International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


William Nsemani1 ⃰, Fortress Yayra Aku2, Bismark Sarfo1, Charles Noora1, Donne Ameme1, Ernest Kenu1
1Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana.
2Department of Epidemiology and Biostatistics, Fred Binka School of Public Health, University of Health and Allied Sciences, Hohoe.
*Corresponding author: William Nsemani, Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana.
Received: June 01, 2026 | Accepted: June 15, 2026 | Published: June 20, 2026
Citation: Nsemani W, Fortress Y Aku, Sarfo B, Noora C, Ameme D, Kenu E., (2026) “Typhoid Fever Surveillance System Evaluation, WA Municipality, Ghana”. International Journal of Epidemiology and Public Health Research, 9(4); DOI: 10.61148/2836-2810/IJEPHR/204.
Copyright: © 2026. William Nsemani This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Typhoid fever is a bacterial infection caused by Salmonella typhi and transmitted through ingestion of contaminated food and water. The disease remains a public health concern in Ghana, as it leads to intestinal perforation, septic shock, and death. It is therefore a reportable disease placed under surveillance and requires periodic evaluation. We, therefore, evaluated the system to assess its attributes, usefulness, and whether it was meeting its objectives.
Methods: A descriptive cross-sectional design was used to evaluate the typhoid fever surveillance system for the period 2017 to 2021, in the WA municipality. The evaluation adopted the CDC updated guidelines to collect quantitative and qualitative data through interviews and records review. Data were analyzed using Microsoft excel and results were presented as frequencies, graphs and tables.
Results: Between 2017 and 2021, 16,552 suspected samples of typhoid fever were referred to the laboratory where 464 cases tested positive. The surveillance system helped to establish electronic reporting systems, sensitizing of food vendors on good food hygiene practices, and improved water and sanitation services in WA municipality. Regarding simplicity, 88% (30/34) of respondents knew the case definition of typhoid fever. All 100% (11/11) key informants interviewed said the surveillance system was flexible as it was able to adapt to any changes during the period under review. Majority 82% (28/34) of respondents accepted having participated in the surveillance system. Timeliness was averagely at 97.4% whilst representativeness of the surveillance system was at 100%. More than 90% of respondents indicated that the system was stable. Data completeness was 82% (70/85) in 17 sampled health facilities. The overall positive predictive value was 2.8%.
Conclusion: The surveillance system was useful, simple, flexible, acceptable, timely, representative, stable and of good data quality. However, the Positive predictive value (PPV) was low. Periodic refresher training is therefore recommended to improve PPV.
Surveillance system, Evaluation, Typhoid fever, WA municipality, Ghana
Les parasitoses intestinales constituent un problème de santé publique majeur, notamment dans les zones à ressources limitées (1,2). Elles sont responsables d’une morbidité significative et peuvent être asymptomatiques ou provoquer des diarrhées, malnutrition et complications chez les immunodéprimés (3,4). Typhoid and paratyphoid fever is a bacterial infection, transmitted through ingestion of food and water contaminated with faecal matter and it is caused by systemic infection with Salmonella enterica serovars Paratyphi A, B, and C (Marks et al., 2017). Salmonella is classified into two major groups: the invasive and the non-invasive. The invasive Salmonella, otherwise called typhoidal Salmonellae produce primarily bacteremia febrile illnesses, with prolonged high fever, headache, and malaise being characteristic symptoms (Koul et al., 1993). Without effective treatment, typhoid fevers can lead to altered mental states termed typhoid state (Verghese, 1985), ileus, gastrointestinal bleeding, intestinal perforation, septic shock, and death (Stanaway et al., 2019). The non-invasive Salmonella are termed non-typhoidal Salmonellae and are made up of Salmonella species, which usually cause gastroenteritis (Stanaway et al., 2019).
