International Surgery Case Reports
OPEN ACCESS | Volume 7 - Issue 1 - 2025
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Gosaye Tekelehaymanot Zewde
Department of Midwifery, Harar Health Science College, Harar, Ethiopia
Corresponding author: Gosaye Tekelehaymanot Zewde, Department of Midwifery, Harar Health Science College, Harar, Ethiopia
Received date: February 27, 2021
Accepted date: March 02, 2021
published date: March 08, 2021
Citation: Gosaye T Zewde, “Level of Knowledge and Associated Factors Towards Essential Newborn Care Practices Among Postnatal Mothers Attending Post Natal Service in Governmental Hospital of Harar Town, Eastern Ethiopia 2020.”. International Surgery Case Reports, 2(2); DOI: http;//doi.org/03.2021/1.1010.
Copyright: © 2021 Gosaye Tekelehaymanot Zewde. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Essential new born care is a set of comprehensive recommendations designed by World Health Organization (WHO) to improve health of the new born through intervention before conception, during pregnancy, soon after birth and in postnatal period. Globally 4 million newborn die every year before they reach the age of one month. In Ethiopia neonatal mortality estimated 29 deaths per 1000 live births and 19 deaths per 1000 live births for post-neonatal mortality. Even those few studies conducted on essential newborn care practice in Ethiopia, there is no sufficient information in our study area there for come this study will try to fill the information gap which was not address by other researchers.
Objective of the study: Assessment of Level of Knowledge and Associated Factors towards Essential Newborn Care Practices among postnatal mothers attending post natal service at Governmental Hospital of Harar Town, Eastern Ethiopia 2020
Methods: Facility based cross sectional study was conducted in Harari Town, Jugul and Hiwot Fana Specialized University Hospital. Voluntary postnatal mothers who are randomly selected were participated on the study. A total sample of 266 women was included on the study. Data was collected through face to face interview. Training was given for data collectors and data evaluation was done on daily based. Cleaned data was entered to SPSS version 20 and multiple logistic regression analysis was used for better prediction of determinants and to reduce bias due to confounders. Those variables with P-valueless than 0.25 were entered in to multiple logistic regression analysis. Associations with P - value less than 0.05 was declared as statistically significant. Result was presented by figure, table and effort will made to published in a relevant scientific journal and disseminated online.
Result: The overall prevalence of good knowledge was 57.2%. Educational Status, Average monthly income, ANC visit and Parity had significantly associated with outcome variables
Conclusion and Recommendation: More than half of mother had inadequate newborn care knowledge. There for to enhance it maternal knowledge improvement need to be established.
1. Introduction: Essential newborn care is a set of comprehensive recommendations designed by World Health Organization (WHO) to improve health of the newborn through intervention soon after birth and in postnatal period [1]. It includes thermal care, clean delivery and cord care, early initiation of breastfeeding, immunization, eye care, recognition of danger signs, care of the preterm / low birth weight and management of newborn illnesses [2,3]. Newborn care is of immense importance for the survival and proper development and healthy life of a baby [4].
Statement of the problem: Globally 4 million new-borns die every year before they reach the age of one month. Approximately 3.4 million new-borns die within the first week of life of these deaths 66% occur during the 1st 24 hours it can prevented if mothers have good knowledge about new born care including danger signs of new born [5]. More than half of the approximately 7.5 million neonatal deaths in the world occur in the first four weeks after birth. Ninety-eight percent of these neonatal deaths occur in developing regions, 28 % in the least developed countries. Overall, there were 30 neonatal deaths per 1000 live births; 5 per 1000 in developed and 33 per 1000 in developing regions, and 42 per 1000 in the least developed countries. This means that in developing regions, the risk of death in the neonatal period is more than six times than that of developed countries; in the least developed countries, it is more than eight times higher [6].
In Ethiopia during the past five-year period, neonatal mortality estimated 29 deaths per 1000 live births and 19 deaths per 1000 live births for post-neonatal mortality. Even though there is improvement about the past five years, under-5 mortality rates 67 deaths per 1,000 live births in 2016, 48 deaths per 1,000 live births. Thus, further intervention is needed to sustain the improvement for neonatal mortality [7].
