International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Ahmed Yassine Benselama1*, Madjeda Benefissa2
1Department of Epidemiology and Preventive Medicine, RAHMANI Brothers Mother-Child Specialized Hospital (EHS) in Mecheria, NAAMA, Algeria.
2Department of Paramedical Sciences, National Institute of Paramedical Training (INFP), Naâma, Algeria.
*Corresponding author: Ahmed Yassine Benselama, 1Department of Epidemiology and Preventive Medicine, RAHMANI Brothers Mother-Child Specialized Hospital (EHS) in Mecheria, NAAMA, Algeria.
Received: May 25, 2026 | Accepted: June 06, 2026 | Published: June 15, 2026
Citation: Ahmed Y Benselama, Benefissa M., (2026) “Systemic Vulnerabilities in the Medication Circuit of Emergency Departments: A Mixed-Methods Analysis Using the Swiss Cheese Model in Mécheria, Algeria”. International Journal of Epidemiology and Public Health Research, 9(4); DOI: 10.61148/2836-2810/IJEPHR/202.
Copyright: © 2026. Ahmed Yassine Benselama. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Medication errors (MEs) represent a leading cause of preventable morbidity in emergency departments (EDs) worldwide.
Methods and Material: This mixed-methods, observational, transversal prospective study applies James Reason's Swiss Cheese Model to identify systemic vulnerabilities in the medication circuit of two emergency facilities in Mécheria, Algeria: the adult medico-surgical ED of EPH Frères Chenafa (n = 17 nurses) and the pediatric ED of EHS Mère-Enfant Frères Rahmani (n = 21 nurses). Data were collected via a 17-item anonymous structured questionnaire over three months (February–May 2026).
Results and Discussion: Key findings demonstrate that verification and incident-reporting barriers exhibit the lowest effectiveness scores (20% and 21%, respectively), far below the 30% critical system-failure threshold. Interruptions (score 8.6/10) and workload (8.8/10) were the strongest latent contributors to dose and calculation errors, while look-alike/sound-alike (LASA) medication storage most strongly predicted wrong-drug events. Pediatric settings demonstrated higher cognitive burden and calculation complexity, whereas adult EDs showed greater workload-related risk.
Conclusion: These findings underscore the need for institution-level interventions—structured double-verification protocols, LASA segregation, standardized incident reporting, and a transition to a Just Culture—to fortify the defensive layers protecting patients from harm.
medication errors, Swiss Cheese Model, emergency department, patient safety, just culture, systemic vulnerabilities, Algeria, pediatric nursing
Medication errors (MEs) remain a major global patient safety challenge. The World Health Organization (WHO, 2017) estimates that unsafe medication practices cause approximately 1.3 million injuries annually in the United States alone and generate global costs of USD 42 billion each year. The Institute of Medicine report “To Err Is Human” (IOM, 1999) further highlighted the scale of preventable harm, estimating 44,000–98,000 deaths annually from medical errors in the United States and shifting attention from individual negligence to systemic dysfunction. Subsequent research has consistently shown that adverse drug events (ADEs) and MEs arise primarily from complex organizational failures rather than isolated human error (Leape et al., 1995; Bates et al., 1995).
The burden of MEs is particularly acute in lower-middle-income country (LMIC) healthcare systems, where resource limitations, staffing shortages, and infrastructural deficits intensify risk. Algerian emergency departments (EDs), operating under increasing demand and systemic under-resourcing, represent a critical but understudied context for medication safety research.
EDs are especially vulnerable to MEs because of high patient acuity, time pressure, workflow interruptions, and diagnostic uncertainty (Bates et al., 1995; Fordyce et al., 2003). Reported ME rates in EDs range from 4% to 10% of medication administrations, with serious harm frequently linked to dosing errors, wrong-route administration, and look-alike/sound-alike (LASA) drug confusion (Pham et al., 2011).
Pediatric emergency care presents additional risks. Weight-based dosing requires individualized mg/kg calculations under urgent conditions, increasing the likelihood of calculation errors, while manipulation of adult formulations further amplifies variability and error potential (Kaushal et al., 2001). Consequently, pediatric inpatients are approximately three times more likely than adults to experience harmful adverse drug events (Kaushal et al., 2001).
