International Surgery Case Reports
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Rafael Dominguez Sampaio Menezes1, Wagner Ramos Borges2*
15th year medical student and supervisor of monitors in the curricular component Regional Applied Anatomy/Medicine, Bahiana School of Medicine and Public Health, Salvador, Bahia, Brazil.
2PhD in Medicine and Health / Faculty of Medicine of Bahia of the Federal University of Bahia; Vascular Surgeon, General Surgeon, CEO Vivasc Angioclínica de Salvador, Bahia, Brazil.
*Corresponding author: Wagner Ramos Borges, PhD in Medicine and Health / Faculty of Medicine of Bahia of the Federal University of Bahia; Vascular Surgeon, General Surgeon, CEO Vivasc Angioclínica de Salvador, Bahia, Brazil.
Received: May 05, 2026 | Accepted: May 16, 2026 | Published: May 20, 2026
Citation: Sampaio Menezes RD, Wagner R Borges. (2026) “Access Vascular for Hemodialysis in Children and Adolescents: Comparative Profile Between the Use of Catheters and Arteriovenous Fistulas in Brazil.”, International Surgery Case Reports, 8(2); DOI: 10.61148/2836-2845/ISCR/117.
Copyright: © 2026. Wagner Ramos Borges. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Vascular access for hemodialysis constitutes a fundamental component in the treatment of children and adolescents requiring renal replacement therapy. Among the main modalities used, arteriovenous fistula and central venous catheters of short and long duration stand out, and their selection may vary according to clinical characteristics, patient age, and availability of healthcare resources. The analysis of the utilization profile of these accesses helps to understand the pattern of care provided and to identify differences in clinical practice, contributing to the development of strategies that promote better quality of care for pediatric patients undergoing hemodialysis. Objective: This study analyzed and described the temporal trend in the use of vascular accesses for hemodialysis in children and adolescents in Brazil between 2015 and 2024, in addition to estimating the frequency of arteriovenous fistula, short-term catheter, and long-term catheter use during the period, and describing the variables that influence the utilization of these accesses. Methods: This is an observational, descriptive, and retrospective time-series study, carried out using secondary data obtained from the Outpatient Information System of the Brazilian Unified Health System (SIA/SUS), available at the Department of Informatics of the SUS (DataSUS). Records of procedures related to vascular accesses for hemodialysis in individuals aged 0 to 19 years were analyzed, considering the variables of procedure type, age group, sex, region of residence, and year of registration. A descriptive analysis of the absolute and relative frequencies of the procedures over the studied period was performed. Results: During the analyzed period, 148,819 procedures. Arteriovenous fistula was the most frequently performed type of access, corresponding to 46.6% of the procedures, followed by long-term catheters (30.2%) and short-term catheters (23.1%). Regarding regional distribution, a higher concentration of procedures was observed in the Southeast and Northeast regions, which together accounted for the majority of records during the analyzed period. In terms of demographic characteristics, a predominance of males (52.7%) was observed compared to females (47.3%). Regarding age group, the highest frequency of procedures occurred in the 15–19-year age group, while younger age groups had fewer records. A low prevalence of infections was observed, with positivity rates of 0.1% for HBsAg and 0.3% for HIV, with a slight predominance among patients using catheters. The hospital mortality rate was 0.65%, with a decreasing trend over the analyzed period, and higher rates observed in younger age groups, particularly among patients under 1 year of age. Conclusion: The study showed that arteriovenous fistula was the most commonly used vascular access for hemodialysis in children and adolescents in Brazil; however, a reduction in its use was observed over the analyzed decade, indicating the need to strengthen strategies to expand access to fistula creation in the pediatric population.
Catheters. Arteriovenous Fistula. Renal Dialysis
The term dialysis is derived from Greek, through the union of the words “dia”, whose meaning is “through”, and “lysis”, which means “to loosen or divide”. Dialysis is a solution found for renal replacement therapy, in which an extracorporeal artificial equipment performs the role of the kidney in filtering blood, removing solutes/toxins and excess water.1 This procedure is widely usedo to maintain homeostasis in individuals who present rapid loss of kidney function, as in acute kidney injury (AKI) or prolonged loss, as in chronic kidney disease (CKD).1
Furthermore, the global incidence of kidney failure is increasing e consequently, the number of dialyses also grows – as it emerges as a transitional therapy during the waiting period for kidney transplant, due to the insufficient supply of organs.2,3 Hemodialysis is the most common form of dialysis, representing 89%, while peritoneal dialysis accounts for the other 11%.2 Worldwide, more than 2 million patients require hemodialysis (HD), a procedure lasting 3 to 4 hours per day, usually 3 times a week.4 NIn Brazil, the total number of patients in chronic dialysis in 2019 was estimated at 139,691, and of these, 93.2% were on hemodialysis, meaning they used vascular access.5
Thus, the dialysis patient needs a functional vascular access (VA) that meets their medical needs. The main forms of VA for hemodialysis include dialysis catheters – which can be tunneled, indicated for long-term use (Perm-cath) or non- tunneled, used as short-term access (Sorensen e Hickman) – or arteriovenous fistulas (AVFs), autologous grafts in which the vein is anastomosed to the patient's own artery.6