Global estimates suggest that over two-thirds deaths can be prevented using proven and cost-effective existing maternal and child health programs interventions like Home-Based New-born Care (HBNC) package, prompt postnatal care (PPNC) [7, 8 9].
Significance of study: The ability to identify knowledge gaps early in the neonatal period would help healthcare workers identify and implement timely and appropriate interventions that would lead to better neonatal outcomes. Therefore, this study will be expected to investigate the mothers’ level of knowledge and associated factors towards essential newborn care practice which the researchers, policy makers, healthcare workers and community and care givers use as a base line for their future interventions and activities.
2. Objectives
2.1 General Objective
2.2 Specific Objectives
3. Methodology
3.1 Study Area and Period: The study was conducted in Harar town which is one of the ten regional states of the Federal Democratic Republic of Ethiopia located in the eastern part at a distance of 526 km away from Addis Ababa, the capital city of Ethiopia. In the region, there are3 governmental and 2 private hospitals as well as 1 Fistula hospital and 8 Health centres were found [6]. The study was conducted in Jegula and Hiwot Fana Specialized University Hospital from Feb 7 – 25, 2020 G.C
3.2 Study design: Institutional based cross-sectional study was conducted
3.3. Population
3.3.1. Source population
All mother who are having postnatal service in Hiwot Fana Specialized University and Jugel Hospital Harar Ethiopia 2020.
3.3.2. Study Population
Randomly selected postnatal mothers in Hiwot Fana Specialized University and Jugel Hospital Harar
3.4 Eligibility criteria
3.4.1 Inclusion criteria
3.4.2 Exclusion criteria
3.5 Sample Size Determination: Sample size was determined by using a single population proportion formula by assuming 5% marginal error and 95% confidence interval (∂ (alpha) = 0.05) the prevalence of good Knowledge towards essential newborn care was 80.4 % on study conducted in Addis Ababa. [17] And by considering 10% non-response rate, the final sample size will be become 266
3.6 Sampling Technique and Procedure: Two governmental Health institutions were selected by SRS method and samples were proportionately allocated based on their average monthly postnatal client flow. Individual study participants who meet the inclusion criteria from each health facility were selected by systematic random sampling;
In Harar town there are 3 governmental Hospital
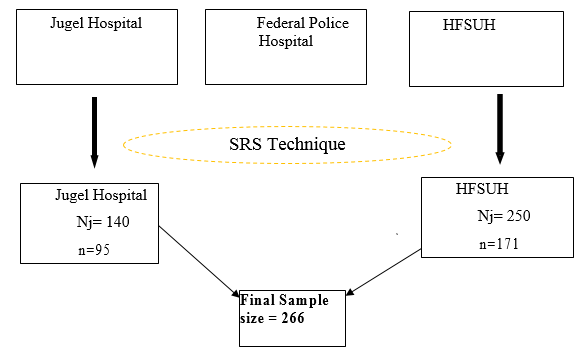
Figure 2: Adapted schematic presentation of the Sampling Procedure on postnatal mothers attending postnatal service in Governmental Hospital of Harar Town, Eastern Ethiopia 2020.
3.7 Study variables
3.7.1 Dependent variables
3.7.2. Independent variables
3.8 Operational definition
Poor knowledge: Questions regarding knowledge of breast feeding, cord care, eye care, immunization, thermal care, and identification of danger sign measures for newborn care were scored and if the women answered below or equal to the mean value had said to be poor knowledge [8].
Good knowledge: Questions regarding knowledge of breast feeding, cord care, eye care, immunization, thermal care, and identification of danger sign measures for newborn care were scored and if the women answered above the mean value had said to be Good knowledge [8].
4.9. Data collection tools: Data collection instrument was developed after critical review of literature (15 -19). It contains socio- demographic characteristics, Antenatal care and delivery history of the women and mother’s knowledge on the WHO essential newborn care practices.
3.10 Data Collection Procedure: Data was collected by 4 diploma midwife via face to face interview after having informed consent from the study participants who full fills inclusion criteria.