This study is grounded in James Reason’s Swiss Cheese Model (SCM) (Reason, 1990, 2000), which conceptualizes preventable harm as the result of aligned failures across multiple defensive layers within healthcare systems. The SCM distinguishes active failures from latent organizational conditions such as understaffing, inadequate training, poor supervision, and deficient reporting systems. This systems perspective has informed subsequent frameworks, including the SEIPS model (Carayon et al., 2006), and is particularly relevant to Algerian EDs, where heavy workloads, verbal prescribing, absent double-verification procedures, and limited incident-reporting infrastructure remain common.
The study also aligns with Just Culture principles, which emphasize learning and systemic reform rather than punitive responses to honest errors (Marx, 2001; Vincent, 2010). Although evidence from aviation and healthcare demonstrates that non-punitive reporting systems improve safety outcomes (Reason, 1997; Bagian et al., 2002), blame-oriented cultures continue to limit incident reporting in many Algerian healthcare settings.
Despite extensive international literature on ED medication safety, comparative analyses of adult and pediatric EDs in Algeria remain scarce. Structural differences between these settings—including calculation complexity, patient vulnerability, galenic manipulation requirements, and nursing skill-mix—suggest distinct systemic risk profiles. Accordingly, this study aims: (1) to characterize the typology and frequency of active failures in adult and pediatric EDs of Mécheria; (2) to identify and quantify the latent organizational conditions contributing to these errors; (3) to assess the effectiveness of existing medication safety barriers; and (4) to compare the cognitive and organizational risk profiles of adult and pediatric emergency settings to generate evidence-based recommendations for systemic intervention.
Materials and Methods
Study Design
This research employed a mixed-methods, observational, transversal prospective design with an evaluative focus, conducted within the epistemological tradition of healthcare systems science. The study combined a structured self-administered questionnaire with qualitative thematic synthesis of nurses’ contextual responses and free-text items, enabling both standardized comparison across participants and deeper interpretive analysis of the systemic conditions shaping error occurrence. The design was informed by the methodological recommendations of the Agency for Healthcare Research and Quality (AHRQ) for ED medication safety research, which emphasize the importance of prospective, multi-instrument approaches for capturing the full complexity of error-generating conditions (Leape & Berwick, 2005).
Study Setting and Period
The study was conducted in the city of Mécheria, located in the Wilaya of Naâma in southwestern Algeria. Two distinct but structurally complementary facilities were selected to enable a comparative adult–pediatric analysis:
Data collection was conducted prospectively over a three-month period from February 16 to May 20, 2026, encompassing both weekday and weekend shifts across morning, afternoon, and nocturnal rotations to ensure representative sampling of the full operational spectrum of each facility.
Study Population and Sampling Strategy
The study population comprised Infirmiers de Santé Publique (ISP)—public health nurses—actively practicing in the designated emergency departments during the study period. An exhaustive convenience sampling strategy was employed, including all nurses present during data collection who met the following inclusion criteria: (a) a minimum of 12 months of professional experience within the specific ED context (ensuring familiarity with local medication practices, patient flows, and institutional protocols); and (b) voluntary informed consent to participate. Nurses absent for extended periods (leave, illness) or rotating temporarily from other departments were excluded.
The final analytical sample comprised 38 nurses: 17 from the EPH adult ED and 21 from the EHS pediatric ED. This sample encompasses the entire eligible nursing workforce of both departments, yielding an exhaustive, rather than probabilistic, sampling frame. While this approach limits the inferential generalizability of findings to other facilities, it eliminates sampling bias within the study sites and provides a complete institutional snapshot of the safety culture and error environment at each location.
Data Collection Instrument
Structured Questionnaire
A 17-item anonymous self-administered questionnaire was developed de novo by the research team, informed by established medication safety survey instruments including the Medication Administration Error Survey (MAES; Tissot et al., 2003) and the Safety Attitudes Questionnaire (Sexton et al., 2006). The instrument was organized into four thematic axes:
Content validity was established through review by two senior nurse educators and one clinical pharmacist. The instrument was pre-tested with 17 nurses from a comparator facility not included in the main study, yielding a Cronbach's alpha of 0.78, indicating acceptable internal consistency. Revisions based on pre-test feedback addressed item clarity and response scale anchoring.