In Ghana, Typhoid fever is endemic and according to the study conducted by Global Burden of Disease (2017), it is estimated that, in 2017 alone, there were at least: 69,506 typhoid cases (230 cases per 100,000) and 973 typhoid deaths, 88,981 disability-adjusted life-years lost to typhoid fever (Institute of Health Metrics and Evaluation, 2019). It is also reported that most typhoid cases in Ghana occur in children under the age of 15 years old. A study conducted by the Typhoid Fever Surveillance in Africa Program (TFSAP) found that typhoid incidence rates among children below the age of 15 years in Asante Akim North, Ghana, were two times higher in children living in rural than those in urban areas with 636 versus 297 cases per 100,000, respectively (Espinoza et al., 2016) .
Ghana is currently implementing various preventive and control measures against typhoid fever and they include provision of clean water and sanitation, immunization of children under the age of 15 years (Jin et al., 2017); putting in place measures to prevent drug resistant strain of typhoid fever and strengthening the surveillance system of typhoid fever in the country. Typhoid fever is one of the diseases listed for surveillance according to the Integrated Disease Surveillance and Response (IDSR) strategy in Ghana because of its public health impact characterized by gradual onset of clinical features and the likely misdiagnosis of the disease due to the clinical picture similar to many other febrile illnesses such as malaria (Evans et al., 2004). Additionally, there is no documented evidence of an evaluation on typhoid fever in Wa municipality, hence the need for this evaluation to assess whether the typhoid fever surveillance system in Wa municipality was meeting its set objectives; assess its usefulness and its attributes.
Methods
Study design and area
This was a cross-sectional surveillance system evaluation conducted from 6th to 30th June, 2022, in Wa Municipality, Ghana, covering the period from January 2017 to December, 2021.
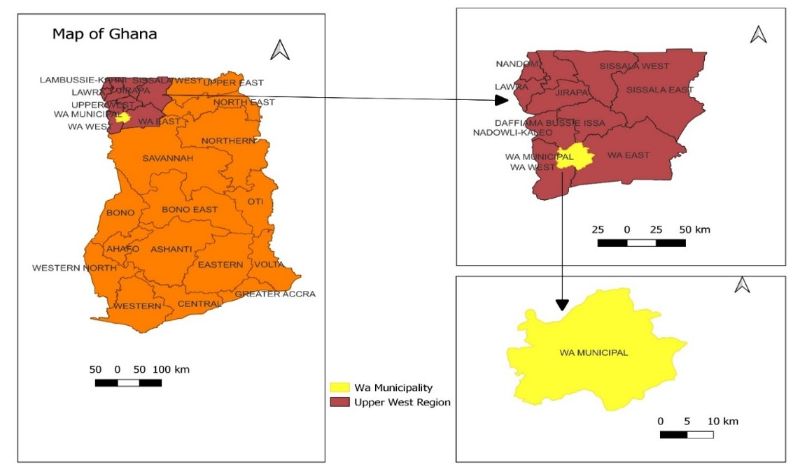
Figure 1: Map of evaluation site - WA Municipality, 2022 Data collection
Structured questionnaires were used to collect data from stakeholders through interviews and observational checklist of surveillance practice. Surveillance data were extracted from various databases such as District Health Information Management System – 2 (DHIMS - 2), Hospital Administration Management System (HAMS), monthly summary forms for notifiable diseases, annual reports, and reviews to establish whether the system was meeting its objectives in order to assess its usefulness.
Case definition
The standard case definition of typhoid fever was used to collect the data on typhoid fever during the evaluation of the typhoid fever surveillance system.
Table 1: Surveillance system attributes and indicators
|
Attribute |
Indicators/Means of assessment |
|
Simplicity |
This was assessed by finding out from stakeholders:
|
|
Flexibility |
Interviewed stakeholders at region and district on:
|
|
Acceptability |
|
|
Timeliness |
|
|
Representativeness |
|
|
Stability |
|
|
Data Quality |
|
|
Positive predictive value |
Data analysis
The collected data were analyzed using Microsoft Excel software and Epi Info version 7.2.5.0 and results were presented as frequencies and proportions.