4.11 Data Processing and Analysis: Data checking and cleaning was done on daily basis and analysis was done using SPSS version 20.0. The Uni-variate analyses such as proportions, percentages, ratios, frequency distributions and appropriate graphic presentations as well as measures of central tendency and measures of dispersion were made. Multiple logistic regression analysis was used for better prediction of determinants and to reduce bias due to confounders. Those variables with P-valueless than 0.25 will entered into multiple logistic regression analysis. Associations with P - value less than 0.05will be declared as statistically significantat 95% confidence level
4.12. Data Quality Assurance: Data quality assurance mechanisms were instituted at several points to ensure the quality of the data. Pre-test was conducted, questionnaires was translated into local language. Training was given for Data collector and supervisor. Prior to data collection they were allowed to fill the questionnaire and later discussion was made in all contents of the questioners and areas of difficulties were revised. The data was coded carefully in order to increase accuracy and quality of data.
3.13. Ethical Considerations: Ethical clearance letter was obtained from Harar Health Science College Research Ethics Review Committee and it was submitted to the study organization and consent was obtained from hospital CEO and Permission was obtained from study institution. All the participants were informed the purpose, advantages and disadvantages, there have the right to be involved or not as well as they can withdraw from the study any time they want. Informed verbal consent was obtained from all participants. Confidentiality was maintained by avoiding names and other personal identification.
4. Result
4.1 Socio demographic characteristics
From 266 postnatal mothers, 257 women were interviewed which makes response rate 96.6%. Majority 123 (47.9%) of respondents were between the age group 25 -34 years with mean age of 27.18 and standard deviation of (SD ± 5.922) and ranges from 18 to 40 years. Regarding marital status majority 242 (94.1%) of the respondent were married and their first age for marriage was minimum of 18 and max 35 years with mean age of 21.68 and standard deviation of (SD ± 2.77). Most of respondents were 127 (49.4%) Muslim religion followers and from 175 (68.1%) Oromo ethnic group and one third 73 (28.4%) of respondent were Unable to read and write. Regarding Occupation Status and living area majority 130 (50.6%) and 174 (67.7%) were House wife and live in Rural. Regarding average monthly income ranges from 300 up to 8500 birr with mean of 2902 and standard deviation of (SD ±2535) (Table 1)
|
S. No |
Variable |
Characteristics |
Frequency |
Percent |
|
1 |
Maternal age
|
18-24 |
90 |
35 |
|
25-34 |
123 |
47.9 |
||
|
35-40 |
44 |
17.1 |
||
|
2 |
Marital status |
Single |
6 |
2.3. |
|
Married |
242 |
94.1 |
||
|
Divorced/Separated |
7 |
2.7 |
||
|
Widowed |
2 |
0.8 |
||
|
3 |
Religion |
Orthodox Christian |
98 |
38.1 |
|
Muslim |
127 |
49.4 |
||
|
Protestant |
22 |
8.6 |
||
|
Catholic |
8 |
3.1 |
||
|
Other |
2 |
0.8 |
||
|