According to the protocol of the Kidney Disease Outcomes Quality Initiative (K/DOQI), updated in 2019, AVFs should be prioritized as initial vascular access. The aforementioned document warns about the increase in morbidity and mortality in adult patients using central venous catheters (CVCs). However, in 2019, the International Pediatric Hemodialysis Network reported that in 552 children from 55 dialysis centers in 27 countries, the vascular access used was a CVC in 404 patients, representing 73% of the sample.7 This demonstrates that the majority of pediatric patients still start hemodialysis via CVC compared to AVFs.8
The AVF was first described by Brescia and collaborators (1966) and is still considered the "gold standard" access for hemodialysis.9,10 Since the 1990s, the main guidelines encourage the creation of AVFs whenever possible in dialysis patients.11 The main advantage of AVFs over catheter placement is precisely their entirely autogenous nature, which minimizes the main concern with other types of vascular access, which is infection.6
The first attempts at AVFs in children reported an immediate failure rate of 50%, however, over the years, there have been advancements in technique and, especially, an increase in surgical experience. In the study conducted by Chand (2019), the results showed that after 6 months, only 5% of pediatric patients dialyzed via AVFs developed infection, while in those dialyzed via CVCs, this rate reached about 36%, making the investigation even more necessary when choosing the type of vascular access for these individuals..10
Regarding CVCs, in addition to their short lifespan, there is a consensus in the literature regarding possible complications, such as gas embolism, occlusion, thrombosis, malfunction, and infection. However, they offer benefits, such as immediate access – without maturation or healing time–, the absence of the need for needle cannulation, the greater ease of placement, and the fact that they present a good prognosis as a temporary solution in patients with small caliber vessels (especially children weighing less than 10kg).6,10 In other words, despite the benefits that AVFs demonstrate ,CVCs still have clinical importance , being indicated bythe K/DOQI in some situations.a K/DOQI in some situations.8
Even after major advancements in hemodialysis treatment worldwide, achieving vascular access without complications remains one of the biggest challenges in the care of nephrology patients. According to the systematic review conducted by Hidalgo-Blanco and collaborators (2023), this problem is responsible for more than 15% of hospitalizations of patients on HD. Furthermore, the authors conclude that reducing these rates is essential for treatment to continue evolving and becoming increasingly effective for patients.12
Pediatric patients on HD face particular challenges in obtaining AV, due to reduced physical size and limited availability of specific devices for this age group. Furthermore, the need for hospitalization for sedation increases the risk of hospital infections, such as those caused by Staphylococcus, E. coli and other gram-negative bacteria.7,13
Thus, despite the initiative “fistula first” developed bya K/DOQI, in its 2006 update, and the information previously presented about AVFs and catheters, the choice of AV for hemodialysis is still challenging and specific to each individual, especially for the pediatric population. In this context, the present study aims to analyze the profile of AVs used in a population little evaluated in the country, in order to expand knowledge on the subject and provide subsidies that can assist in clinical practice and in planning the choice of AV in this population.
Acute and chronic kidney failure is a disease that has accompanied humanity since its beginnings. In ancient Rome and later in the Middle Ages, treatments – archaic and rudimentary – included hot baths, sedation therapies, bloodletting, and enemas.14 The journey to reach the relative popularization of dialysis treatment that exists today was long and full of obstacles. It began in the 19th century, with the first scientific descriptions by Scottish chemist Thomas Graham, titled "father of dialysis".11,14
The global increase in chronic diseases, driven by population aging, includes CKD, which presents high morbidity and reduces patients' quality of life. Treatment can be done by HD, peritoneal dialysis, or kidney transplant, with HD being the most common, used by 88.2% of patients on renal replacement therapy, according to the 2023 Brazilian Society of Nephrology Census.15
In the United States of America (USA)), end-stage renal disease is a reality not only for adults and the elderly, but also for pediatric patients and adolescents.. Today, there are over 400,000 patients in the US on dialysis, which means 62 million dialysis sessions annually. According to the Centers for Disease Control and Prevention, nearly 10,000 of them are children, 60% of whom are on HD.3,7
Kidney transplantation is the first choice in the pediatric population facing end-stage renal disease and requiring renal replacement therapy; however, it is known that the number of individuals who would need a new kidney is much higher than its availability. Therefore, while on the transplant waiting list, they start dialysis – thus requiring an AV for this procedure.16
The ideal access is one that can be obtained easily, provides adequate flow, has good durability, and presents a low rate of complications. The choice should be guided by an adequate evaluation including history of previous use of central and peripheral accesses, in addition to a detailed physical vascular examination.17 The patient's choice and experience, often lost and ignored in the challenging management of end-stage organ failure, must remain central as we focus on patient-centered care of the AV and view it individually.4
Furthermore, discussing the catheters short term, these are recommended for situations acute and for insertion percutaneous at the bedside. The sites of preference for insertion venous are right jugular, femoral, left jugular, and, as a last choice, subclavian, preferably on the non-dominant side – mainly due to the risk of central venous stenosis. Additionally, when choosing the puncture site, one must also consider preserving the vessel for future creation of fistula arteriovenous.17