Results
A total of thirty-four health staff were interviewed during the evaluation of which 59% (20/34) were males and 41% (14/34) were females. The median age of participants was 35.5 (IQR 26 – 46). Level of participation in the surveillance system at Community level was 9 (26.5%), at Health centre/clinic was 9 (26.5%), at Hospital level was 10 (29%), at Wa Municipality level was 2 (6%) and at regional level, it was 4(12%). The interview was conducted among health staff with different professional background: 17 (50%) of Nursing staff, 5 (14.7%) Medical Officers, 4 (11.8%) Physicians, 2 (5.9%) Disease control officers, 2 (5.9%) Health information officer, 2 (5.9%) Disease surveillance officers, 1 (2.9%) Medical laboratory and 1 (2.9%) Health assistant (Table 2).
Table 2: Demographic characteristics of study participants
|
Demographic characteristics |
Frequency (N=34) |
Percent (100) |
|
Sex Males Females |
20 14 |
59.0 41.0 |
|
Age 25 – 29 30 – 34 35 – 39 40 – 44 45 ≤ |
4 13 9 4 4 |
11.8 38.1 26.5 11.8 11.8 |
|
Level of participation Regional Municipality Hospitals Health Centres/Clinics CHPS |
4 2 10 9 9 |
12.0 6.0 29.0 26.5 26.5 |
|
Profession Nursing Medical officers Physicians Disease control officers Health information officers Disease surveillance officers Medical laboratory Health assistant |
17 5 4 2 2 2 1 1 |
50.0 14.7 11.8 5.9 5.9 5.9 2.9 2.9 |
The operation of typhoid fever surveillance system in Wa municipality begins at the lowest structure of the Ghana Health Services to the national level and beyond and feedback is given in the same order as indicated on figure 2.
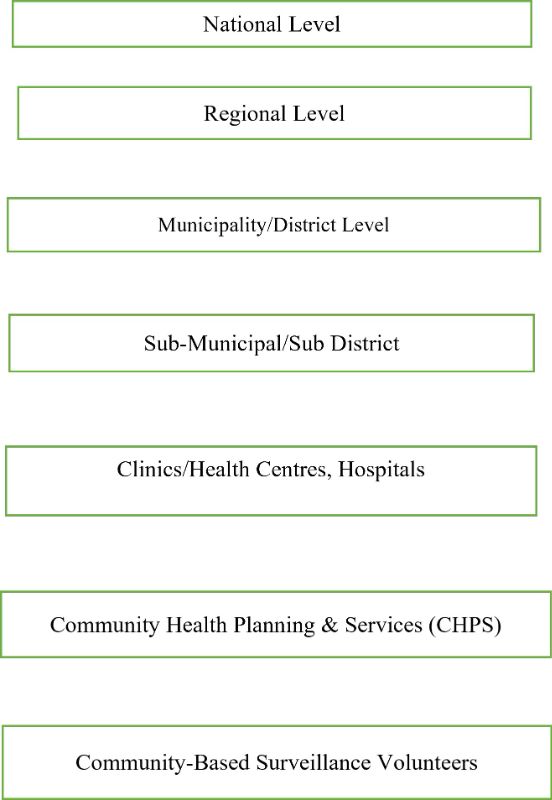
Figure 2: Operation of Typhoid fever surveillance system, Wa municipality, 2017 - 2021
The surveillance system was able to detect typhoid fever cases and outbreaks promptly, and seek laboratory verification (Fig 3).
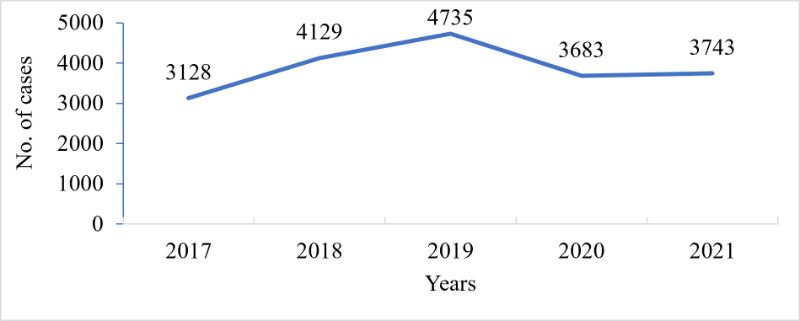
Figure 3: Typhoid fever trend, Wa municipal, 2017 - 2021
The surveillance system was also able to identify areas (Fig 4) and population at high risk (Fig 5).