4 |
Ethnicity of Mother |
Oromo |
175 |
68.1 |
|
Amhara |
57 |
22.2 |
||
|
Harari |
7 |
2.7 |
||
|
Tigray |
6 |
2.3 |
||
|
Other (specify) |
12 |
4.7 |
||
|
5 |
Educational Status |
Unable to read and write |
73 |
28.4 |
|
Able to read and write |
62 |
24.1 |
||
|
Primary education |
41 |
16 |
||
|
Secondary education |
33 |
12.8 |
||
|
College and above |
48 |
18.7 |
||
|
6 |
Occupation of mother |
House wife |
130 |
50.6 |
|
Private employee |
51 |
19.8 |
||
|
Government employee |
43 |
16.7 |
||
|
Merchant |
12 |
4.7 |
||
|
Farmer |
10 |
3.9 |
||
|
Student |
11 |
4.3 |
||
|
7 |
Living area (Residence) |
Rural |
174 |
67.7 |
|
Urban |
83 |
32.3 |
||
|
8 |
Families monthly income (in Birr) |
< 1000 |
106 |
41.2 |
|
1001 – 2000 |
41 |
16.0 |
||
|
>2001 |
110 |
42.8 |
Table 1: Socio - demographic characteristics of postnatal mothers in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.2 Antenatal care and delivery history of study participants
In this study majority 222 (85.3%) and 68 (30.6%) of mother had ANC follow up and more than 4 times had ANC visit. Regarding initiation time of ANC majority 68 (30.6%) start visit at 3 month of gestational age there min and max month of starting ANC was at 1 and 9 month with mean of 3.93 and standard deviation of (SD ± 1.625). Majority 93 (36.2%) of study participant had gave birth once and the max birth was 10 (0.4%) with mean of 2.4 and standard deviation of (SD ± 1.633). the minimum and maximum number of delivery ranges from 1 up to 10 with mean of 2.4 delivery. During data collection time majority 101 (39.3%) of study participant replied that they have one child living with them. Regarding time spent to reach to hospital the min and max duration mentioned was 2 and 300 min respectively with mean of mean of 39.1 and standard deviation of (SD ± 41.04). (Table 2)
|
S. No |
Variable |
Characteristics |
Frequency |
Percent |
|
1 |
Have ANC follow up |
Yes |
222 |
85.3 |
|
No |
35 |
14.7 |
||
|
2 |
Frequency of ANC follow up |
One |
33 |
14.9 |
|
Two |
56 |
25.2 |
||
|
Three |
65 |
29.3 |
||
|
Four and above |
68 |
30.6 |
||
|
3 |
When start ANC |
Before 16 Wks |
165 |
74.3 |
|
> 16 wks |
57 |
25.7 |
||
|
4 |
Number of delivery (Para) |
Primiparous |
93 |
36.2 |
|
Multiparas |
164 |
63.8 |
||
|
5 |
Number of child have |
1 up to 3 child |
212 |
82.5 |
|
4 to 10 child |
45 |
17.5 |
||
|
6 |
Time spent to reach hospital |
2 up to 60 min |
197 |
76.7 |
|
61 minute up to 300 min |
60 |
23.3 |
||
|
7 |
Sex of previous delivery |
Male |
139 |
54.1 |
|
Female |
118 |
45.9 |
||
|
8 |
Place of birth |
Health facility |
252 |
98.1 |
|
Home |
3 |
1.2 |
||
|
Other (specify) |
2 |
0.8 |
||
|
9 |
Last delivery attendant |
Skilled health care provider |
245 |
95.3 |
|
Trained traditional birth attendant |
7 |
2.7 |
||
|
Traditional birth attendant |
5 |
1.9 |
||
|
10 |
Mode of delivery |
SVD |
179 |
69.6 |
|
Caesarean section |
66 |
25.7 |
||
|
Instrumental |
12 |
4.7 |
Table 2: Antenatal care and delivery history of postnatal mothers in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.3 Knowledge on Essential Newborn Care
4.3.1 Breast Feeding:
