International Surgery Case Reports
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Dr Monika Joshi MBBS, DNB1* (General Surgery), Dr Nitish Jhawar MBBS, MS2 (General Surgery)
1Department of Surgery, Apollo Hospitals, Navi Mumbai.
2Department of Surgery, Apollo Hospitals, Navi Mumbai.
*Corresponding author: Monika Joshi, MBBS, DNB (General Surgery), Department of Surgery Apollo Hospitals, Navi Mumbai.
Received: February 25, 2026 | Accepted: March 02, 2026 | Published: March 11, 2026
Citation: Joshi M, Jhawar N. (2026) “When Small Ports Fail: A Rare 5-mm Lateral Port-Site Hernia.”, International Surgery Case Reports, 8(2); DOI: 10.61148/2836-2845/ISCR/116.
Copyright: © 2026. Monika Joshi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Port-site herniation through trocar sites less than 10 mm is an uncommon complication following laparoscopic surgery. This report highlights a rare case of herniation through a 5-mm lateral trocar port site.
Case Presentation:
A 63-year-old obese female with a body mass index (BMI) of 35 kg/m2 presented with a bulge on the left lateral abdominal wall. She had undergone a laparoscopic hysterectomy and intraperitoneal onlay mesh (IPOM) repair for an umbilical hernia one year prior. Clinical examination revealed a 5x5 cm palpable mass in the left lateral abdominal wall. A computed tomography (CT) scan of the abdomen demonstrated a 3.1 cm defect in the anterior abdominal wall in the left lateral lumbar region. The patient was planned for laparoscopic repair of the hernia. Intraoperatively, the previous mesh was found to be in situ with omental adhesions overlying it. A defect in the left lateral abdominal wall was identified, with herniation of the omentum. Adhesiolysis was performed, and the lateral wall defect was repaired using V-Loc sutures. A 15x15 cm composite mesh was placed, and the port site was re-approximated with 2-0 Ethilon sutures. The skin was closed with absorbable continuous subcuticular sutures.
Conclusion
Port-site herniation through a 5-mm trocar port is an exceedingly rare complication of laparoscopic surgery. Prompt recognition and management are essential to avoid complications.
Port-site hernia, Hysterectomy, Laparoscopy, Lateral 5-mm port, Trocar-site hernia
Port site hernia (PSH), often referred to as port-site incisional hernia (PIH) or trocar site hernia (TSH), is characterized by the formation of a hernia at the sites of cannula insertion, with these names often used interchangeably in several publications. Published literature mentions the prevalence of PSH to be between 0.65% to 6.0%.1 Numerous authors have acknowledged this as the inaugural report on trocar site hernias. Crist and Gadacz defined trocar site hernia as the occurrence of a hernia at the cannula insertion site.2 Hitoshi et al. categorized trocar site hernias into three kinds based on documented instances.3 Early-onset type signifies dehiscence of the anterior fascial plane, posterior fascial plane, and peritoneum. The early-onset variant was identified in several case reports as commencing shortly after surgery, frequently manifesting as a small-bowel blockage. The late-onset type signifies dehiscence of the anterior and posterior fascial planes. The hernia sac of the late-onset kind is comprised of the peritoneum.
The late-onset form has frequently been associated, in several extensive studies, with problems arising after trocar implantation. Late-onset type hernias typically manifest in the latter phases, some months post-surgery. Furthermore, the literature review indicated that almost all trocar site hernias occur at sites >10 mm, with only a limited number of instances documenting herniation at 5 mm sites.
We report a case of an Indian patient who developed late incisional hernia at the lateral 5 mm trocar insertion site that was produced during the elective Laparoscopic total abdominal hysterectomy for the treatment of symptomatic uterine fibroid.
