International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 5 - Issue 1 - 2025
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


T Karthikeyan1
1Associate Professor, Dept of Physiotherapy, Gurugram University, Gurugram, Haryana, India.
*Corresponding author: Dr.Karthikeyan T, PhD, DSC, Associate Professor, Dept of Physiotherapy, Gurugram University (A Govt University), Gurugram, Haryana, India.
Received: June 17, 2025
Accepted: June 21, 2025
Published: July 18, 2025
Citation: Karthikeyan T. (2025) “A Comparative Clinical Study of Vestibular and Neurodevelopmental Therapies for Balance Enhancement in Down Syndrome”. International Journal of Epidemiology and Public Health Research, 7(1); DOI:10.61148/2836-2810/IJEPHR/147.
Copyright: © 2025. T Karthikeyan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited., provided the original work is properly cited.
Introduction: Down syndrome, commonly known as Down syndrome, is a genetic disorder caused by an extra copy of chromosome 21. Children with this condition often present with various motor impairments including hypotonia, joint hypermobility, diminished reflexes, persistent primitive reflexes, and delayed postural reactions—all contributing to impaired balance and delayed motor development.
Purpose: This study aimed to evaluate and compare the therapeutic efficacy of vestibular stimulation (VS) versus neurodevelopmental therapy (NDT) in improving balance function among children with Down syndrome.
Methods: A total of 20 children diagnosed with Down syndrome were selected using purposive sampling and divided into two equal groups (n=10). One group received vestibular stimulation therapy while the other underwent neurodevelopmental therapy. The Pediatric Balance Scale (PBS) was used as the outcome measure to assess pre- and post-intervention balance performance.
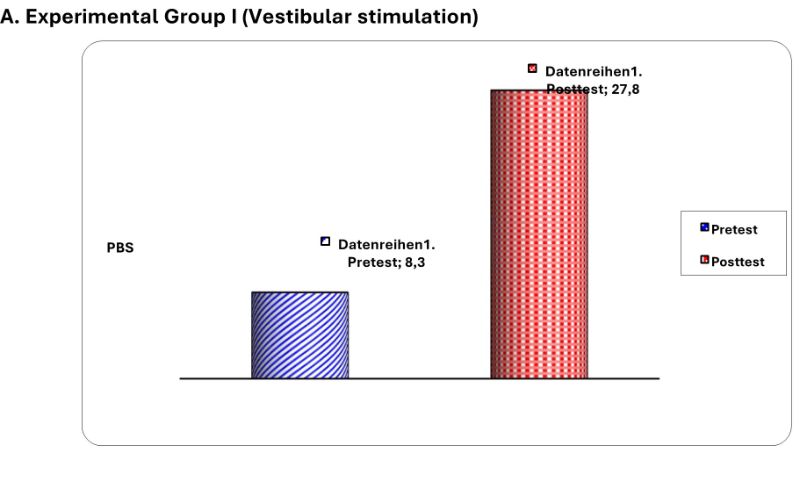
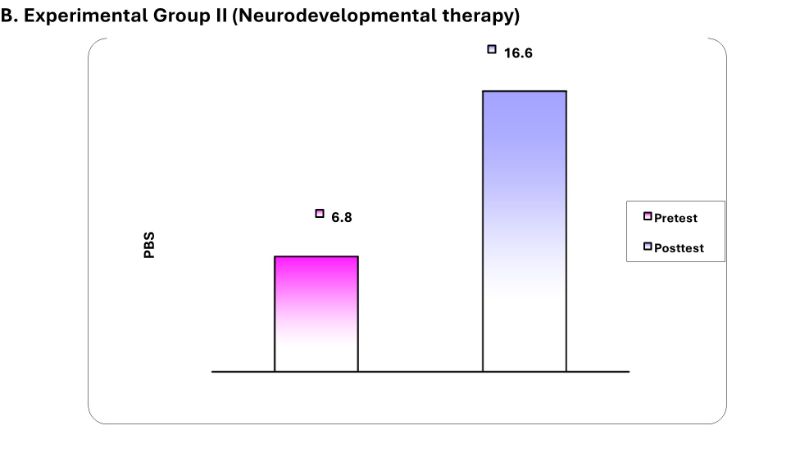
Results: The vestibular stimulation group showed a significant improvement, with mean PBS scores increasing from 8.3 (pre) to 27.8 (post), p < 0.05. The neurodevelopmental therapy group also demonstrated improvement, with scores increasing from 6.8 to 16.6, p < 0.05. However, the improvement was markedly greater in the vestibular stimulation group.