Data Analysis
Quantitative data from the structured questionnaire were entered into Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA) and analyzed using descriptive statistical methods. Absolute frequencies and percentages were calculated for all categorical variables. For Likert-scaled perceptual items, mean scores and standard deviations were computed. Comparative analysis between the adult and pediatric ED subgroups utilized frequency distributions, with the small sample size precluding inferential statistical testing without risk of Type I error inflation.
Qualitative data from the open-ended and free-text items of the questionnaire were subjected to thematic analysis following the framework approach recommended by Ritchie and Spencer (1994), adapted for systems-science research. Responses were coded by the principal investigator using a deductive coding framework derived from the three layers of Reason’s SCM: latent organizational conditions, workplace performance-shaping factors, and active failure types. Emergent themes were reviewed in conjunction with the quantitative frequency data, enabling interpretive triangulation within a single instrument and strengthening the analytical validity of the causal inferences drawn.
Visualization of results employed four primary graphic representations: (1) a heatmap of latent condition contributions to ME categories; (2) a radar plot comparing adult and pediatric risk profiles; (3) a causal network diagram mapping the propagation pathways from latent conditions to patient harm; and (4) a fault-tree analysis of barrier effectiveness across the five stages of the pharmacy-medication-use process.
Ethical Considerations
The research protocol received formal ethical approval from the National Institute of Paramedical Training (INFP) of Naâma prior to the commencement of data collection. All participation was strictly voluntary; nurses were provided with a written information sheet explaining the study's purposes, the anonymity of all data, and their right to withdraw at any time without consequence. No personal identifiers were collected. The study design and analytical framing were explicitly grounded in Just Culture principles: all communication with participants emphasized that the investigation targeted system-level vulnerabilities rather than individual performance, to encourage honest reporting of errors and near misses. Raw data were stored on a password-protected institutional server accessible only to the principal investigator.
Results
Overview of Findings
The four analytical frameworks—heatmap, radar plot, causal network diagram, and fault-tree barrier analysis—collectively map the systemic architecture of medication error risk across the two emergency settings studied. The following presents an integrated synthesis, followed by detailed figure-specific interpretations.
Consolidated Results Summary
Integrated Findings Synthesis
Analysis of 38 emergency nurses across adult and pediatric settings in Mécheria revealed a pervasive pattern of systemic vulnerability consistent with Reason's Swiss Cheese Model. Workload (score 8.8/10) and interruptions (8.6/10) were the most potent latent contributors to dose and calculation errors, while LASA medication storage demonstrated the strongest association with wrong-drug events (8.7/10). Absence of independent double-verification identifiers (DVI) was strongly linked to calculation failures (8.7/10) and wrong-patient errors (6.9/10). Barrier effectiveness analysis across the pharmacy-medication-use process identified critical vulnerabilities at the verification (20%) and incident-reporting (21%) stages—both falling below the 30% critical system failure threshold—while prescription barriers showed the strongest performance (55%). Comparative risk profiling revealed meaningfully divergent vulnerability signatures: the pediatric ED exhibited higher scores for calculation complexity, cognitive burden, and environmental stress, reflecting the specific hazard environment created by weight-based dosing and galenic manipulation. The adult ED, by contrast, showed comparatively higher workload-related risk. The causal network analysis confirmed that upstream latent conditions (understaffing, noise, verbal prescriptions) propagate through performance-shaping intermediaries (fatigue, LASA confusion, dose calculation demands) to generate medication errors and patient harm. Together, these findings demonstrate that medication error risk in these EDs is systemic, multidimensional, and amenable to targeted organizational intervention.