As for long-term catheters, there are two types: totally implantable and semi-implantable ((perma-cath). Both options are indicated in patients requiring dialysis therapy for more than one week and who do not yet have an arteriovenous fistula. They are indicated for patients with multiple comorbidities, elderly patients, with unfavorable vascular anatomy, or with limited life expectancy. The right internal jugular vein is the preferred site for implantation.17
Non- tunneled catheters are used in critically ill patients and are designed for short-term dialysis. Typically, these catheters need to be removed before hospital discharge due to the risk of catheter dislodgement and infection. On the other hand, tunneled catheters can be used for long-term HD and feature the internal jugular vein as the preferred access vessel. The subcutaneous tunnel is sealed by a cuff to reduce the risk of infection and catheter dislodgement.2 This cuffto has a subcutaneous retention function, allowing tissue growth, acting as an antimicrobial barrier and an anchor. Short-term catheters do not have this cuff and therefore have a higher risk of dislodgement and developing infectious complications.6
A AV Fistula is the access of choice for patients undergoing chronic HD, as it requires less maintenance e andis associated with lower morbidity and mortality. The surgical technique for an AVF consists of the anastomosis between the lateral wall of the artery and the lateral wall of the vein, or the lateral wall of the with the end of the vein. In order of preference, are indicated the veins radiocephalic, then the brachiocephalic, followed by the brachiobasilic. This procedure is performed in the surgical center under regional or local anesthesia and the evaluation prior of the patient by the nephrologist and vascular surgeon is fundamental, based on the “Fistula First” initiative developed bya K/DOQI. This guideline concerns the creation of the AVF in a preemptive manner with a view to reducing the complications inherent to the chronic process of therapy, the risks of infections e and recurrent hospitalizations, which can generate a great impact on the morbidity and mortality of these patients. It is considered as fistula ideal that located as distal as possible possible in the upper limb not dominant, mainly for preservation of the vessel in future interventions.17
The preferred sites for AVF placement include, in order, radial artery to cephalic vein (radiocephalic), brachial artery to cephalic vein (brachiocephalic) and brachial artery to basilic vein (brachiobasilic, with or without transposition).10 In fistulas, the cephalic vein is the preferred outflow vein, as it typically does not require transposition and is easier to cannulate due to its superficial location.6
The K/DOQI guidelines emphasized the need to increase the use of AVFs. Unfortunately, comorbid disease processes and late referrals for AV have maintained our reliance on synthetic grafts and catheters. Late referrals end up compromising the choice of fistula, this happens due to the healing period required after AVF creation, which can last up to 6 months.18
The AVF is often considered the "gold standard" for hemodialysis access because it demonstrates the best overall performance, is associated with fewer infections and therefore fewer hospitalizations, and tends to last longer than other types of AV.19 Generally, most articles found in previous reviews by Hidalgo-Blanco MA and collaborators highlight that complication rates in AVFs are very low, around 1.14 per access year. Results reinforced by those investigations that also compared the incidence of complications between different access routes for HD, with AV suffering the fewest potential complications.12
Regarding complications related to AV, oneof the main morbidities related to CVC, due to its high incidence, is infection, with sepsis being the most important. A study with patients enrolled in the United States Renal Data System (USRDS) discovered that 29.8% of patients developed sepsis, with the highest rate in those using a CVC for HD. Furthermore, it was observed that patients presented a higher number of comorbidities associated and advanced age.20 USRDS data showed that sepsis rates associated with CVCs are approximately 80 per 100 patient-years, compared to only 10 per 100 patient-years for AVFs.10
The increase in catheter use by elderly patients was evidenced, which is related to high rates of infections and worse survival. This increase in their use has been associated with a rise in mortality. However, in elderly patients, it is not clear if the increase in mortality is due to the catheter or the patient's baseline characteristics.20 One way to analyze and compare these findings is through comparative analysis with younger populations, such as the pediatric population, since, in summary, they present fewer comorbidities and underlying diseases.
Regarding sex, it is found that women present lower maturation rates; have reduced rates of primary, primary assisted, and secondary patency; require more procedures per capita to achieve maturation and maintain fistula patency; are more likely to receive dialysis via an arteriovenous graft or central venous catheter; and require more time and potentially more invasive assistive interventions to achieve a mature fistula.21
The Centers for Medicare & Medicaid Services (CMS) introduced the “Fistula First” initiative in 2003, with the aim of achieving the K/DOQI guidelines. These guidelines recommend an AVF rate of 50% in all incident HD patients and a prevalent AVF rate of 40% in adult HD patients. HDThis was not extrapolated to the pediatric population. However, if the goal is to provide the best possible access for HD, an AVF needs to be considered in all pediatric HD populations as well.10
Despite the aforementioned regarding the “Fistula First” initiative, the pediatric nephrology community in the USA uses central venous catheters as the primary dialysis access for most patients.10 Thus, the analysis of the AV choice profile for HD in Brazil becomes necessary for comparison between countries.