Conclusion: The findings suggest that vestibular stimulation is more effective than neurodevelopmental therapy in enhancing balance in children with Down syndrome. Incorporating vestibular-based interventions may thus provide greater benefits in managing balance dysfunction in this population.
Down syndrome is also referred to as Triosomy 21. It is a condition in which a person has an extra chromosome. Chromosomes are small “packages” of genes in the body2. They determine how a baby’s body forms and functions as it grows during pregnancy and after birth. Typically, a baby is born with 46 chromosomes. Babies with Down syndrome have an extra copy of one of these chromosomes, chromosome 21 2. A medical term for having an extra copy of a chromosome is Down syndrome.In children with Down syndrome there have been a few observed and measured motor characteristics such as hypotoncity, joint hypo mobility, decrease in deep tendon reflex, maintenance of primitive reflex and a delay in appearance of reaction timing and equilibrium reaction that may have contributed to delay development3.
Purpose: to find out the therapeutic efficacy of vestibular stimulation versus neurodevelopmental therapy for balance disorder of children with triosomy21.
Down syndrome was named after JOHN LANGDON DOWN the first physician to identify the syndrome. Down syndrome is the most common Chromosomal abnormality among live birth4. Down syndrome is the most frequent genetic cause of mild to moderate mental retardation and associated medical problem and occurs in 1 out of 800 live births in all races and economic groups5.
Down syndrome is characterized by a variety of dimorphic features, congenital malformation and other health problems and medical condition. Not all of them are present in each affected individual6.
In children with Down syndrome there have been several observed and measured motor characteristics such as hypotoncity, joint hypo mobility, decrease in deep tendon reflex, maintenance of primitive reflex and a delay in appearance of reaction timing and equilibrium reaction that may have contributed to delay development7.
The chromosomal basis of Down syndrome
Human body cell contains 23 pairs of chromosomes, half of which are inherited from each parent. Only the human reproductive cells, the sperm cells in males and the Ovum in females, have 23 individual chromosomes not pairs. These chromosome pairs as the xx pair present in females, and the xy pairs, present in males, and number them 1 through 228.
When the reproductive cells, the sperm and ovum combine at fertilization, the fertilized egg that results contain 23 chromosome pairs. A fertilized egg that will develop into a female contains chromosome pairs 1 through 22, and the xx pair. A fertilized egg that will develop into a male contains chromosome pairs 1 through 22, and the xy pair. When the fertilized egg contains extra material from chromosome number 21, this results in Down syndrome9.
Incidence of Down syndrome
Down syndrome rises with increasing maternal age.
For parents of a child with Down syndrome due to translocation Down syndrome, there may be an increased likelihood of Down syndrome in future pregnancies. This is because one of the two parents may be balanced carriers of the translocation 10.
Occurrence of Down syndrome
Occurrence of Down syndrome is due to a random event that occurred during formation of the reproductive cells, the ovum or sperm. The probability that another child with Down syndrome will be born in a subsequent pregnancy is about 1 percent, regardless of maternal age11.
AIM & NEED OF STUDY:
AIM OF STUDY
Aim of the study is to compare the effectiveness of Vestibular stimulation Vs Neurodevelopmental therapy in improving balance for children with Down syndrome12.
NEED FOR STUDY
In clinical setting Neurodevelopmental therapy is being usually given to improve balance for children with Down syndrome. Vestibular stimulation has shown promising result, and it is an approach that can be used to improve balance in children with Down syndrome by
normalization of extensor muscle tone and by the development of equilibrium reaction 14.
This study has been conducted to compare the effectiveness of vestibular stimulation with Neurodevelopmental therapy to improve balance for children with Down syndrome 13.
