International Surgery Case Reports
OPEN ACCESS | Volume 7 - Issue 3 - 2025
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Zahra Ansari Aval1, Mahdi Rezaei2, Niki Mirhosseini3, Seyed Mohsen Mirhosseini1*
1Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Mycobacteriology and Pulmonary Research, Pasteur Institute of Iran, Tehran, Iran
3Stritch School of Medicine, Loyola University, Chicago, Illinois, United States of America.
*Corresponding author: Seyed Mohsen Mirhosseini, Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Received: November 01, 2025 | Accepted: November 08, 2025 | Published: November 13, 2025
Citation: Zahra A Aval, Rezaei M, Mirhosseini N, Seyed M Mirhosseini. (2025) “Rare Self-Inflicted Cardiac Injury Due to Suicidal Needle Injection in a 17-Year-Old Female: A Case Report.”, International Surgery Case Reports, 7(3); DOI: 10.61148/2836-2845/ISCR/107.
Copyright: © 2025. Seyed Mohsen Mirhosseini. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Penetrating cardiac injuries, particularly those caused by self-harm, are exceptionally uncommon. There have been only a limited number of documented cases where sewing needles have penetrated the heart, with most of these associated with pre-existing psychiatric conditions. Such injuries present significant diagnostic and surgical challenges, particularly in accurately locating foreign objects within the heart. This case report describes a 17-year-old female who attempted suicide by injecting a needle into her heart. The needle was surgically extracted from the right ventricle after prompt diagnosis and intervention. This case highlights the importance of early recognition and multidisciplinary management in cases of intracardiac foreign objects, especially in patients with psychiatric conditions. While timely surgical removal is critical to prevent life-threatening complications, a better understanding of the psychological factors that lead to such extreme actions is essential. Future research should focus on the integration of psychiatric care into the management of patients at risk for self-inflicted injuries, as well as advancements in non-invasive diagnostic techniques to improve the identification and treatment of foreign bodies in the heart.
Needle Injury, Suicide, Trans Thoracic Echocardiography (TTE)
"This article was previously posted to the ESS Open Archive eprints on March 2024” [1]
Although rare, sharp objects such as pins, needles, and other items have been used to inflict injuries on the chest area as a means of suicide, often reflecting underlying psychiatric distress [2]. Approximately one-third of all cases of penetrating cardiac injuries are caused by sharp objects, and these injuries carry a significant risk of fatality, especially when diagnosis and treatment are delayed, leading to life-threatening complications such as cardiac tamponade [3]. Despite the overall rarity of such incidents, there are documented cases of individuals deliberately injuring their hearts with sharp objects, including needles, often associated with psychiatric disorders like major depression, dissociative disorders, and substance use [2].
The rarity of self-inflicted cardiac trauma poses unique challenges for both diagnosis and treatment. Penetrating injuries to the heart commonly affect the right ventricle due to its anatomical location, with symptoms ranging from chest pain and shortness of breath to potentially being asymptomatic [4]. Advanced imaging techniques, such as transthoracic echocardiography (TTE), are crucial in the timely and accurate localization of foreign objects in the heart, allowing for precise surgical planning and intervention [5].
This paper presents the case of a 17-year-old girl who attempted suicide by injecting a syringe needle into her heart. The case underscores the importance of prompt recognition, multidisciplinary management, and the role of mental health in addressing both the physical and psychological dimensions of self-inflicted cardiac injuries.
Case Presentation
A 17-year-old female student from the suburbs was brought to our center following a suicide attempt and chest trauma. Upon arrival at the emergency room, the patient was alert but exhibited aggressive behavior. She experienced mild respiratory distress and pain during breathing.
The patient had a history of neurological medications, including fluoxetine, tiapride, and imipramine. She also had a history of similar chest traumas, as well as self-inflicted burns on her forearm and right hand. Additionally, she had been diagnosed with attention deficit hyperactivity disorder (ADHD) and had been taking methylphenidate since childhood. Her medical history also included trichotillomania and sleep-talking.
