearly all 21 patients within 10–18 months, using the anterior branch of the ON in most cases (3).
In our case, no donor-site morbidity was noted, and the patient regained sufficient knee extension for walking and stair climbing, though running remained limited. This is consistent with our previous experience and prior reports noting transient, self-resolving adduction weakness (12-15). Preservation of the adductor magnus and the dual innervation of the adductor brevis likely explain this maintained function (4).
Overall, obturator-to-femoral nerve transfer is a safe and effective method for restoring quadriceps function in femoral nerve palsy. Its advantage including shorter regeneration distance, faster recovery, and minimal donor-site morbidity, make it a strong alternative to nerve grafting, especially in extensive or proximal injuries (11).
4. Conclusion
Obturator-to-femoral nerve transfer is a reliable reconstructive option for patients with severe lumbosacral plexus injuries when the obturator nerve remains functional. In this case, early intervention within six months, combined with preservation of the hip adductors, enabled successful reinnervation of the quadriceps without donor-site morbidity. Given that the obturator nerve may retain function even in extensive lumbosacral plexus injuries, it should be carefully and repeatedly assessed, as it can serve as an excellent donor for restoring knee extension.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org