Numerous reports of successful creation of AVFs in children have been documented worldwide, with primary failure rates as low as 5%. Maturation time can be prolonged, with reports of up to 6 months. Therefore, advance planning should be done to allow time for maturation and/or revision if necessary.10
The development of a native AVF is the preferred access route for pediatric HD patients with the best success rate and the lowest incidence of complications. When the AVF cannot be created or utilized, CVCs without cuffs may be suitable as vascular access with guidewire exchange until stabilization of the long-term access route. The transhepatic CVC can be used as an for long-term use in pediatric patients with exhausted classic venous access routes.22
The importance of patient self-care with the catheter at home is highlighted, requiring proper guidance so that they can identify signs of infection and seek healthcare services in a timely manner. Early recognition of the signs flogistical, in addition to granting the individual autonomy in vascular access care, contributes to the prevention of infections, such as sepsis and endocarditis, since central vascular access allows rapid access of microorganisms to the systemic circulation.5
Even after major advances in the field of hemodialysis treatment worldwide, obtaining uncomplicated vascular access remains one of the greatest aspirations in the care of nephrological patients; it is estimated that more than 15% of hospitalizations of patients undergoing HD are due to problems arising from AV.12
Objectives
To describe vascular access for hemodialysis in children and adolescents up to 19 years of age in Brazil between 2015 and 2024.
Methods
An observational and descriptive study conducted using secondary data.
This study was conducted within the territory of Brazil. Brazil has a land area of approximately 8.5 million square kilometers, making it the largest country in South America and the fifth largest in the world by land area. Administratively, it consists of 26 states and the Federal District, organized into five major geographic regions: North, Northeast, Central-West, Southeast, and South.23
The period analyzed was from January 2015 to December 2024, a span covering a full decade, allowing for the assessment of trends and variations over time.
All records of children and adolescents—according to the Ministry of Health’s age classification (0 to 19 years) undergoing hemodialysis using temporary or permanent vascular access via catheters and arteriovenous fistulas were included. Procedures with generic codes or without specification of the type of vascular access were excluded from the comparative analysis.
The data were obtained from the SUS Outpatient Information System (SIA/SUS), hosted on the DATASUS website (http://www.datasus.gov.br), extracted and tabulated using Tabwin software (version 4.15), developed by DATASUS for statistical analysis. Records corresponding to ATD – APAC Dialysis Treatment, registered between 2015 and 2024, were selected.
Tabulations were performed in Tabwin based on the following variables:
• Type of procedure (AVF, short-stay catheter, and long-stay catheter);
• Age group (<1 year, 1–4 years, 5–9 years, 10–14 years, and 15–19 years);
• Gender (Male and Female);
• Regions of Brazil (North, Northeast, South, Southeast, and Midwest);
• Infections (HBsAg and HIV)
• Year of processing (2015–2024);
The data extracted using Tabwin (version 4.15) were transferred to Microsoft Excel (version 16.32), where they were analyzed and presented in tables and graphs created in the same program. Initially, a univariate descriptive analysis of the categorical variables was performed by calculating absolute and relative frequencies (%). In addition to applying measures of central tendency (mean) and dispersion (standard deviation), a normality test was conducted using the Shapiro-Wilk test to verify the normality of the variable. To verify the temporal trend, linear regression was used. To verify the association between the categorical variables, the chi-square test of independence (X²) with one degree of freedom was used. A p-value of <0.05 was adopted as the level of significance. Inferential analyses were performed using the OpenEpi® statistical tool (Open Source Epidemiologic Statistics for Public Health, version 3.01), available free of charge online.
This study utilized secondary data in the public domain, extracted from the SUS Outpatient Information System (SAI/SUS) database, available on the DATASUS website, which is anonymized and freely accessible. Thus, there is no risk of individual patient identification or direct collection of personal information.
Since this is a study that uses only public and aggregated data, it was not necessary to submit it to the Research Ethics Committee.
Nevertheless, this study adhered to the ethical principles of scientific research, ensuring the responsible and judicious use of information, in accordance with the precepts of research ethics and the General Data Protection Law (Law No. 13,709/2018), even though the data used are already anonymized.
Results
During the analyzed period, 148,819 procedures were recorded. It was observed that the AVF was the most frequent type of access, accounting for 46.6%, followed by long-term catheters at 30.2% and short-term catheters at 23.1%. (Table 1)
Data analysis revealed that the annual arithmetic mean for AVFs was 6,938.5 ± 1,128 procedures per year, for short-stay catheters it was 3,456.1 ± 300 procedures, and for long-stay catheters it was 4,497.3 ± 605 procedures. Comparing the procedures (AVF, short-stay catheter, and long-stay catheter) over the years, a statistically significant difference was observed, with p<0.000. The same applies to the comparison between AVF and long-stay catheter, as well as between AVF and short-stay catheter.
Throughout the entire period analyzed, AVF was the most frequently performed procedure in every year. Among the catheters, there was greater use of the long-term catheter compared to the short-term catheter.