Physical examination revealed an obese young female, weighing 102 kg, with a height of 170 cm. Her vital signs were as follows: blood pressure 120/70 mmHg, pulse rate 107 bpm, temperature 37°C, and respiratory rate 12 breaths per minute. Lung auscultation was relatively clear, and the trauma site was noted at the fifth intercostal space along the midclavicular line.
Emergency diagnostic measures were promptly conducted, including a chest X-ray (Figure 1), echocardiography, and a computed tomography (CT) scan of the chest (Figure 2). The echocardiogram revealed an ejection fraction of 55%, along with early signs of cardiac tamponade, characterized by a small pericardial effusion measuring 5 mm anteriorly, 10 mm posteriorly, and 7 mm laterally, with an estimated total volume of 100-150 ml. Since echocardiography does not provide a clear visualization of the needle's path, a CT scan was performed, as illustrated in Figure 2.

A median sternotomy was performed under general anesthesia with endotracheal intubation. Upon opening the chest, a large hematoma was discovered on the pericardium. The pericardium was then incised, allowing for the drainage of the clot and a significant volume of blood (approximately 550 mL). The syringe needle (Figure 3) was located within the right ventricle. The entry point was traced from the left pleural cavity into the pericardial cavity. The needle was then manually extracted from the heart (Figure 4) without the use of a cardiopulmonary bypass machine, and the bleeding site was secured with sutures. After placing drains in both the left pleural and pericardial spaces, the chest was closed, and the patient was transferred to the intensive care unit (ICU) in stable condition. She was discharged after six days with ongoing psychiatric care and a treatment regimen that included haloperidol, lorazepam, amitriptyline, imipramine, and antibiotics.
Over the past six months, under psychiatric care, she has not experienced any heart-related issues.
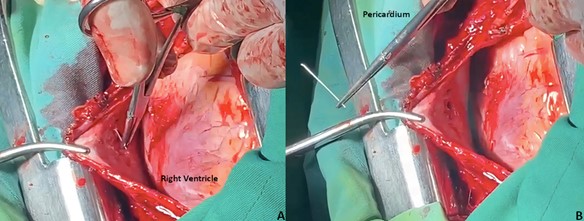
Figure 3: Extraction of the needle from the right ventricle, with confirmation of puncture damage to the right ventricle

Figure 4: Extracted needle
Discussion
Suicide is a significant public health concern that claims more lives annually than interpersonal violence and war. Depression, particularly among elderly adults, is a leading contributor to suicide attempts [6]. The social stigma surrounding mental illness and suicide often results in underreporting, making it difficult to accurately assess the scale of the problem [4]. Self-destructive behavior is sometimes associated with medical conditions like Lesch-Nyhan syndrome, de Lange syndrome, Gilles de la Tourette's syndrome, and cognitive impairments. Psychiatric disorders such as personality disorders, dissociative disorders, schizophrenia, major depressive episodes, mania, and gender dysphoria also play a role in suicidal behavior [2]. In many cases involving the self-embedding of needles into the heart, substance use (drugs or alcohol) is a common factor, exacerbating impaired judgment and risky behavior [7]. However, in our patient, there was no evidence of substance use, but underlying conditions like depression and ADHD may have contributed to her actions.
Trauma involving the heart, especially from sharp objects such as needles, is rare but poses severe risks. Self-inflicted injuries involving needle insertion into the chest, while uncommon, have been documented. Schechter and Gilbert (1969) reported that 56% of injuries involving pins and needles in the heart and great vessels were accidental, while 33% were intentional acts of self-harm [8]. From 1967 to 2013, only 40 cases of sewing needles impaling the heart were reported, with 90% occurring in patients with significant psychiatric conditions [2]. Our case involved a suicide attempt using a syringe needle, contributing to a unique form of cardiac trauma.
Cardiac trauma from penetrating objects typically affects the right ventricle, followed by the left ventricle, right atrium, and left atrium. The prognosis depends on factors like the type of object, the location of the injury, associated pericardial damage, and adjacent lung involvement [9]. Symptoms of penetrating cardiac trauma often include chest pain and shortness of breath, although some patients may remain asymptomatic [10]. In our case, the patient exhibited typical symptoms of difficulty breathing and chest discomfort. Immediate diagnosis and intervention are crucial, as the most common fatal complication, pericardial tamponade, can occur when the pericardium fills with blood due to a puncture wound.
