International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Yohanna Puwu Markus*, Jonathan Ngutyo Uever, Charles Gabriel Iortimah
Department of Human Kinetics and Health Education, Faculty of Education, Rev. Fr. Moses Orshio Adasu University Makurdi, Benue State, Nigeria.
*Corresponding author: Yohanna Puwu Markus, Department of Human Kinetics and Health Education, Faculty of Education, Rev. Fr. Moses Orshio Adasu University Makurdi, Benue State, Nigeria.
Received: May 02, 2026 | Accepted: May 11, 2026 | Published: May 15, 2026
Citation: Yohanna P Markus, Jonathan N Uever, Charles Gabriel Iortimah., (2026) “Influence of Parents’ Residential Location and Level of Knowledge of Vaccine Preventable Diseases on The Acceptance of Childhood Immumization in The North-East Zone, Nigeria”. International Journal of Epidemiology and Public Health Research, 9(3); DOI: 10.61148/2836-2810/IJEPHR/199.
Copyright: © 2026. Yohanna Puwu Markus. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Childhood immunization is the process whereby a person is made immune or resistant to an infectious disease, typically by the administration of a vaccines. This study investigated influence of parents’ residential location and level of knowledge of vaccine preventable diseases on the acceptance of childhood immunization in Northeast Nigeria. The study adopted a cross-sectional descriptive survey design involving 400 parents of children under five years, using two step sampling procedure. Data were collected using a researcher-developed instrument titled “Influence of Parents’ Residential Location and level of knowledge of Vaccine-preventable diseases on Childhood Immunization Acceptance Questionnaire (IPRLLKV-PDCIAQ)”, which was validated by experts and pilot-tested for reliability. Out of the 400-questionnaire administered, 392 (98%) were correctly completed and successfully retrieved for analysis. Data were analysed using descriptive statistics and binary logistic regression at a significance level of p < .05. Results revealed that overall parental acceptance of childhood immunization was moderate at 52.8%. Residential location revealed that urban parents had the highest acceptance (77.3%), with urban residence significantly increasing the likelihood of acceptance (OR = 18.670, 95% CI: 9.370–37.186, p < .001). Knowledge of vaccine-preventable diseases was a powerful predictor; parents with good knowledge had 94.6% acceptance rate (OR = 141.270, 95% CI: 55.375–356.943, p < .001). The study concludes that improving parental knowledge, alongside addressing geographical location gaps, are critical for boosting immunization uptake in Northeast Nigeria. Targeted health education, community engagement, and context-specific outreach programmes are recommended to close acceptance gaps and strengthen child health outcomes in the region.
Acceptance, Childhood immunization, Residential location, Knowledge, Vaccine preventable diseases
Globally, childhood immunization remains a proven strategy for reducing child morbidity and mortality from vaccine-preventable diseases. However, the success of childhood immunization depends on the level of its acceptance by the parents whose personal variables such as location and knowledge of vaccine- preventable diseases play a major role. This is because Parents basically decide whether their children would receive immunization.
Immunization is a process whereby an individual is given vaccination either by oral or injection method to increase natural immunity against infectious diseases most especially among children [1]. Childhood immunization refers to the process of protecting children from serious infectious diseases by increasing body resistance to external infectious diseases and its effects [2].
In Nigeria, the National Programme on Immunization (NPI) now part of the National Primary Health Care Development Agency (NPHCDA) oversees childhood immunization under the broader Expanded Programme on Immunization (EPI), which is supported by WHO and UNICEF. The schedule for the immunization in Nigeria covers at birth (BCG for Tuberculosis, OPV 0 for Oral Polio Vaccine, Hepatitis B (Birth dose), 6 weeks (OPV 1, Pentavalent 1 for DPT-HepB-Hib), PCV 1 for Pneumococcal and Rotavirus 1), 10 weeks (OPV 2, Pentavalent 2, PCV 2, Rotavirus 2), 14 weeks (OPV 3, Pentavalent 3, PCV 3, Inactivated Polio Vaccine), 6 months (Vitamin A supplementation), 9 months (Measles-Rubella 1, Yellow Fever), 12 months (Measles-Rubella 2, Meningitis A) and from 6 months to 5 years (Vitamin A supplementation every 6 months). These vaccines stimulate the child's immune system to recognize and fight specific pathogens, providing immunity without causing the disease itself [3].