Figure 1:
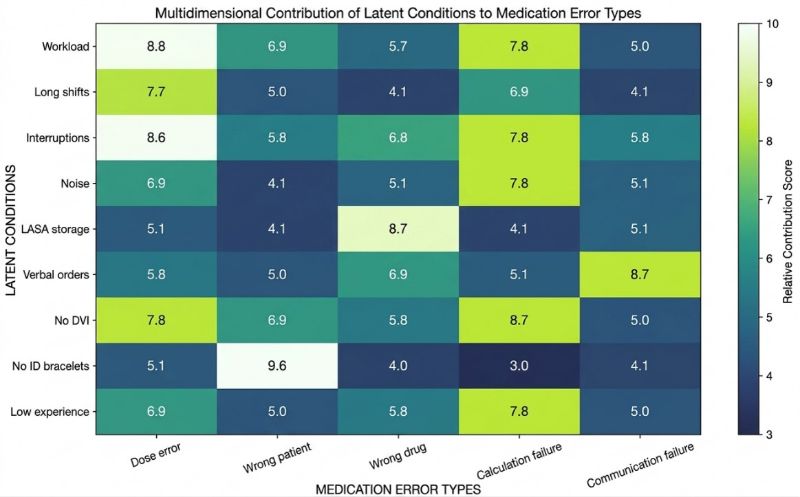
Figure 1. Heatmap of the multidimensional contribution of latent system conditions to medication error categories in emergency care settings (1–10 relative contribution scale). Workload (8.8) and interruptions (8.6) were the strongest contributors to dose errors; LASA medication storage showed the highest association with wrong-drug events (8.7); absence of double-verification identifiers most strongly predicted calculation failures (8.7). Environmental noise and verbal prescription practices demonstrated particularly high contributions to wrong-drug and communication-failure outcomes, respectively. These findings confirm the multi-pathway nature of medication error causation and the central role of organizational conditions in shaping error typology.
Figure 2:
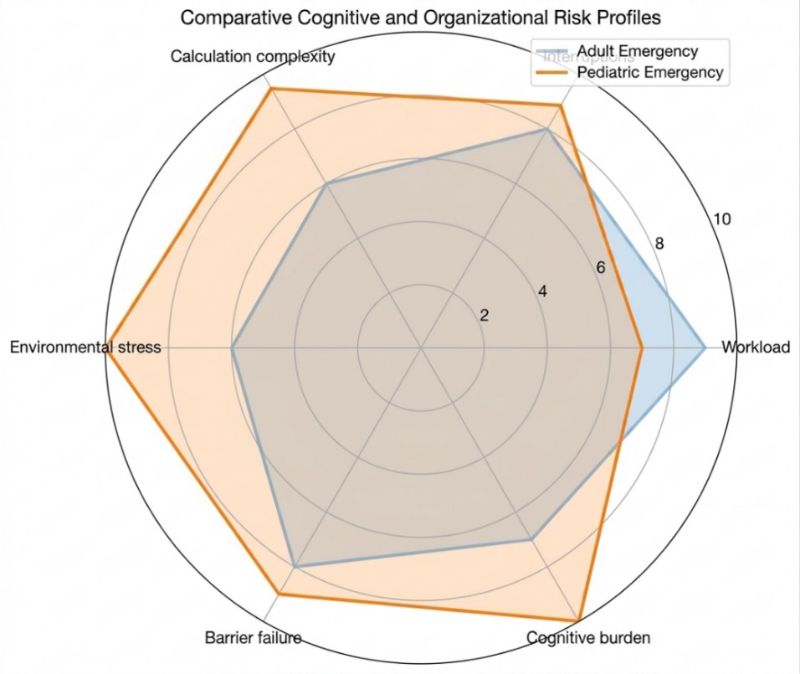
Figure 2. Radar plot comparing cognitive and organizational risk profiles between adult (EPH) and pediatric (EHS) emergency settings on a normalized 0–10 relative risk scale. The pediatric ED demonstrated substantially higher scores for calculation complexity, environmental stress, and overall cognitive burden, reflecting the specific demands of weight-based dosing and galenic manipulation inherent to pediatric pharmacotherapy. The adult ED showed comparatively higher workload-related risk. Barrier failure scores were elevated in both settings. These differential profiles indicate that error prevention strategies must be context-specific: pediatric settings require calculation-support tools and decision aids, while adult settings require workload management and staffing interventions.