Diagnosis of cardiac trauma is achieved through imaging techniques, with transthoracic echocardiography (TTE) being a preferred method due to its high accuracy and non-invasive nature [11]. TTE can localize foreign objects within the heart and provide critical information about the object's size, position, and movement, assisting in preoperative planning [5]. In this case, TTE effectively localized the needle in the right ventricle, enabling its safe manual extraction during surgery.
Managing cardiac trauma from self-inflicted injuries requires a multidisciplinary approach, involving collaboration between cardiologists, cardiothoracic surgeons, radiologists, psychiatrists, and emergency care providers [12]. The treatment decision-making process takes into account several factors, including the patient’s clinical presentation, the size and location of the foreign object, the risk of complications, and the patient’s overall psychiatric and medical condition [13]. Treatment options for foreign body removal from the heart can range from minimally invasive surgery to open-heart surgery, and the decision is influenced by the characteristics of the injury and patient stability [14].
Minimally Invasive Surgery such as thoracoscopy or video-assisted thoracic surgery (VATS), can be utilized in certain cases to remove foreign objects without the need for open surgery; They are especially useful for objects located in accessible areas of the chest or heart [15]. In cases of needle insertion, however, the risk of damage to surrounding structures may still necessitate a more invasive approach. Open-Heart Surgery uses for foreign bodies like sewing needles or syringe tips that penetrate deeply into the heart tissue, open-heart surgery is often necessary. In cases where the needle is embedded within the myocardium, especially if it is causing hemodynamic instability or is at risk of migration, open surgery allows for direct visualization and safe removal. Cardiopulmonary bypass (CPB) may be required if the object is not easily accessible or poses a risk to the heart's structural integrity [16]. In our patient’s case, the needle tip was visible on the surface of the heart, which allowed for successful manual extraction without CPB. In this case, after careful evaluation of the needle's position using transthoracic echocardiography (TTE), the surgical team decided on manual extraction due to the needle's accessibility and the patient's overall stability. Had the needle been more deeply embedded or posed greater risk, a more invasive procedure, possibly requiring CPB, would have been necessary.
Timely recognition and management of self-inflicted cardiac trauma are essential to prevent fatal outcomes. Although rare, this type of trauma requires immediate medical attention, and the successful outcome in our case highlights the importance of early intervention, accurate imaging, and appropriate surgical techniques in treating patients with self-inflicted penetrating cardiac injuries.
Conclusion
This report underscores the importance of considering intracardiac foreign objects in individuals with self-aggressive tendencies, demonstrating how early detection and intervention can save lives. The necessity of prompt surgical removal is emphasized as crucial. Additionally, echocardiography is highlighted as the primary noninvasive diagnostic tool. Rapid recognition of warning signs of self-aggressive behavior, combined with immediate medical response, is essential for effectively mitigating life-threatening complications.
Additional Information
Author Contributions
Zahra Ansari Aval: Conceptualization; project administration; supervision; writing – original draft.
Mahdi Rezaei: Data curation; resources; supervision; Methodology.
Niki Mirhosseini: Data curation; resources; supervision; Methodology.
Nmirhosseini1@luc.edu
Seyed Mohsen Mirhosseini: Supervision; visualization; writing – original draft.
mohsenmirhosseini@sbmu.ac.ir
Disclosure
Study Limitations: This study has no notable limitations. The case was managed effectively with appropriate diagnostic and surgical interventions, and all relevant factors were thoroughly considered. Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Acknowledgment
We acknowledge the use of ChatGPT for assistance in correcting grammatical errors and clarifying certain sentences in the manuscript.
ORCID
Seyed Mohsen Mirhosseini
https://orcid.org/0000-0002-2903-682X
Mahdi Rezaei
https://orcid.org/0000-0003-0409-2072














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org