The success of childhood immunization in any nation depends on several factors including parental acceptance. Parental acceptance of childhood immunization refers to the willingness of parents or guardians to have their children receive recommended vaccines according to national or international immunization schedules [4]. They further explained that, the acceptance of childhood immunization to a significant extent depends on parental personal variables including parent’s location of residence and knowledge of vaccine-preventable diseases.
Parents’ location of residence (rural or urban) could influence the acceptance of childhood immunization due to differences in access to healthcare services, education, and exposure to health information and immunization programmes, which can lead to low vaccination rates [5]. According to Cuesta, et al “higher percentage of partially vaccinated children live in rural areas, (22.5%) did not receive any vaccination compared to urban areas (9.3%). This difference can be attributed to inadequate skill health care workers, lower knowledge of vaccine-preventable diseases and routine immunization among rural mothers [6]. They added that parents in rural areas may have less access to information about vaccines and their benefits, which can lead to lower vaccine uptake. UNICEF, 2019, revealed that, transportation to vaccination clinics can be difficult, especially for families with limited resources [7].
Parental knowledge of vaccine-preventable diseases refers to the understanding that parents or guardians have knowledge about diseases that can be prevented through vaccination. This includes parents’ awareness of what the diseases are (e.g., measles, polio, diphtheria), how they are transmitted, their potential severity and complications, and the role vaccines play in preventing the diseases [8]. Parental knowledge on acceptance of vaccination is a major player on the decision to utilize immunization programmes.
The purpose of this study was therefore, to examine influence of parents’ residential location and level of knowledge of Vaccine-preventable diseases on acceptance of childhood immunization in North-East Zone, Nigeria. Specifically, the study sought to answer the following questions:
Research Questions
Hypotheses
The following hypotheses were formulated to guide the study and were tested at 0.05 Alpha level.
Methods
The study setting is North-East geopolitical zone of Nigeria, the most populous zone in Nigeria, with an estimated population of over 28 million people or 13. 6% of the country’s population. Northeast Zone currently has 6 states. These states are further divided into local government areas, and each local government area is divided into wards. The Northeast Zone people are multi-ethnic, multicultural and multi-religious.
This research was carried out between May and August, 2025 in rural, semi-urban and urban settings in two states, Adamawa and Bauchi in northeast, Nigeria. Rural area in term of immunization, is defined as settlements challenges in logistics, geographical accessibility that create barriers to accessing health services such as increase travel time to clinics, lower population density and lower utilization of routine immunization, semi -urban area is defined as a settlement bridging the gap between urban and rural settings, characterized by mix of infrastructure, intermediate population density, and unique vaccination challenges, and urban settlement is defined as a highly populated density, diverse demographics and distinct, often fragmented health services. We selected these two states based on simple random selection. Two local government areas was also randomly selected from each senatorial district within the 2 sample states of the zone, making a total of 12 local government areas, and 3 wards was also randomly selected in each sampled local government areas in this study. These is to ensure at least moderate representation is achieved.
The population of the study comprise of all parents’ (heads of household) in North East zone of Nigeria. The parents ‘of 5,742,118 in this study was drawn from the 2006 National Population Census of 28,710,587 people as projected from the 6 states of the zone. The 5,742,118 was derived by dividing the geographical zone total population by 5.0, using the region’s average household size of 5.0, according to the Harmonized Nigeria Living Standard Survey [13].