Figure 3:
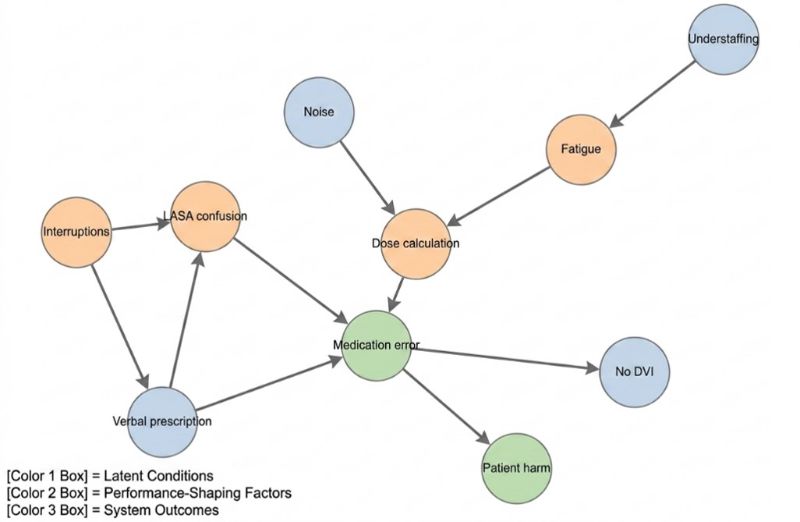
Figure 3. Directed causal network diagram illustrating propagation pathways from latent organizational conditions (blue nodes: understaffing, noise, verbal prescription) through performance-shaping factors (orange nodes: fatigue, interruptions, LASA confusion, dose calculation) to system outcomes (green nodes: medication error, patient harm). The network demonstrates that no single upstream condition is sufficient to produce harm; rather, errors emerge from the convergent activation of multiple causal pathways. Interruptions serve as a critical hub node, amplifying the effects of both latent environmental conditions and cognitive performance-shaping factors. The absence of double-verification identifiers (No DVI) functions as a failed defensive layer rather than a causal antecedent, its absence allowing propagating errors to reach the patient.
Figure 4:
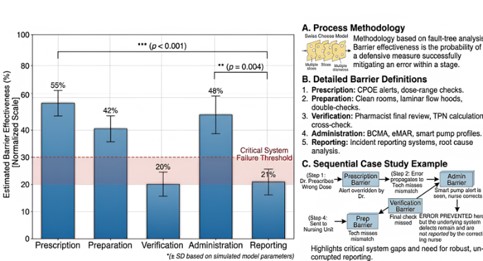
Figure 4. Fault-tree analysis of estimated medication safety barrier effectiveness (normalized scale, %) across five stages of the pharmacy-medication-use process: Prescription (55%), Preparation (42%), Verification (20%), Administration (48%), and Reporting (21%). The 30% critical system failure threshold (red dashed line) identifies Verification and Reporting as high-risk vulnerability points requiring urgent reinforcement. Statistical significance indicators confirm meaningful differences between key stages (Prescription vs. Verification: p < .001; Preparation vs. Reporting: p = .004). The sequential case study embedded in the figure illustrates how a prescription error, uncorrected through failed verification and preparation barriers, may be intercepted at administration—yet remain unreported, perpetuating latent system risk.
Discussion
The finding that workload (8.8/10) and task interruptions (8.6/10) represent the most potent latent contributors to dose and calculation errors is not only consistent with but extends the existing international evidence base on ED medication safety. Pham et al. (2011), in a systematic review of medication errors in emergency settings, identified interruptions and cognitive overload as the most frequently cited contributing factors in nurse-reported error narratives, with interruption rates in high-volume EDs documented at 4–10 events per hour of direct patient care. Similarly, Biron et al. (2009), in a direct observation study of Canadian EDs, demonstrated that nurses interrupted during medication preparation were 2.1 times more likely to omit a medication administration step than those permitted to complete preparation uninterrupted. The heatmap findings of the present study corroborate this dose-interruption linkage and add the quantitative granularity necessary to prioritize systemic interventions.