Table 1 – Annual frequency of vascular access in dialysis patients aged 19 and under. Brazil. 2015–2024.
|
Years |
AVF |
Short-CVC |
Long-term CVC |
Total |
|
2015 |
8.711 |
3.407 |
4.837 |
16.955 |
|
2016 |
7.822 |
3.769 |
4.043 |
15.634 |
|
2017 |
7.506 |
3.592 |
3.982 |
15.080 |
|
2018 |
7.716 |
3.585 |
3.574 |
14.875 |
|
2019 |
7.699 |
3.405 |
3.904 |
15.008 |
|
2020 |
7.012 |
3.051 |
4.574 |
14.637 |
|
2021 |
6.071 |
3.191 |
5.207 |
14.469 |
|
2022 |
5.492 |
3.837 |
4.827 |
14.156 |
|
2023 |
5.733 |
3.668 |
4.592 |
13.993 |
|
2024 |
5.623 |
2.956 |
5.433 |
14.012 |
|
Total |
69.385 (46,6%) |
34.461 (23,1%) |
44.973 (30,2%) |
148.819 |
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024
The time trend for FAV showed a high coefficient of determination, a downward trend, and statistical significance (R² = 0.893; β = −352.164; p = 0.000). For short-stay catheters: weak coefficient of determination, a decreasing trend, and statistically insignificant (R² = 0.096; β = −30.769; p = 0.382). For long-term catheters, there was a moderate coefficient of determination, an increasing trend, and no statistical significance (R² = 0.332; β = 115.157; p = 0.081). (Figure 1)
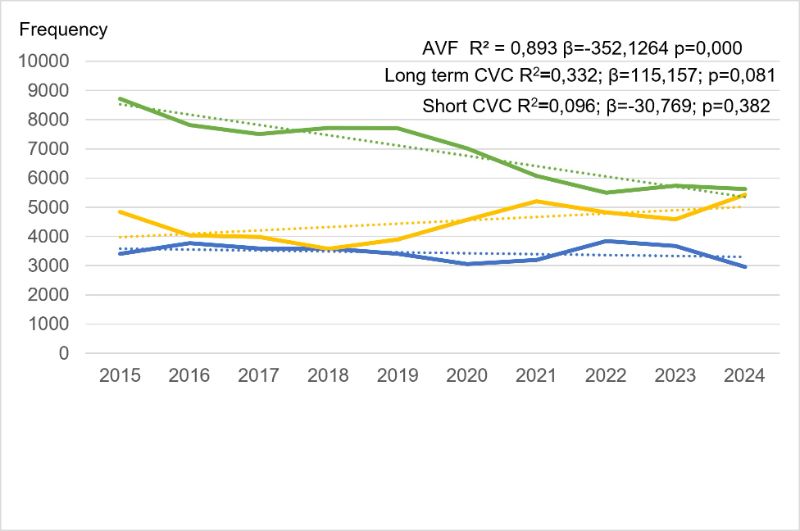
Figure 1. Time-series trend in the incidence of arteriovenous fistulas, short-term catheters, and long-term catheters in dialysis patients up to 19 years of age per year. Brazil. 2015–2024.
Regarding the patients’ biological sex, there was a predominance of males across all types of vascular access, although the difference between the sexes was not marked. Of the total procedures, 52.7% were performed on male patients and 47.3% on female patients. (Table 2)
The analysis of the association between the type of vascular access and the sex of patients up to 19 years of age was performed using Pearson’s chi-square test. Comparing the procedures (AVF, short-term catheter, and long-term catheter) with sex, a statistically significant difference was found, with p<0.000. The comparison between AVF and short-term catheter showed a value of X²=1.806, with 1 degree of freedom and p=0.1792, indicating no statistically significant difference between the sexes (p>0.05). On the other hand, when analyzing AVF and long-term catheters, X²=54.94, with 1 degree of freedom and p<0.000, indicating a statistically significant difference in the pattern of choice of vascular access type between the sexes (p<0.05).
Table 2 – Frequency of vascular access in dialysis patients aged 19 and under, by sex. Brazil. 2015–2024.
|
VA |
AVF |
Short CVC |
Long term CVC |
Total |
|
|
Male |
36.944 |
18.501 |
22.938 |
78.383 (52,7%) |
|
|
Female |
32.441 |
15.960 |
22.035 |
70.436 (47,3%) |
|
|
Total |
69.385 |
34.461 |
44.973 |
148.819 |
|
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024.
Analysis by age group reveals a significant increase in the total frequency of procedures as age increases. In the group of children under 1 year of age, the number of procedures accounts for 1.4%, while adolescents aged 15 to 19 years account for 60.7% of the total number of procedures performed during the period. (Table 3)
There is a progressive increase in the use of AVFs with increasing age, since long-term catheters predominate in younger age groups, and starting at age 10, there is a marked change in the access pattern, with a significant increase in AVF, which accounts for 35.8% of accesses among 10- to 14-year-olds and reaches 57.4% among 15- to 19-year-olds, becoming the predominant type of access in adolescence.
In the chi-square test performed to assess the association between age group and vascular access, the results were X²=16,250, with 8 degrees of freedom and p<0.000. In other words, there is a statistically significant difference in the type of vascular access across age groups.
Table 3 – Frequency of vascular access in dialysis patients aged 19 and under, by age group. Brazil. 2015–2024.
|
VA/years |
AVF |
Short CVC |
Long term CVC |
Total |
|
|
< 1 |
344 |
547 |
1.146 |
2.037 |
|
|
1-4 |
2.463 |
2.473 |
6.517 |
11.453 |
|
|
5-9 |
3.837 |
3.269 |
7.628 |
14.734 |
|
|
10-14 |
10.853 |
7.233 |
12.165 |
30.251 |
|
|
15-19 |
51.888 |
20.939 |
17.517 |
90.344 |
|
|
Total |
69.385 |
34.461 |
44.973 |
148.819 |
|
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024.