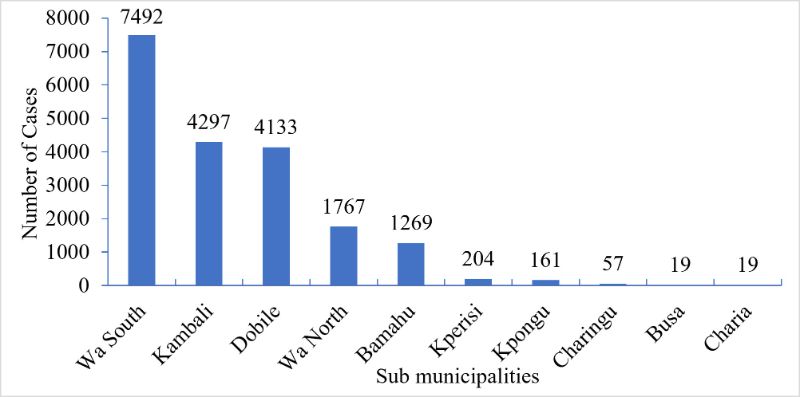
Figure 4: Distribution of typhoid fever cases in Wa Sub municipalities, 2017 – 2021
Table 3: Laboratory detected typhoid fever cases, Wa municipality, 2017 – 2021
|
Years |
Males |
Females |
Total Negatives |
Total Positives |
Total Cases |
||
|
|
-ve |
+ve |
-ve |
+ve |
|
||
|
2017 |
206 |
6 |
276 |
6 |
482 |
12 |
494 |
|
2018 |
453 |
12 |
605 |
23 |
1058 |
35 |
1093 |
|
2019 |
777 |
57 |
1011 |
71 |
1788 |
128 |
1916 |
|
2020 |
2387 |
59 |
3123 |
67 |
5510 |
126 |
5636 |
|
2021 |
3144 |
74 |
4106 |
89 |
7250 |
163 |
7413 |
|
Total |
6,967 |
208 |
9,121 |
256 |
16,088 |
464 |
16,552 |
The typhoid fever surveillance system demonstrated its usefulness by:
We also assessed the attributes of the typhoid fever surveillance system.
Simplicity
Majority 88% (30/34) of respondents knew the case definition of typhoid fever, 9% (3/34) had partial knowledge whilst 3% (1/34) did not know. On the other hand, most 80% (20/25) respondents indicated that capturing typhoid fever data took less than 5 minutes, 16% (4/25) said it took 5 to 10 minutes and then 4% (1/25) indicated that it took 10 to 20 minutes. With regard to reporting system, majority 92% (23/25) knew the reporting system of typhoid fever; 4% (1/25) did not know whilst 4% (1/25) was not sure.
Flexibility
All 100% (11/11) the key informants interviewed indicated that the surveillance system was flexible as it was able to adapt to any changes especially with the introduction of the SORMAS mobile app to collect data. The key informants included the Deputy regional director, Deputy regional director of nursing services, Municipal director, Hospital directors, Disease surveillance officers, Disease control officers and Health information officers.
Acceptability
Majority 82% (28/34) of the stakeholders participated in typhoid fever surveillance system and 18% (6/34) were not involved. The data extracted from 41 health facilities indicated that only 54% (22/41) facilities reported in 2017; 71% (29/41) reported in 2018; 66% (27/41) reported in 2019; 73% (30/41) reported in 2020 and 78% (32/41) reported in 2021 (Figure 5).