Majority 204 (79.3 %) of mothers reported that their newborns were breastfed within the first hour after delivery and 53 (20.7 %) squeezed out the colostrum before breastfeeding. The most commonly food given was formula feed 28 (58.4%) and 220 (85.6%) reported exclusive breastfeeding for 6 months is recommended for the new born (Table 3)
|
S. No |
Variable |
Characteristics |
Frequency |
Percent |
|
1 |
Do you know early initiation of Breastfeeding |
Yes |
32 |
12.5 |
|
No |
225 |
87.5 |
||
|
2 |
When did you start Breast Feeding |
Within 1 hour after delivery |
204 |
79.4 |
|
After 1 hour up 1day |
53 |
20.6 |
||
|
3 |
Have you squeezed out the colostrum |
Yes |
53 |
20.7 |
|
No |
204 |
79.4 |
||
|
4 |
Do you provided anything other than breast milk for new born |
Yes |
48 |
18.7 |
|
No |
209 |
81.3 |
||
|
5 |
first feed you gave to the baby immediately after delivery |
cow’s milk |
9 |
18.7 |
|
Plain water |
6 |
12.5 |
||
|
Formula feed |
28 |
58.4 |
||
|
Sugar water |
4 |
8.3 |
||
|
Other (specify) |
1 |
2.1 |
||
|
6 |
Do you know breast should be given on demand |
Yes |
162 |
63 |
|
No |
95 |
37 |
||
|
7 |
Do you know important of clostrum feeding |
Yes |
183 |
71.2 |
|
No |
74 |
28.3 |
||
|
8 |
Do you know exclusive breast feeding is recommended for 6 month |
Yes |
220 |
85.6 |
|
No |
37 |
14.4 |
||
|
9 |
Do you know the importance of prelacteal feeds |
Yes |
173 |
67.3 |
|
No |
84 |
32.7 |
Table 3: Knowledge of postnatal mothers towards Breast Feeding in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.3.2 Immunization
Among 257 respondent’s majority 206 (80.2%) of mothers child were vaccinated. More than half 185 (72%) of respondent agreed that New born need to be vaccinate at birth and 190 (73.9%) Mentioned vaccine was important to prevent disease. And 93 (36.2%) and 144 (44%) replied that BCG and Polio protect tuberculosis and polio mellitus respectively. (Fig 1)
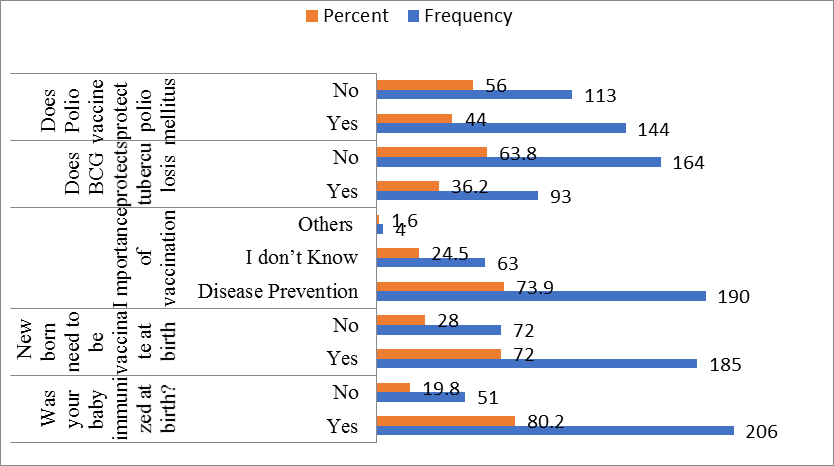
Figure 1: Knowledge of postnatal mothers towards Immunization in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.3.3 Thermoregulation
Among respondents 175 (68.1%) had replied there had know how to maintain body temperature of the new born, majority 135 (52.5 %) replied that wrapped the baby in a cloth immediately will important to maintain temperature. Regarding bathing of newborn 109 (42.4%) only correctly identified the proper time of bathing which was after 24 hour of delivery. (Fig 2)
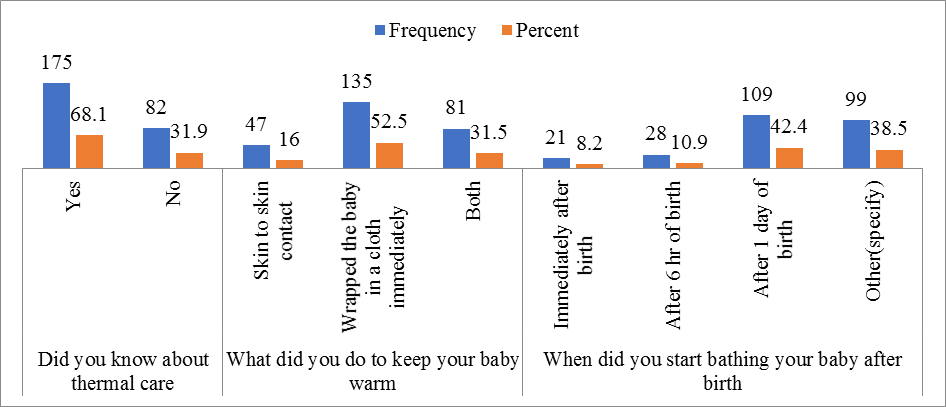
Figure 2: knowledge of postnatal mothers on thermoregulation in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.3.4 Knowledge on Eye and Cord care
From the study participants Majority187 (72.8 %) of mothers are aware of signs of eye infection
and 108 (49.4%) of women reported that reddening of eye is the main symptom followed by Abnormal eye discharge which accounts 66 (30.1%). Regarding cord care majority 79 (30.7%) replied that cord should be cover with cloth. 131 (49%) of the participant replied that something need to applied to the cord while 30 (22.9%) of mothers mentioned that butter should be applied to the stump, while 74 (56.6 %) of mothers know that Vaseline was applied on the cord (Table 4).