In terms of regional distribution, the Southeast region accounted for the highest absolute number of vascular accesses (60,829; 40.9% of the national total), followed by the Northeast (46,266; 31.1%) and South (17,038; 11.4%) regions. The Midwest and North regions had the lowest representation, with 12,762 (8.6%) and 11,924 (8.0%), respectively. (Table 4)
It is observed that AVF was the most frequent type of access in all regions, although with significant variation in its prevalence. The Midwest and North regions had the highest proportions of AVF (62.3% and 60.9%, respectively), while the South region had the lowest, at 38.3%.
The analysis, performed using the chi-square test of independence (X²), indicated a statistically significant difference (p<0.000) in the distribution of vascular access types among the Brazilian macro-regions.
Table 4 – Frequency of vascular access in dialysis patients aged 19 and under by Brazilian macro-region. Brazil. 2015–2024.
|
VA -Brazil |
AVF |
Short CVC |
Long term CVC |
Total |
|
|
North |
7.267 |
2.938 |
1.719 |
11.924 |
|
|
Northest |
22.947 |
10.669 |
12.650 |
46.266 |
|
|
Midwest |
7.952 |
1.970 |
2.840 |
12.762 |
|
|
Southeast |
24.696 |
13.655 |
22.478 |
60.829 |
|
|
South |
6.523 |
5.229 |
5.286 |
17.038 |
|
|
Total |
69.385 |
34.461 |
44.973 |
148.819 |
|
Negative results predominated for both infectious markers, accounting for approximately 95% of the records, followed by missing data (4.4%) and positive results—0.1% for hepatitis B surface antigen (HBsAg) and 0.3% for human immunodeficiency virus (HIV). (Table 5)
The proportional distribution of positive hepatitis B cases showed a slightly higher proportion among patients with long-term catheters, accounting for 0.17% (78/44,973). For HIV, the highest proportion of positive results was observed among individuals who used short-term catheters, representing 0.43% (150/34,461).
Table 5 – Prevalence of HBsAg and HIV infections in dialysis patients aged 19 and under, by type of vascular access. Brazil. 2015–2024.
|
Infection |
AVF |
Short CVC |
Long Term CVC |
Total |
|
HbsAg |
||||
|
Not filled in |
2.652 |
1.973 |
1.899 |
6.524 |
|
Negative |
66.644 |
32.446 |
42.996 |
142.086 |
|
Positive |
89 |
42 |
78 |
209 |
|
Total |
69.385 |
34.461 |
44.973 |
148.819 |
|
HIV |
||||
|
Not filled in |
2.724 |
1.991 |
1.864 |
6.579 |
|
Negative |
66.413 |
32.320 |
43.020 |
141.753 |
|
Positive |
248 |
150 |
89 |
487 |
|
Total |
69.385 |
34.461 |
44.973 |
148.819 |
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024.
Among dialysis patients who underwent AV access, the mortality rate was 0.65%, with a slightly higher rate among females (0.69%) compared to males (0.62%). (Table 6)
When analyzing in-hospital mortality according to the type of vascular access, it was noted that patients using AVF had the lowest rate (0.46%), while the highest rate was observed among patients with short-term catheters (1.07%), followed by those using long-term catheters (0.64%). (Table 6)
Table 6 – Hospital mortality rate (100%) among dialysis patients aged 19 and under, by type of vascular access and sex. Brazil. 2015–2024.
|
AC -gender |
AVF |
Short CVC |
Long term CVC |
Total |
|
Male |
0,44 |
0,98 |
0,62 |
0,62 |
|
Female |
0,47 |
1,17 |
0,66 |
0,69 |
|
Total |
0,46 |
1,07 |
0,64 |
0,65 |
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024.
This study found a trend toward a gradual decline in the hospital mortality rate among these patients over the years, with an overall decrease of 41% during the period analyzed. Dialysis patients using short-stay catheters had the highest rates throughout the entire period, peaking at 1.93% in 2020. (Figure 2)
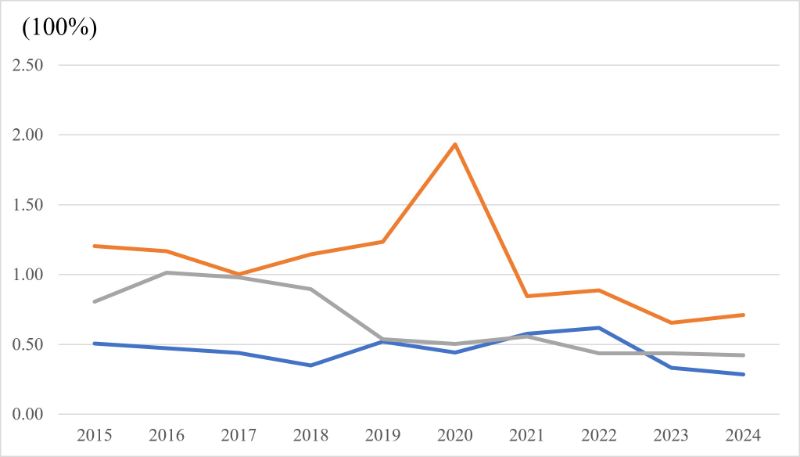
Figure 2 – Hospital mortality rate (100%) among dialysis patients aged 19 and under, by type of vascular access. Brazil. 2015–2024.