This study utilized the cross-sectional survey research design. This design permits the description of parents’ residential location and level of knowledge of Vaccine-preventable diseases on acceptance of childhood immunization in North-East zone of Nigeria in their natural setting. A sample of 400 parents were selected through a proportionate stratified random sampling using the Taro Yamane sample size Formula [12].
The instrument for data collection was researchers-developed and validated questionnaire named “Influence of Parents’ Residential Location and level of knowledge of Vaccine-preventable diseases on Childhood Immunization Acceptance Questionnaire (IPRLLKV-PDCIAQ)”
Reliability of the instrument was ensured using Cronbach Alpha Statistic which yielded a reliability coefficient index of 0.78 indicating a substantial reliability and was used for data collection. A total of sixty (60) copies of questionnaire were randomly distributed to the respondents in Jalingo, state secretariat which is outside the sampled local government. The data collected was analyzed using the Statistical Package for the Social sciences (SPSS) to further ascertain the reliability of the instrument.
Out of the 400 questionnaires that were administered, 392 (98%) were correctly completed and successfully retrieved for analysis. Frequency counts and percentages were used to answer research questions, while hypotheses were tested using Binary Logistic Regression Analysis at .05 Alpha level.
We selected and trained two health workers as research assistants for each local government to assist in the administration of questionnaire to respondents and collection within two weeks at different local government areas of the northeast zone, Nigeria. The questionnaire was administered to the respondents using household visit and the respondent was identified as a parent who is the household head and with a child under 59 months as of the eligible criteria for respondents. The respondents in most cases were required to complete the questionnaire for immediate collection. However, those questionnaires that were unable to be completed instantly due to any unavoidable situation, the research assistants were given an option to reselect eligible household around the cluster or revisit the selected household to complete the questionnaire.
Results.
These discussions included the analysis of proportion of parental acceptance of childhood immunization in North-East Nigeria, in Table 1. Finally, the analysis of Parents’ knowledge of vaccines preventable diseases in Table 3 and parents’ residential location Table 4.
Research Question One: What is the proportion of parental acceptance of childhood immunization in North-East Nigeria? This research question is answered using Table 1.
Table 1: Proportion of Parental Acceptance of Childhood Immunization in North-East Nigeria (n = 392)
|
S/N |
Question on Parental acceptance of childhood Immunization |
Yes |
No |
Proportion of Acceptance (%) |
|
3 |
Would you accept your child receiving all the recommended vaccines? |
274 |
118 |
69.9 |
|
4 |
Would you accept a vaccine for your child even if others in your community do not? |
147 |
245 |
37.5 |
|
5 |
Would you accept to take your child to a health facility when a vaccination is due? |
229 |
163 |
58.4 |
|
6 |
Would you accept vaccination for your child during mass immunization campaigns? |
212 |
180 |
54.1 |
|
7 |
Would you accept your child being vaccinated in school? |
135 |
257 |
34.4 |
|
8 |
Would you accept your child being vaccinated during immunization outreach programs? |
272 |
120 |
69.4 |
|
9 |
Would you accept to return for follow-up vaccine doses for your child? |
234 |
158 |
59.7 |
|
10 |
Would you accept to vaccinate your child even when access requires traveling long distances? |
102 |
290 |
26.0 |
|
11 |
Would you accept healthcare worker advice about immunizing your child? |
263 |
129 |
67.1 |
|
12 |
Would you accept encouraging another parent to vaccinate their child? |
95 |
297 |
24.2 |
|
13 |
Would you accept continuing with your child’s immunization as scheduled by health authorities? |
273 |
119 |
69.6 |
|
14 |
Would you accept your child being vaccinated even during illness if advised by a health professional? |
289 |
103 |
73.7 |
|
15 |
Would you accept your child receiving vaccines provided during emergency health campaigns? |
262 |
130 |
66.8 |
|
16 |
Would you accept bringing your child for vaccination even when you are busy or tired? |
132 |
260 |
33.7 |
|
|
Mean |
207 |
185 |
52.8 |
Table 1 showed various proportions of parental acceptance of childhood immunizations in the North-East.