METHODOLOGY:
Study design
Pretest & posttest experimental study design
Sample Size
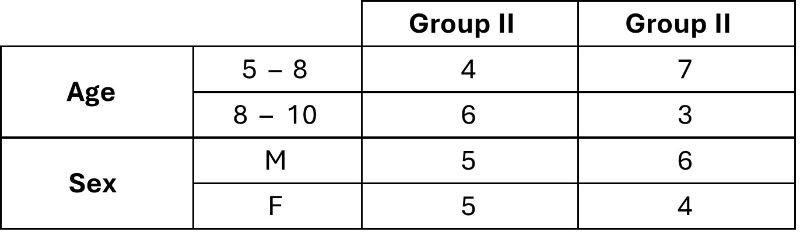
20 Children who fit into the inclusive criteria were taken. 10 patients were allotted for each group.
Sampling technique
Purposive sampling technique.
Study setting
Criteria for selection
Inclusive Criteria
Exclusive Criteria
Duration of study
4 months
Study Method
Experimental group I treated with vestibular stimulation
Two Group
Experimental group II treated with
Neurodevelopmental therapy.
Measurement Tool
Pediatric Balance Scale
Technique of Study
Experimental Group I
To find out the effect of vestibular stimulation in improving balance for children with Down syndrome.
Vestibular Stimulation
Duration of treatment - 45min
Repetition - 10 Rep/exercise
No.of section - 2 session / day No. of day/wee - 5 days / week
Exercise on trampoline
 Experimental Group II
Experimental Group II
To find out the effect of Neurodevelopmental therapy in improving balance for children with Down syndrome.
Neurodevelopmental therapy
Repetition - 10 Rep/exercise
No.of section - 2 session / day
No. of day/week - 5 days / week
Exercise on Swiss ball

DATA PRESENTATION:
|
|
|
|
|
|
|
S.No. |
PRE TEST |
POST TEST |
|
1 2 3 4 5 6 7 8 9 10 |
8 9 7 8 7 8 7 9 5 4 |
18 20 17 19 16 20 15 19 12 10 |
DATA ANALYSIS
Demographic Data
Tabulation: Paired‘t’ test
Level of significance: p<0.05 and significant
Level of significance: p<0.05 and significant
Unpaired ‘t’ test
A. Post test between Experimental Group I and Group II
Level of significance: p<0.05 and significant
GRAPHICAL PRESENTATION
Pediatric balance scale
Paired‘t’ test
Independent ‘t’ test
Post test of experimental group I & group II
 RESULT:
RESULT:
Paired‘t’ test
Pediatric balance scale
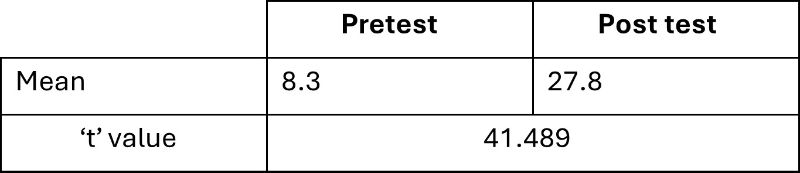
Experimental Group I (Vestibular Stimulation)
For 9 degrees of freedom at 5% level of significance the calculated ’t’ value is 41.489 which is greater than the table ‘t’ value 2.262. Hence alternate hypothesis is accepted.
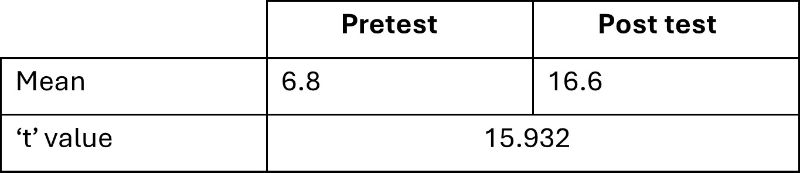
Experimental Group II (Neurodevelopmental therapy)
For 9 degrees of freedom at 5% level of significance the calculated‘t’ value is 15.932 which is greater than the table ‘t’ value 2.262. It shows there is significant difference between data. Hence alternate hypothesis is accepted.