4. 3. 5 Knowledge on Danger Sign: Among 257 respondents more than half 171 (66.5%) replied
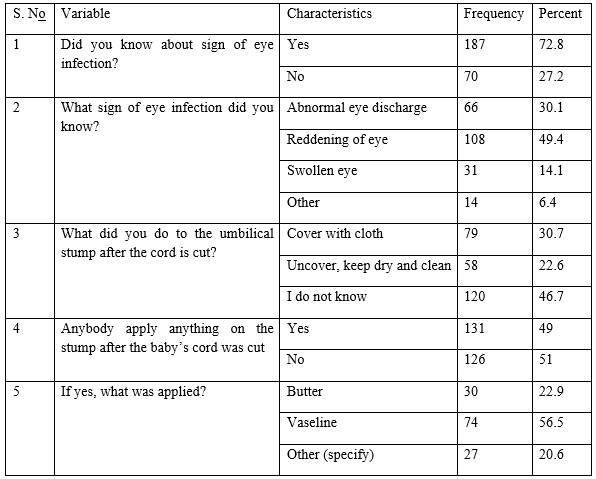
Table 4: knowledge of postnatal mothers on Eye and Cord care in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
that they had know about danger sign on the new born, among those danger sign majority 129 (50.2%) recognized fever as a danger sign while few 2 (0.8%) of them recognized baby being too small/born being too early as a danger sign and 86 (33.5%) did not have awareness on newborn danger signs. Regarding information during pregnancy 206 (80.2%) of participant had provided information the most frequently provided information was about 82 (31.9 %) breast feeding by 113 (44 %) midwives (Table 5)
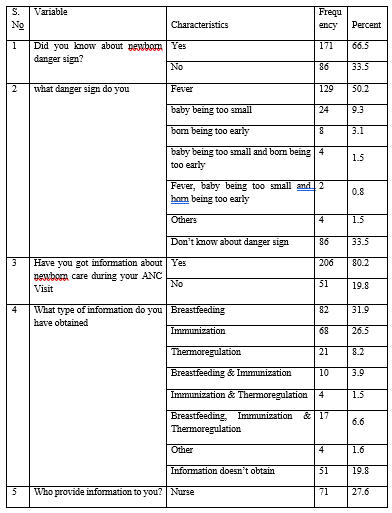
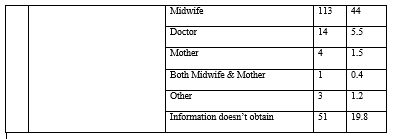
Table 5: knowledge of postnatal mothers on Danger Sign in Governmental Hospital of Harar Town, Feb 7 – 25, 2020 G.C
4.4 Over all knowledge level
The mean score of newborn care knowledge among the total sample was 12.59 (±3.16 SD). The maximum score obtained was 19.00 and the minimum score was 5.00. Considering the mean score of knowledge as the assigned cut-off point, 147 (57.2%) of mothers were found to have good knowledge of newborn care and 147 (57.2%) of mothers were found to have poor knowledge on newborn care. Thus make the overall prevalence of good knowledge in this study was 57.2% the rest 42.8% of participant had poor knowledge on essential new born care practices.
4.4 Factor associate with knowledge
Bivariate logistic regression analyses showed that among socio-demographic characteristics of clients Marital status, occupational status, number of ANC visit, age at first marriage were not statistically associated while Age educational status, Place of residence, Average Families monthly Income, ANC follow up, parity, and Time spent to reach hospital were associated with the outcome variables.
A multiple logistic regression statistical model analysis was performed in order to identify factors associated with knowledge on essential new born care among postnatal mother. Those P - value < 0.25 in Bivariate logistic regression were entered in to final multivariate analysis. After adjusting other variables, Educational status, Average Family monthly, Frequency of visit, Parity were independently associated with Knowledge on Essential new born care.