CASE REPORT
A 63-year-old obese female patient with BMI 35 kg/m2 presented to our centre with complaints of bulge in the left lateral abdominal wall that she had noticed first nearly 2 months back. It was known that the patient had undergone an elective laparoscopic Total Abdominal hysterectomy with Ipom for umbilical hernia through most lateral left 5 mm trocar port-site a year ago. Per-abdominal assessment led to finding of a palpable mass at the left lateral lumbar region, just above lateral 5 mm port-site scar. All haematological and biochemical parameters were within normal limits.
Plain CT scan of the abdomen was done that revealed a 3.1 cm sized defect in the anterior abdominal wall along the left lateral lumbar region with omentum and bowel loops as hernial contents. A diagnosis of trocar site incisional hernia (TSIH) was made, and the patient was planned for laparoscopic IPOM for the left lumbar hernia. Patient was placed in the supine position with a slight right tilt arms tucked by the side. Pneumoperitoneum was created using a Veress needle at the palmer’s point. Optical view entry using a 5mm optical trocar was done at the right hypochondrium, then a right iliac 5mm port and another 10mm port in the right lumbar region were placed under vision for instrumentation (figure 1). Adhesions were visualized over the previous mesh and adhesiolysis was performed. A defect in left lumbar region was seen, and it was approximated using absorbable barbed sutures in a continuous fashion. A 15x15 composite mesh was placed over the defect with a margin of 5 cm on either side. The defect was seen to be overlying on the previous mesh. Mesh was sutured using absorbable barbed sutures and inner crowning of the mesh was done using absorbable tacks. TAP block was given laparoscopically and proper haemostasis was achieved. 10mm port site was closed using a non-absorbable figure-of-8 stitch. Patient was shifted to ward, and she was managed with intravenous analgesics, antibiotics as well as antacids. Visual analogue scale (VAS) score for pain on post-operative day-1 was 3 out of 10. The patient recovered well after the procedure and was discharged in a hemodynamically stable state on post-operative day 2.
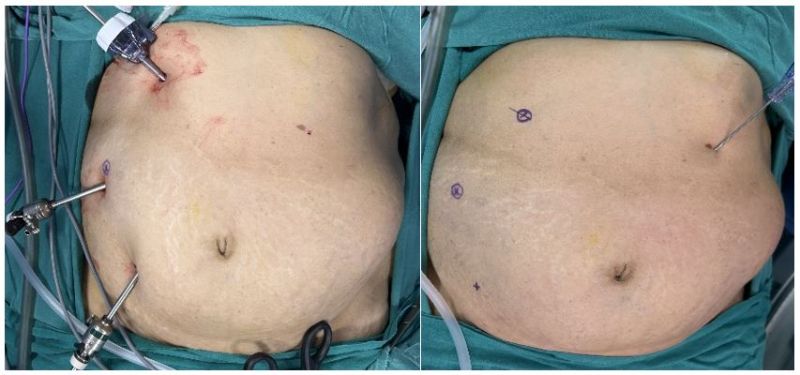
Figure 1: Port position- 5mm optical trocar at right hypochondrium, 10mm at right lumbar, 5mm at right iliac regions respectively.