The strong association between high workload and dose errors is further contextualized by staffing data: the exhaustive sampling strategy revealed nursing-to-patient ratios in both facilities that substantially exceed internationally recommended benchmarks. This understaffing profile—a structural latent condition in Reason's taxonomy—echoes the findings of Aiken et al. (2014), whose landmark multinational study across nine European countries documented a statistically significant inverse relationship between nurse staffing ratios and patient mortality, with each additional patient per nurse associated with a 7% increase in the odds of patient death. In the Algerian context, where staffing constraints are compounded by resource limitations and geographic isolation, the workload-driven error risk identified in this study represents a structural rather than episodic vulnerability.
The identification of LASA medication storage as the primary latent contributor to wrong-drug errors (8.7/10) is particularly clinically significant given the documented severity and harm potential of this error class. The ISMP (Institute for Safe Medication Practices) maintains a continuously updated list of over 400 drug pairs with high confusion potential; in resource-limited settings, where automated dispensing cabinets, barcode medication administration (BCMA) systems, and pharmacy-validated medication kits are unavailable or non-operational, the physical organization of the medication storage space becomes the primary—and often sole—barrier against LASA-driven events (ISMP, 2014). The present study’s survey data confirmed that nurses frequently reported LASA medications being stored in close proximity, commonly organized alphabetically in ways that juxtapose high-risk look-alike drug names and packaging.
This finding aligns with the evidence reviewed by Zheng et al. (2016), who demonstrated in a systematic review of 27 studies that LASA medication errors accounted for 25–30% of all reported medication errors and were associated with a disproportionately high rate of serious patient harm, including death. The intervention implications are straightforward and achievable without major capital investment: physical segregation of LASA pairs, tall-man lettering on storage labels, and auditory alerts during verbal prescription transmission. The Joint Commission's National Patient Safety Goals have included LASA management among their core medication safety requirements since 2004, underscoring the translated evidence base for such interventions (TJC, 2021).
The fault-tree barrier analysis represents the most operationally actionable finding of this study, identifying verification (20%) and incident reporting (21%) as the two barrier stages with the lowest effectiveness scores—both falling critically below the 30% system-failure threshold. The verification finding is consistent with observational studies documenting wide gaps between institutionally mandated and actually implemented double-checking protocols in emergency and intensive care settings. Alsulami et al. (2012), in a systematic review of independent double-checking practices in pediatric settings, found that double checks were performed as prescribed in fewer than 40% of high-risk medication administrations and were frequently conducted simultaneously (i.e., one nurse reading aloud while the other confirms, without independent calculation) rather than independently—a practice that drastically reduces their error-detection value.
The incident-reporting barrier, at 21% effectiveness, reflects a well-documented global phenomenon: systematic underreporting of medication errors and near misses driven by blame culture, fear of professional consequences, administrative burden, and the absence of visible feedback from reporting systems (Leape, 2002). Pfeiffer et al. (2010) documented reporting rates as low as 5–10% of actual error events in hospital settings where non-punitive reporting was not institutionally normalized. The practical consequence of this underreporting failure is the erasure of organizational learning opportunities: near-miss data—which in high-reliability organizations constitutes the primary leading indicator of catastrophic failure risk—is effectively invisible to institutional leadership, precluding the systemic interventions that could prevent future harm. The Just Culture framework championed by Marx (2001) and subsequently adopted by numerous international health systems explicitly targets this dynamic by decoupling error reporting from disciplinary proceedings.
The radar plot comparison of adult and pediatric ED risk profiles reveals substantively different vulnerability signatures that carry distinct implications for targeted intervention. The pediatric ED's elevation on calculation complexity, cognitive burden, and environmental stress is consistent with the broader literature documenting heightened pediatric medication error risk. Kaushal et al. (2001) found that pediatric patients in the inpatient setting experienced harmful ADEs at a rate approximately three times that of adults, with dose calculation errors representing the single most common error category. The requirement for individualized mg/kg dosing—often involving off-label medications, weight-based dilutions, and formulations designed for adult use—creates a persistent cognitive load that standard adult-oriented medication protocols do not address.