Those Postnatal women whose secondary educational level was 5 times (AOR = 5.938, CI: (1.943 – 18.144) more like having Knowledge than Unable to read and write. Postnatal mother whose average monthly income between 1000 – 2000 birr were 64.1% (AOR = 0.359, CI: 0.146 – 0.887) less likely knowledgeable than their encounter and those postnatal mothers who had three times ANC visit 69.7% (AOR = 0.303 CI: 0.096 – 0.995) less likely knowledgeable than those who less than 1000 birr. Postnatal mother who had Multi-para women had 2.8 times (AOR = 2.871 CI: 1.133 –7.273) more likely Knowledgeable than Primi-para Women (Table 6)
|
Characteristics |
knowledge level |
Crude OR (95%) |
P Value |
Adjusted OR (95%) CI |
|||||
|
poor knowledge |
Good knowledge |
||||||||
|
No (%) |
No (%) |
||||||||
|
Age |
|||||||||
|
18-24 Yrs |
47 (42.7) |
43 (29.3) |
1.00 |
0.435 |
1.00 |
||||
|
25-35 yrs |
48 (43.6) |
75 (51.0) |
1.708 (0.986 - 2.960)* |
0.496 |
0.736 (0.304 - 1778) |
||||
|
35- 40 yrs |
15 (13.6) |
29 (19.7) |
2.113 (1.000 - 4.465) |
0.628 |
1.346 (0.405 – 4.472) |
||||
|
Educational Status |
|||||||||
|
Unable to read & write |
53 (48.2) |
20 (13.6) |
1.00 |
0.000 |
1.00 |
||||
|
Able to read & write |
26 (26.6) |
36 (24.5) |
3.669 (1.758 -7541)* |
0.020 |
2.961 (1.185 – 7.400) |
||||
|
Primary education |
18 (16.4) |
23 (15.6) |
3.386 (1.517 -7559)* |
0.081 |
2.371 (0.898 – 6.258) |
||||
|
Secondary Education |
7 (6.4) |
26 (17.7) |
9.843 (3.693 -26.335)* |
0.002 |
5.938 (1.943 – 18.144)* |
||||
|
Widowed |
6 (5.5) |
42 (28.6) |
18.550 (6.873 -50.330)* |
0.000 |
15.015 (4.461 – 50.537) |
||||
|
Place of Residence |
|||||||||
|
Rural |
52 (47.3) |
122 (83.0) |
1.00 |
|
1.00 |
||||
|
Urban |
58 (52.7) |
25 (17.0) |
0.184 (0.104 -0.325)* |
0.104 |
0.479 (0.198 – 1.63) |
||||
|
Average monthly income |
|||||||||
|
Less than 1000 |
40 (36.4) |
66 (44.9) |
1.00 |
0.083 |
1.00 |
||||
|
1001 – 2000 |
25 (22.7) |
16 (10.9) |
0.388 (0.185 – 0.813)* |
0.026 |
0.359 (0.146 – 0.887)* |
||||
|
Greater or equal to 2001 |
45 (40.9) |
65 (44.2) |
0.875 (0.507 – 1512) |
0.270 |
0.665 (0.322 – 1.374) |
||||
|
ANC Follow up |
|||||||||
|
No |
28 (25.5) |
7 (4.8) |
1.00 |
0.531 |
0.629 (0.147 - 2.684) |
||||
|
Yes |
82 (74.5) |
140 (95.2) |
6.829 (2.856 – 16.332)* |
0.612 |
0.642 (0.115 - 3569) |
||||
|
Frequency of visit |
|||||||||
|
One |
10 (12.3) |
23 (16.3) |
1.00 |
0.241 |
|
||||
|
Two |
19 (23.5) |
37 (26.2) |
0.8847 (0.335 – 2137) |
0.122 |
0.405 (0.129 – 1.273) |
||||
|
Three |
30 (37.0) |
35 (24.8) |
0.5507 (0.209 – 1.233) |
0.042 |
0.303 (0.096 – 0.995)* |
||||
|
Four and above |
22 (27.2) |
46 (32.6) |
0.909 (0.370 – 2.235) |
0.173 |
0.450 (0.142 - 1.421) |
||||
|
Parity |
|||||||||
|
Primi-para |
50 (45.5) |
43 (29.3) |
1.00 |
|
|
||||
|
Multi para |
60 (54.5) |
104 (70.7) |
2.016 (1.202 - 3.379)* |
0.026 |
2.871 (1.133 –7.273)* |
||||
|
Time spent to reach hospital |
|||||||||
|
2-60 minute |
73 (66.4) |
124 (84.4) |
1.00 |
|
|
||||
|
60 - 300 minute |
37 (33.6) |
23 (15.6) |
0.366 (0.202- 0664)* |
0.865 |
1.091 (0.399 - 2983) |
||||
Table 6: Association of knowledge on newborn care with socio-demographic and other factors, among Postnatal Mothers in Harar Hiwot Fana Specialized University and Jugel Hospital Harar Eastern Ethiopia 2020 (N = 257)
5. Discussion
In our study 57.2% of the mothers had good knowledge our finding was relatively lower than study conducted in India 76.7 % [14] and Gulomekada Eastern Tigray 80.4 % [10]. This deference might be due to differences in the study setting and study period.