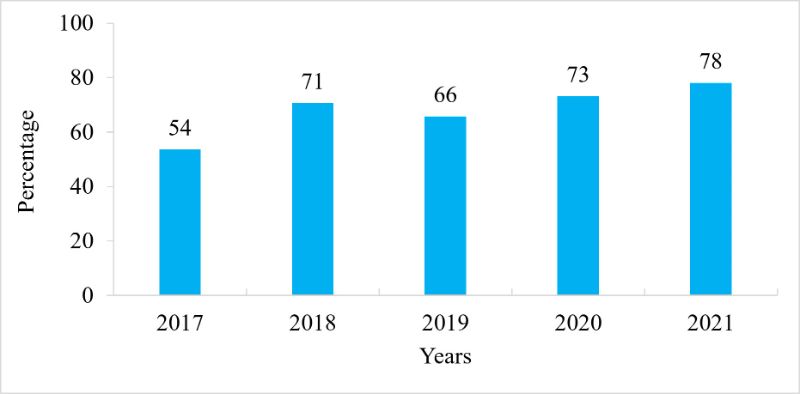
Figure 5: Reporting by facilities, WA municipality, 2017 – 2021
Timeliness
Out of 24 prescribers, 38% (9/24) said typhoid fever patients visited the health facility for treatment within 4 to 5 days of onset of their signs and symptoms; 25% (6/24) said it took 2 to 3 days; 21% (5/24) stated 6 to 7 days; 8% (2/24) said after 7 days whilst 8% (2/24) indicated that patients seek medical treatment within a day. The turnaround time for Widal test was 1 hour and 72 hours for Bacteriological test. The completeness of the data was at 100% while timeliness was on average at 97.4% during the period under review. This was far above the timeliness and completeness threshold reporting of 80% (Figure 6).
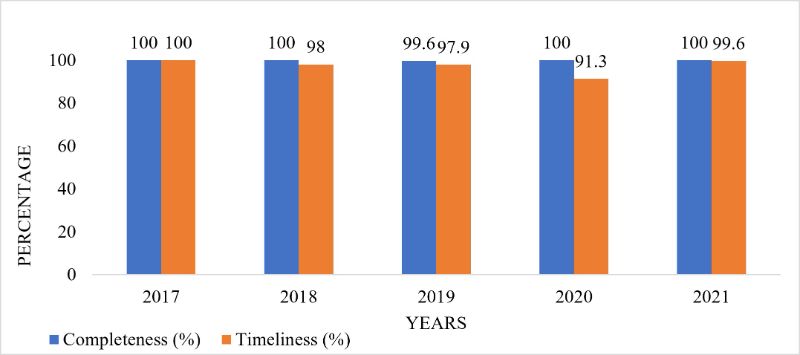
Figure 6: Completeness and timeliness, WA municipality, 2017 – 2021
Representativeness
All the 10 sub municipal health facilities in WA municipality were involved in the typhoid fever surveillance system (Table 4). And the age and sex distribution of total cases detected reflect the general distribution of the population in WA municipality (Table 5).