The in-hospital mortality rate was highest among patients under 1 year of age, with an average of 6.97%, particularly among those who used short-stay catheters, reaching 13.16%. In the other age groups, these rates were progressively lower. In the 15- to 19-year-old age group, the rates remained low, ranging from 0.40% for VAS to 0.80% for short-stay catheters. (Table 7).
Table 7 – Hospital mortality rate (100%) among dialysis patients aged 19 and under, by age group and type of vascular access. Brazil, 2015–2024.
|
Years/ VA |
AVF |
Short CVC |
Long term CVC |
Total |
|
< 1 |
4,07 |
13,16 |
4,89 |
6,97 |
|
1-4 |
0,81 |
1,54 |
0,95 |
1,05 |
|
5-9 |
0,55 |
1,13 |
0,47 |
0,64 |
|
10-14 |
0,49 |
0,75 |
0,36 |
0,50 |
|
15-19 |
0,40 |
0,80 |
0,51 |
0,52 |
|
Total |
0,46 |
1,07 |
0,64 |
0,65 |
Source: SUS Outpatient Information System (SIA/SUS), 2015–2024.
Discussion
Between 2015 and 2024, AVF was the most frequently recorded type of access during the analyzed period, accounting for 46.6% of procedures. However, when considered together, short- and long-term catheters accounted for more than half of the accesses (53.3%), indicating a predominance of temporary accesses in the study population. This finding is consistent with international data demonstrating widespread use of CVCs in pediatric patients, even in light of the recommendations of the KDOQI guidelines, which prioritize VAF as the initial access whenever possible.8,24
The temporal trend analysis revealed a statistically significant reduction in the use of AVFs over the decade studied, while long-term catheters showed a trend toward increase, albeit without statistical significance. In a historical Brazilian cohort evaluating children and adolescents on hemodialysis between 1997 and 2007, it was found that 51% initiated HD with a CVC, while AVF was used less frequently, indicating that the use of a catheter as the initial access was already predominant in the pediatric setting in Brazil and may have persisted in the following decades, contributing to the relative reduction in AVF use in the pediatric population.13 This pattern may be related to factors such as delayed referral to a nephrologist, the need for emergency initiation of hemodialysis, greater clinical complexity of pediatric patients, and structural difficulties in planning vascular access in advance—hypotheses widely discussed in the literature, as in the studies conducted by Astor et al.25 (2001) and Khatri et al.26 (2021)—but which cannot be confirmed based on the available data.10,18
The cohort study conducted by Fadrowski et al.24 (2009), based on national data from the USRDS and CMS, demonstrated that in children under 5–6 years of age, catheter use exceeded 85%, while the likelihood of AVF use increased progressively with age, with adolescents being up to three times more likely to use AVF compared to younger children. Similarly, data from the European ERA-EDTA registry (European Renal Association – European Dialysis and Transplant Association) indicate that, among children under 5 years of age, more than 70% used a catheter as their primary vascular access, while among adolescents, AVF accounted for approximately 45–55% of accesses, with a statistically significant association between age and type of access (p < 0.001). These international findings are consistent with the results of the study, which observed a predominance of catheters in younger age groups, especially among those under 5 years of age (79.2% catheter use), and a progressive transition to AVF with increasing age, reaching 57.4% AVF use among those aged 15–19 years. This pattern may be related to smaller vascular caliber, low body weight, the need for immediate initiation of therapy, and the greater technical difficulty in creating and maturing the AVF in young children.3,10,16 Thus, although the AVF is considered the gold-standard access, its applicability in the pediatric population depends heavily on age and physical development.
With regard to biological sex, a slight predominance of males was observed across all types of vascular access. This finding is consistent with international epidemiological studies, such as that by Hecking et al.27 (2014), which demonstrated a male predominance of approximately 55–60% (Dialysis Outcomes and Practice Patterns Study—DOPPS), and that of MacRae et al.28 (2021), with 61% men in a multicenter Canadian clinical cohort. However, unlike the adult population—where risk factors such as hypertension, smoking, and cardiovascular disease contribute to the development and progression of CKD—in the pediatric population, the main etiologies are related to congenital anomalies of the kidney and urinary tract (CAKUT), which account for approximately 45–60% of CKD cases in this population. Studies such as that by Harambat et al.29 (2012) indicate a higher prevalence of these malformations in males (male-to-female ratio ranging from 1.3 to 2.0), which may contribute to the slight predominance of boys observed in the study.
A statistically significant difference was observed when comparing PAFs and long-term catheters (p<0.000), indicating that gender may influence the choice of access method or the maintenance of long-term access. The study by Macrae et al.28 (2021) also demonstrates a lower probability of women undergoing AVF creation and using them successfully. This reinforces the hypothesis that anatomical (vascular caliber), biological (maturation time), and sociocultural (aesthetic impact) factors may be related to this pattern.