Unpaired ‘t’ test
Pediatric balance scale
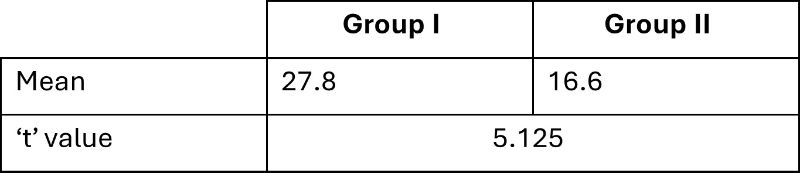
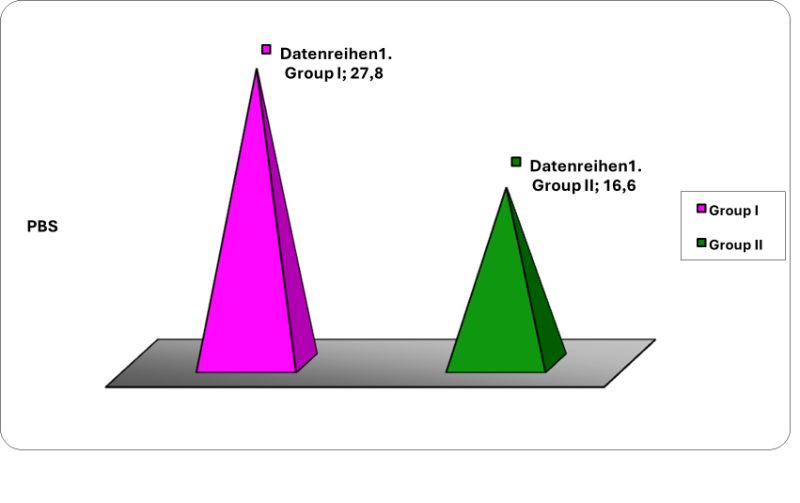
Post test value (Experimental Group I & II)
When the post-test value of experimental Group I and experimental
Group II were analyzed by unpaired ‘t’ test. The calculated ‘t’ value is 5.125. The table ‘t’ value at 5% level of 18 degree of freedom is 2.101 which is less than the calculated ‘t’ value. So, there is significant difference between two groups and hence alternate hypothesis is accepted.
DISCUSSION:
Down syndrome is the most common chromosomal abnormality among live birth15. In children with Down syndrome there have been several observed and measured motor characteristics such as delay in equilibrium reaction, hypotonicity, joint hypomobility, a delay in appearance of reaction timing16.
The study was conducted to compare the effectiveness of Neurodevelopmental therapy and Vestibular stimulation to improve balance in children with Down syndrome17.
The study comprised of two experimental group of 20 samples. They were included according to the inclusive and exclusive criteria18. The samples were selected using purposive sampling design. The samples were divided into two experimental groups where experimental group I received vestibular stimulation and experimental group II received neurodevelopmental therapy19. Pre and post test scores were noted according to the study design. Balance was assessed using pediatric balance scale20.
The statistical analysis was done using paired‘t’ test and independent‘t’ test. The results obtained after analysis showed there is significant improvement in group I treated with vestibular stimulation compared to group II treated with neurodevelopmental therapy and found that there is no significant difference between two groups.
The improvement is due to vestibular stimulation.
Reasons: -
CONCLUSION:
A balance disorder is a disturbance that causes an individual to feel unsteady or have a sensation of movement. An organ in our inner ear is an important part of our vestibular system.
The Vestibular system in the brain does more than just allow us to stand upright, maintain balance and move through space. Its co-ordinates information from the vestibular organ in the inner ear eyes, muscle, joints fingertips, palm of the hand, gravity receptors on the skin and adjust to heart rate, Blood pressure, muscle tone, limb position, arousal and balance.
Dysfunction in the vestibular system can cause abnormalities in muscle tone, difficulty defecating, need for self-stimulation etc. Exercises that activate wide range of inputs to the vestibular system have been found to be effective in reducing vestibular problem.
Physical therapy intervention like vestibular stimulation and neurodevelopmental therapy were given to selected patient 10 patient in each group.
Pretest, posttest scores are noted, and analysis was done using paired ‘t’ test and independent ‘t’ test statistical analysis shows that there is significant improvement in balance with both technique and vestibular stimulation is found to be more effective than neurodevelopmental therapy.
From this it can be concluded that vestibular stimulation can be incorporated to treat children with Down syndrome to improve balance. Further undergoing earlier management leads to better prognosis.
LIMITATION AND SUGGESTION:
‘pediatric clinical test of sensory interaction for Balance.
Conflict of Interest:
None
Acknowledgement:
My sincere thanks to Vice Chancellor, Registrar,DAA & Chairperson (Department of Physiotherapy) given the permission to conduct this study.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org