Table 4: Geographical representativeness of typhoid fever, WA municipality, 2017 - 2021
|
Sub municipal |
|
|||||
|
2017 |
2018 |
2019 |
2020 |
2021 |
Total |
|
|
Bamahu |
231 |
271 |
177 |
192 |
398 |
1269 |
|
Busa |
1 |
1 |
12 |
5 |
0 |
19 |
|
Charia |
10 |
8 |
0 |
0 |
1 |
19 |
|
Charingu |
0 |
42 |
0 |
13 |
2 |
57 |
|
Dobile |
872 |
870 |
1213 |
493 |
685 |
4133 |
|
Kambali |
301 |
1143 |
1112 |
867 |
874 |
4297 |
|
Kperisi |
0 |
0 |
35 |
88 |
81 |
204 |
|
Kpongu |
17 |
16 |
23 |
52 |
53 |
161 |
|
Wa North |
259 |
356 |
477 |
408 |
267 |
1767 |
|
Wa South |
1437 |
1422 |
1686 |
1565 |
1382 |
7492 |
|
Total |
3128 |
4129 |
4735 |
3683 |
3743 |
19418 |
Table 5: Typhoid fever representativeness by age and sex, WA municipality, 2018 – 2021
|
Year |
Sex/ Age |
1-11 mths |
1-4yrs |
5-9yrs |
10-14yrs |
15-17yrs |
18-19yrs |
20-34yrs |
35-49yrs |
50-59yrs |
60-69yrs |
70+ |
Total |
|
2018 |
Male |
0 |
1 |
62 |
21 |
9 |
7 |
158 |
87 |
32 |
13 |
18 |
408 |
|
Female |
0 |
4 |
40 |
26 |
9 |
7 |
229 |
141 |
55 |
33 |
33 |
577 |
|
|
2019 |
Male |
0 |
33 |
145 |
77 |
22 |
19 |
236 |
136 |
52 |
29 |
28 |
777 |
|
Female |
0 |
21 |
89 |
68 |
17 |
13 |
385 |
207 |
93 |
55 |
59 |
1007 |
|
|
2020 |
Male |
0 |
425 |
339 |
125 |
56 |
31 |
585 |
324 |
130 |
80 |
90 |
2185 |
|
Female |
0 |
353 |
296 |
119 |
51 |
37 |
1012 |
465 |
241 |
184 |
176 |
2934 |
|
|
2020 |
Male |
49 |
761 |
303 |
132 |
39 |
36 |
542 |
286 |
178 |
86 |
100 |
2512 |
|
Female |
43 |
537 |
221 |
98 |
83 |
98 |
1114 |
462 |
280 |
140 |
157 |
3233 |
|
|
|
Totals |
92 |
2135 |
1495 |
666 |
286 |
248 |
4261 |
2108 |
1061 |
620 |
661 |
13633 |
Stability
Regarding the stability of the typhoid fever surveillance system, 97% (33/34) of respondents said the system was able to operate smoothly despite interruptions to power supply system, 94% (32/34) indicated that the system was able to operate smoothly within the available funds and human resources in Wa municipality.
Data Quality
A total of 85 case based forms were sampled from 17 health facilities for completeness from 2017 to 2021 and of this number, 70 were completed, giving the data completeness of 82% across all the 17 health facilities.
Positive predictive value (PPV)
The overall positive predictive value (PPV) for the typhoid fever surveillance system was 2.8% during the period under review. There was a total number of 16,552 cases of suspected typhoid fever recorded out of which 464 cases tested positive. The positive predictive value was assessed by considering that number of suspected cases of typhoid fever recorded in the last 5 years divided by the number of cases confirmed by the laboratory (Table 6).
Table 6: Positive Predictive Value
|
Years |
Males |
Subtotal |
Females |
Subtotal |
Total Negatives |
Total Positives |
PPV |
||
|
|
-ve |
+ve |
|
-ve |
+ve |
|
|
|
|
|
2017 |
206 |
6 |
212 |
276 |
6 |
282 |
482 |
12 |
2.4% |
|
2018 |
453 |
12 |
465 |
605 |
23 |
628 |
1058 |
35 |
3.2% |
|
2019 |
777 |
57 |
834 |
1011 |
71 |
1082 |
1788 |
128 |
6.7% |
|
2020 |
2387 |
59 |
2446 |
3123 |
67 |
3190 |
5510 |
126 |
2.2% |
|
2021 |
3144 |
74 |
3218 |
4106 |
89 |
4195 |
7250 |
163 |
2.2% |
|
Total |
6,967 |
208 |
7175 |
9,121 |
256 |
9,377 |
16,088 |
464 |
2.8% |
Discussion
We evaluated the typhoid fever surveillance system to establish whether it was meeting its set objectives, its usefulness and attributes. Between 2017 and 2021, the surveillance system detected 19,418 suspected cases of typhoid fever and of this number, 16,552 samples were sent to the laboratory for confirmation and 464 cases tested positive. However, the annual reports did not document any outbreak during the period under review. The highest number of cases were reported from Wa South sub municipal with 7492, followed by Kambali sub municipal with 4297, Dobile recorded 4133, Wa North reported 1767 cases, Bamahu recorded 1269, Kperisi recorded 204, Kpongu had 161 cases, Charingu reported 57, Busa and Charia sub municipals both recorded the lowest number of cases with each having 19 cases. Through typhoid fever surveillance data, several actions were taken within the period under review and this proved the usefulness of the system.