Regarding immunization in this study 72% of mothers were aware of the need to vaccinate their newborns at birth this finding is lower than study conducted in Adiss Ababa 96.1% [11] and in this study 36.2% and 44% of postnatal mothers reported that BCG and OPV will administer at birth to prevent TB and polio while this finding is lower than study conducted in Kenya showed that 17.8% [12]. This deference might be in our study area postnatal mother were not provide sufficient information during ANC time on immunization.
One of essential new born care component was early initiation of breast feeding in this study 79.3 % of mothers reported that their start breast feeding within the first hour after delivery which was slightly higher than study conducted in Pakistan [13] study showed that 66.2%. This deference might be due to variation in Socio-demographic
Regarding thermoregulation in this study 52.5 % replied that wrapped the baby in a cloth immediately important to maintain temperature and 42.4% only correctly identified the proper time of bathing which was after 24 hour of delivery. Our finding is lower than study conducted in Tigray 77.4 % and 77.4% [10]. This might be due to difference in socio- demographic as well as more emphasis was not given on providing education in our study area.
In this study 22.9% mothers mentioned that butter should be applied to the stump, this finding is lower than study conducted in Adiss 60 % [11] this deference might be due to participant in our study area had better knowledge on cord care practice.
In this study one of the factors significantly associated was educational status this was in line with study conducted in India [14] and Tigray [10] as well as udupi district [17] Tamil Nadu [15] and Bahir Dar City [18]
In this study parity had significantly associated with knowledge level which was in line with study conducted in Addis Ababa [12] while ANC visit does not have significant association.
In this study Residence, ANC follow up and occupational status had not significant association with knowledge of mothers on essential new born care. This finding was in line with study conducted in Tigray [10]
In this study time spent to reach hospital had no significant association with knowledge but in Himalayas among mothers who reported that their nearest health facility was less than one hour (30–59minutes) walking distance had higher odds of having adequate new born care knowledge [16]
6. Strength and limitation of the study
6.1 Strength
6.2 Limitation
7. Conclusion
The overall prevalence of good knowledge in this study was 57.2% the rest 42.8% of participant had poor knowledge on essential new born care practices. Among component of essential new born care majority of finding like, breast feeding initiation time, aware of the need to vaccinate, knowing that vaccines were given to prevent diseases, awareness of why BCG and OPV will administered, how to maintain thermoregulation, eye infection and its sign were much lower than study conducted in another area. On multivariable association Educational Status, Average monthly income, ANC visit and Parity had significantly associated with outcome variables.
8. Recommendation
Based on the findings from this study the following recommendations are made:
For Harari Regional Health Office
Better to have a close follow up on Maternal and new born care service
Maintain a strategy that will incorporate maternal education service on essential newborn care
Prepare and distribute posters that will describe essential new born care
Provide short-term training on newborn care especially to Health Extension Workers (health care service providers at home level),
Strength close monitoring system
For Health Institutions
Maternal education on essential newborn care was provide in the antenatal period
Better to put posters that will describe essential new born care practice.
Empowering women mechanism need to be established like improving educational status.
Maintain close monitoring method among staffs
For Those Health Professionals
Awareness creations need to be implement on new born care
Provide education on breast feeding mainly importance of clostrum feeding sass well as prelacteal feeding.
Better to provide details education on the importance of each vaccine
Give emphasis on cord care as it was prone for having infection.
The mothers should get continuous health education on this issue of newborn care by health care providers specially Health Extension Workers.
Further researches should be conducted on areas of essential newborn care to identify more gaps.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org