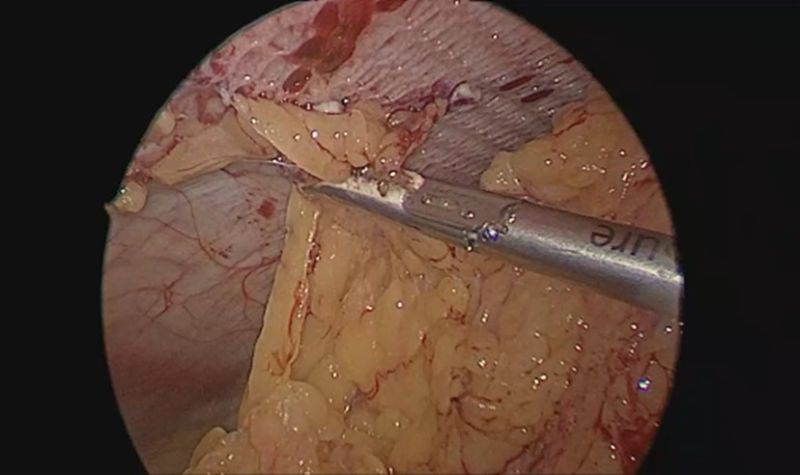
Figure 2: Omental adhesions over the previous mesh
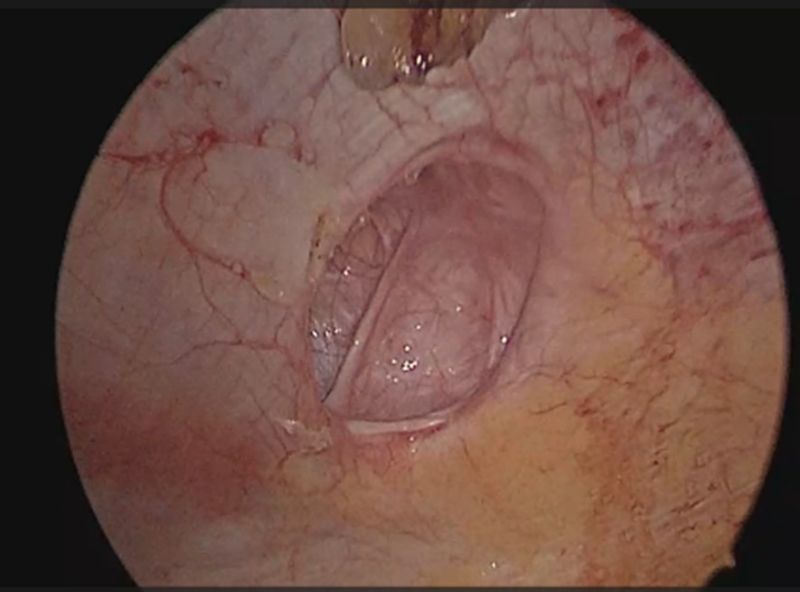
Figure 3: Defect in the left lumbar region
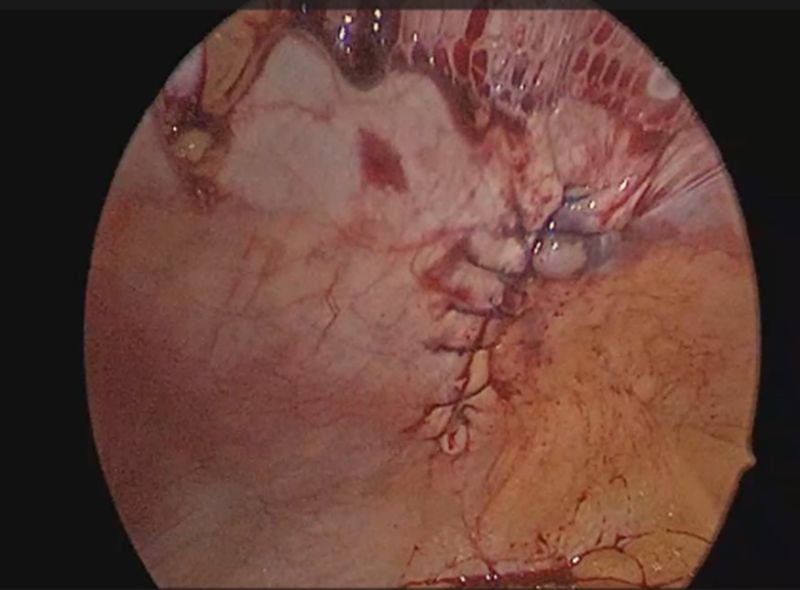
Figure 4: Defect closure with absorbable barbed continuous sutures
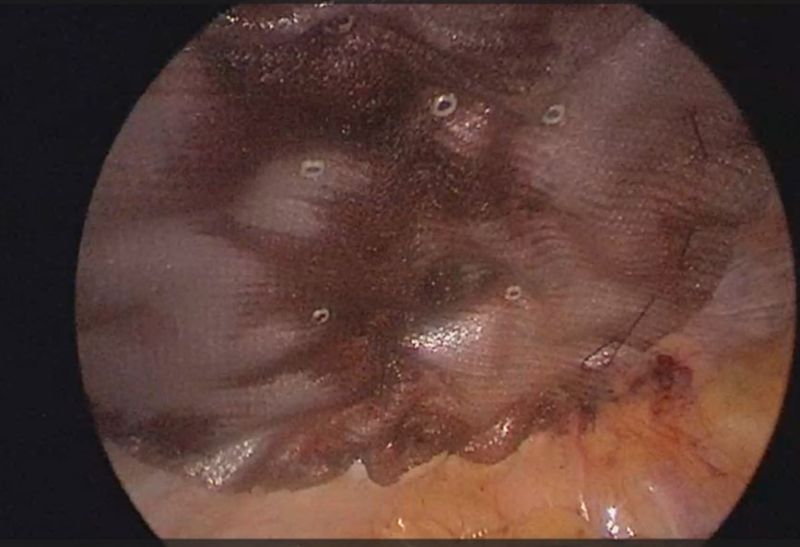
Figure 5: Mesh placement over the defect
DISCUSSION
We present a case of PSH arising in a 5 mm port, contributing to the continuing discourse over the requirement of fascial closure for ports less than 10 mm.4 The uncertainty stems from the infrequency of PSH in smaller ports lacking fascia closure; this instance is the authors' first encounter with PSH in a port measuring less than 10 mm.
The actual frequency of PSH, encompassing every type, is probably greater than what is documented in current research, due to patients either failing to disclose symptoms or being lost to follow-up.5
A widely accepted classification system categorized PSH into three types 3:
Most reported 5-mm trocar-site hernias belong to the late-onset category, often presenting as a localized swelling rather than acute obstruction.
Late-onset PSH frequently presents without symptoms, with recent reports revealing an incidence rate of up to 23.7%, evaluated either physical examination of incision sites or imaging techniques.6 While we present a case of late-onset PSH, it seems to be less alarming because to the infrequent incidence of bowel imprisonment, in contrast to the early-onset variant.7
The incidence of PSH in port sizes lower than 10 mm is presumed to be very low, but it is important to understand the pathogenesis behind the same. Several risk factors linked to PSH have been documented, including obesity, age over 60 years, diabetes, extended surgical time, trocar manipulation force, the requirement for fascia augmentation during specimen extraction, and single-port incision laparoscopy (SILS).8,9
In our case report, laparoscopic method was used to repair the PSH successfully. The laparoscopic technique facilitates the examination of the herniated intestine for viability, thus enabling intra-peritoneal onlay mesh repair. In the presence of gangrenous alterations in the strangulated gut, resection and anastomosis of the colon with primary repair must be performed. Late onset type PSH requires minimum expansion of the port site to facilitate the decrease of contents, followed by precise fascial closure using either an open or laparoscopic method. However, the laparoscopic method may be scrutinized due to the establishment of additional ports for the repair of the PSH, which may potentially serve as prospective locations for hernia development. This point is up for debate, but for now, laparoscopic method remains the best viable option for PSH repair.
Preventing trocar site hernias necessitates the closure of all port sites above 10mm at the fascial level. Certain authors advocate for the fascial closure of 5mm openings as well.3 Many authors have advocated for the deflation of pneumoperitoneum prior to port extraction to prevent the omentum and intestines from being pulled into the fascial defect. Additional methods to avert herniation encompass fascial closure with a fascial closure device, suture carrier, and Deschamps needle.10 Several publications have documented a reduced incidence of hernias associated with the utilization of a paramedian incision and non-bladed trocars featuring a conical tip.11














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org