Regarding regional distribution, a significant concentration of the absolute number of AVs was observed in the Southeast region, accounting for approximately 41% of HD accesses. This predominance can be explained primarily by regional inequalities related to the availability of specialized services, hospital infrastructure, and access to vascular surgeons. The 2023 Brazilian Dialysis Census showed that of the 886 dialysis facilities in Brazil, the Southeast region has 450 active centers, reinforcing the concentration of these facilities in that region. 15 Although a higher proportion of AVFs was expected in the Southeast region, due to the greater concentration of technology and hospitals, the results showed that the North and Central-West regions had the highest proportions of this type of AV. A recent study published by Santos et al.30 in the Journal of Nephrology, 2024, highlighted significant inequalities in the distribution of hemodialysis units across the country, demonstrating that regions such as the North and Midwest have longer average distances traveled by patients to dialysis centers (84.3 km and 68.9 km, respectively) when compared to the Southeast (27.6 km). This may lead to a preference for creating AVFs to avoid frequent catheter changes and infectious complications, representing a possible survival strategy for the system in the face of precarious access to healthcare.
An extremely low prevalence of infectious markers was observed in the pediatric population on hemodialysis, with 0.1% HBsAg-positive and 0.3% HIV-positive. In comparison, the Brazilian Dialysis Census (2023), which predominantly reflects the adult population on dialysis, shows higher prevalences than those found in this study, albeit at relatively low levels in the national context. These findings suggest that the prevalence of viral infections in children and adolescents undergoing hemodialysis is lower than that observed in the adult population, possibly reflecting lower cumulative exposure over time, a lower presence of behavioral risk factors (such as risky sexual practices or injection drug use), and strong coverage of vaccination programs in the pediatric age group, factors that reduce the risk of viral infection transmission compared to the profile observed in adults on dialysis therapy.15
Regarding types of vascular access, a slightly higher proportion of HBsAg positivity was observed among long-term catheter users and of HIV positivity among short-term catheter users, consistent with evidence linking prolonged use of central venous catheters to a higher risk of infections and infectious complications compared to arteriovenous fistulas.12,18 However, it is not possible to attribute such infections exclusively to the type of vascular access due to the unavailability of data.
The observed in-hospital mortality rate was 0.65%, being lower among patients using AVF and higher among those with short-term catheters. This finding is consistent with previous studies that associate AVF with lower morbidity and mortality, attributed to a lower infection rate, greater durability, and better access performance. 10,12,19 However, the higher hospital mortality observed among catheter users may reflect greater clinical severity, the need for emergency initiation of hemodialysis, and the presence of comorbidities not measured in the database; it is not possible to attribute this outcome exclusively to the type of vascular access.31
Also noteworthy is the high rate of in-hospital mortality observed in children under 1 year of age, especially among those who used short-stay catheters, which underscores the vulnerability of this age group. Children of this age often present greater clinical complexity, anatomy complicated by small vessel caliber, the need for prolonged hospital stays, and greater exposure to infectious complications, as described in previous studies.3,22
Clinical studies and longitudinal registries indicate that survival among children and adolescents on renal replacement therapy has improved over the past few decades. USRDS reports show a continuing trend of increased survival among pediatric patients on hemodialysis, attributed to more effective protocols for clinical management, prevention of complications, and increased availability of early transplantation. 32 Reviews such as Raina et al. (2021) also highlight that, with improved vascular access practices and infection surveillance, clinical outcomes have improved in pediatric cohorts.3 These reports are consistent with the trend observed in the present study, which found a gradual reduction in the mortality rate over the years, suggesting advances in pediatric nephrological care.
In addition to the clinical outcomes mentioned, the choice of vascular access significantly impacts the patient experience. A systematic review conducted by Casey et al.33 demonstrated that patients using catheters report greater discomfort, fear of infections, and limitations in daily life, while those with AVF report a greater sense of security and better quality of life—aspects that may indirectly influence treatment adherence and clinical outcomes.
This study has limitations inherent to the use of secondary data from the SIA/SUS. The records refer to procedures performed, not to individual patients, which may overestimate absolute frequencies. Furthermore, the absence of detailed clinical variables—such as the etiology of kidney disease, duration of dialysis, comorbidities, source of infections, and specific complications—limits analyses adjusted for confounding factors. Possible inconsistencies in data entry due to underreporting, as observed in the blank fields for infectious markers, also represent a methodological limitation, indicating registration bias. Although the temporal trend analysis indicates a statistical association, the limited number of annual data points may restrict more robust causal inferences. Nevertheless, as this is a national database, the findings offer a comprehensive view of the vascular access profile for hemodialysis in the Brazilian pediatric population.
Thus, the results reinforce the AVF as the AV associated with better outcomes, while highlighting the specific challenges of the pediatric population and existing regional inequalities in Brazil. These findings may inform strategies for planning and organizing care, while acknowledging the limitations inherent in the study design.
Conclusion
The present study demonstrated that AVF was the most commonly used AV access in children and adolescents on hemodialysis in Brazil between 2015 and 2024, although with a decreasing trend over time. A higher prevalence of males was observed across all types of AV access analyzed. Catheters were predominant at younger ages, while AVF use was higher during adolescence, in addition to significant regional differences. These findings underscore the challenges involved in selecting an AV, particularly in more vulnerable populations, such as infants. Thus, they highlight the need for technical training, expanded access to AV creation, and continuous monitoring of quality indicators for pediatric dialysis therapy in Brazil.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org