In this evaluation, 88% (30/34) of the respondents understood the case definition of typhoid fever lower than 98.8% in the typhoid fever surveillance system evaluation conducted in Egypt (Refaey, 2018). The surveillance system that is simple would enable every member of the system to easily contribute to the operation of the system. With regard to flexibility, the present evaluation established that all 100% (11/11) key informants interviewed said the surveillance system was flexible as it was able to adapt to any changes during the period under review. This finding was in agreement with the surveillance system evaluation conducted in Republics of the former Soviet Union (Wuhib et al., 2002). Flexibility of the system is important as it allows the system to be reviewed by adding necessary information to it or removing some parts of the system that hinders its smooth operation (Mushtaq et al., 2020). In the current evaluation, we found timeliness of reporting to be on average 97.4% for all reporting facilities which meets the target timeliness according to the IDSR compared to 80% timeliness in the evaluation system of the notifiable diseases such as typhoid fever conducted in Zimbabwe (Mairosi et al., 2017). Meeting the targeted timeliness is a good asset for the typhoid fever surveillance system as it suggests that stakeholders have accepted the system and are participating in it. It also means the system is alert and may timely detect any outbreak (Kalil et al., 2021). In terms of acceptability, 82% of stakeholders participate in typhoid fever surveillance system higher than 25% in notifiable disease surveillance system evaluation conducted in South Africa (Benson et al., 2016). The participation of the stakeholders in the surveillance system shows their willingness to accept the system and this promotes effectiveness and efficiency in its operation (Benson et al., 2016). The representativeness of the typhoid fever surveillance system was 100% as the system was able to represent its population by location, age and sex. This finding was to the surveillance system evaluation conducted in Republics of the former Soviet Union (Wuhib et al., 2002). A system that is well representative is a good sign of inclusion of every member of the population it is targeting to serve (Mushtaq et al., 2020).
More than 90% of respondents indicated that the typhoid fever surveillance system was stable as it was able to operate with the available financial, human resources and power supply system slightly higher than 85.5% stability in the typhoid fever surveillance evaluation system conducted in Egypt (Refaey, 2018). A stable surveillance system is important as it is able to collect, manage and provide data without failure using the available financial and human resources and able to operate during unscheduled power outages. Data completeness was 82% (70/85) in 17 sampled health facilities compared to 92% in the evaluation of notifiable disease surveillance system conducted in Zimbabwe (Mairosi et al., 2017). Data completeness is a good indicator of proper data quality. The implication of poor data quality of the surveillance system is that wrong decisions and policies would be made at all levels of decision making instead of addressing the actual problem (Awekeya et al., 2021). In the current typhoid fever surveillance system evaluation, the overall positive predictive value (PPV) was 2.8% similar to the positive predictive value (PPV) of 2.7% on the study of typhoid fever conducted in Ethiopia (Wasihun et al., 2015) but lower than PPV of 50% obtained from the typhoid fever surveillance system evaluation conducted Egypt (Refaey, 2018). The low PPV in this evaluation would mean that the disease is low in the population under the surveillance. This would also mean that the intervention measures that have been put in place are working (Nsubuga et al., 2017).
Conclusion
The typhoid fever surveillance system in Wa municipality meets its set objectives and was also useful. The system was simple, flexible, acceptable, timely, representative and stable. However, there was data inconsistency at health facility and low positive predictive value of the system
Recommendations
Acknowledgements
We acknowledge Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana for financial and technical support during the surveillance system evaluation activity. We further thank Upper West Regional Office and Wa Municipality Directorate for their support. We are grateful to Ms. Fortress Yayra Aku for her mentorship throughout the evaluation process.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org