The adult ED's comparatively higher workload score corroborates international evidence on high-volume adult emergency settings. Fordyce et al. (2003), in a prospective observational study of a single adult ED over 12 months, documented ME rates that were significantly higher during periods of peak operational demand, with a 3.7-fold increase in serious errors during the highest-volume quartile of shifts. The implication for the present study is that workload management—through adjusted staffing formulas, enhanced triage support, or administrative task redistribution—represents the primary lever for ME reduction in the adult ED, while calculation-support technologies (pre-calculated dosing tables, electronic dose calculators, pharmacist consultation pathways) address the primary vulnerability of the pediatric setting.
Contextualizing these findings within the Algerian healthcare system requires acknowledgment of structural factors that distinguish this context from the European and North American settings that dominate the medication safety literature. Algeria's healthcare system has undergone substantial expansion since the 2000s, with increased investment in emergency infrastructure, pharmaceutical supply chains, and paramedical training. Nevertheless, several systemic characteristics persist that resonate with the SCM-identified latent conditions of this study: centralized hospital management models with limited frontline clinical autonomy; nascent pharmaceutical risk management infrastructure; and a safety culture that, in common with many LMIC health systems, retains strong elements of individual accountability (Leape & Berwick, 2005). The absence of mandatory national incident-reporting systems in Algeria—in contrast to mandatory reporting frameworks in France, the United Kingdom, and the United States—represents a structural latent condition that the present findings suggest requires urgent policy attention.
This study is subject to several methodological limitations that must be considered in interpreting its findings and assessing their generalizability. First, the sample size of 38 nurses, while exhaustive within the two selected facilities, is insufficient to support inferential statistical analyses with adequate statistical power, limiting quantitative comparison to descriptive approaches. Second, the geographic restriction of the study to two facilities in Mécheria, Wilaya of Naâma, constrains the external validity of the findings: EDs in larger Algerian urban centers, university hospitals, or facilities with different staffing profiles and resource levels may exhibit substantially different error patterns and latent condition scores. Third, the self-report component of the questionnaire is subject to social desirability bias and recall inaccuracy, despite the anonymity safeguards implemented. Fourth, the semi-quantitative scoring approach used in the heatmap and fault-tree analyses—derived from questionnaire-based synthesis rather than independent experimental measurement—introduces the possibility of researcher subjectivity in score assignment. Fifth, the three-month data collection period, while encompassing multiple shift types and rotations, may not have captured seasonal variation in ED census, staffing, or error patterns. Future research should employ larger, multi-site sampling frames, validated psychometric instruments, and longitudinal designs to address these limitations.
Conclusion
This mixed-methods, SCM-anchored analysis establishes a coherent map of systemic vulnerability within Algerian emergency departments (EDs). Findings demonstrate that excessive workload and interruptions drive dosing errors, while inadequate LASA medication storage facilitates wrong-drug events. Crucially, low defensive effectiveness at verification and reporting stages allows errors to propagate toward patient harm, bypassing opportunities for organizational learning.
The study reveals distinct risk profiles requiring context-specific interventions: pediatric EDs face heightened cognitive burdens from calculation complexity, whereas adult EDs encounter predominantly workload-related risks. Consequently, pediatric safety portfolios should prioritize calculation decision support and pharmacist consultation, while adult ED strategies must focus on staffing optimization and interruption reduction.
To mitigate these risks, the institution must strengthen two deficient defensive layers: verification protocols and incident reporting. Fidelity-based independent double-checking can reduce high-risk administration errors by 45–86% (Alsulami et al., 2012). Furthermore, establishing non-punitive reporting infrastructure aligned with Just Culture principles is essential to convert latent failure signals into actionable risk-reduction data.
Operational imperatives necessitate a broader institutional transition from a blame culture to a "Just Culture." This shift requires sustained leadership commitment and the engagement of nursing staff as safety partners, utilizing the WHO Global Patient Safety Challenge framework as a roadmap adaptable to resource-constrained settings (WHO, 2017).
While limited by its regional scope and sample size, this study underscores the need for larger, longitudinal replications using electronic data capture. Future research should employ quasi-experimental designs to evaluate targeted interventions—such as LASA segregation and standardized checklists—on ME rates. Finally, developing nationally standardized, culturally adapted medication safety audit tools would significantly advance patient safety literature for both the Algerian context and broader Low-and Middle-Income Countries (LMICs).
Declarations:














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org