Overall, the proportion of parental acceptance of childhood immunization in North-East Nigeria stood at 52.8%, indicating that just over half of the surveyed population were generally receptive to immunizing their children.
Research Question Two: How does parents’ residential location influence their acceptance of childhood immunization in North East Nigeria? This research question is answered using Table 2.
Table 2: Descriptive Analysis on Influence of Parents’ Residential Location on Acceptance of Childhood Immunization (n = 392)
|
Residential Location |
Accepted Immunization n (%) |
Did not Accept Immunization n (%) |
|
Rural (n = 91) |
14 (15.4) |
77 (84.6) |
|
Semi-urban (n = 156) |
115 (73.7) |
41 (26.3) |
|
Urban (n = 145) |
112 (77.2) |
33 (22.8) |
Table 2 shows how parents’ residential location influence their acceptance of childhood immunization in Nigeria’s North-East. Among parents living in rural areas (n = 91), only 14 (15.4%) accepted childhood immunization, while a substantial majority, 77 respondents (84.6%) did not. This indicates a low level of childhood immunization acceptance in rural communities. In contrast, acceptance was markedly higher among parents residing in semi-urban areas (n = 156). Here, 115 respondents (73.7%) accepted childhood immunization, and 41 (26.3%) did not. This reflects a considerable improvement in childhood immunization acceptance compared to rural areas. The highest level of acceptance was observed among parents residing in urban areas (n =145), where 112 respondents (77.2%) accepted childhood immunization, and only 33 (22.8%) did not. This suggests that urban residence is associated with a stronger acceptance of childhood immunization services.
Figure Stacked Bar Chart Showing Influence of Parental Residential Location on Acceptance of Childhood Immunization.

Figure 3 is a vertical stacked bar chart illustrating the relationship between parental residential location and acceptance of childhood immunization. The chart compares three residential categories: rural, semi-urban, and urban. In rural areas, only 15.4% of parents accepted childhood immunization. In contrast, acceptance was much higher in semi-urban and urban areas, with 73.7% and 77.2% respectively. This figure demonstrates that parents living in semi-urban and urban areas were more likely to accept childhood immunization compared to those in rural areas, suggesting that parental residential location influences acceptance of childhood immunization in North-East Nigeria.
Research Question Three: How does parental knowledge level regarding vaccine-preventable diseases influence their acceptance of childhood immunization in Nigeria’s North East? This research question is answered using Table 3.
Table 3: Descriptive Analysis on Influence of Parental Level of Knowledge Regarding Vaccine-preventable Diseases on Acceptance of Childhood Immunization (n = 392).
|
Level of Knowledge |
Accepted Immunization n (%) |
Did not Accept Immunization n (%) |
|
Poor (n = 136) |
15 (11.0) |
121 (89.0) |
|
Fair (n = 127) |
104 (81.9) |
23 (18.1) |
|
Good (n = 129) |
122 (94.6) |
07 (5.4) |
Table 3 presents data on influence of parental knowledge of vaccine-preventable diseases on acceptance of childhood immunization among 392 respondents in North-East Nigeria. Among parents with poor knowledge (n = 136), only 11.0% (n = 15) accepted childhood immunization, while a substantial 89.0% (n = 121) did not. In contrast, among those with fair knowledge (n = 127), childhood immunization acceptance rose markedly to 81.9% (n = 104). This demonstrates that even a moderate level of knowledge of vaccine-preventable diseases substantially improves childhood immunization acceptance.
The highest childhood immunization acceptance rate was observed among parents with good knowledge of vaccine-preventable diseases (n = 129), where 94.6% (n = 122) accepted childhood immunization and only 5.4% (n = 7) did not.
Figure 2: Clustered Bar Chart Showing Influence of Parental Knowledge of Vaccine-preventable Diseases on Acceptance of Childhood Immunization.
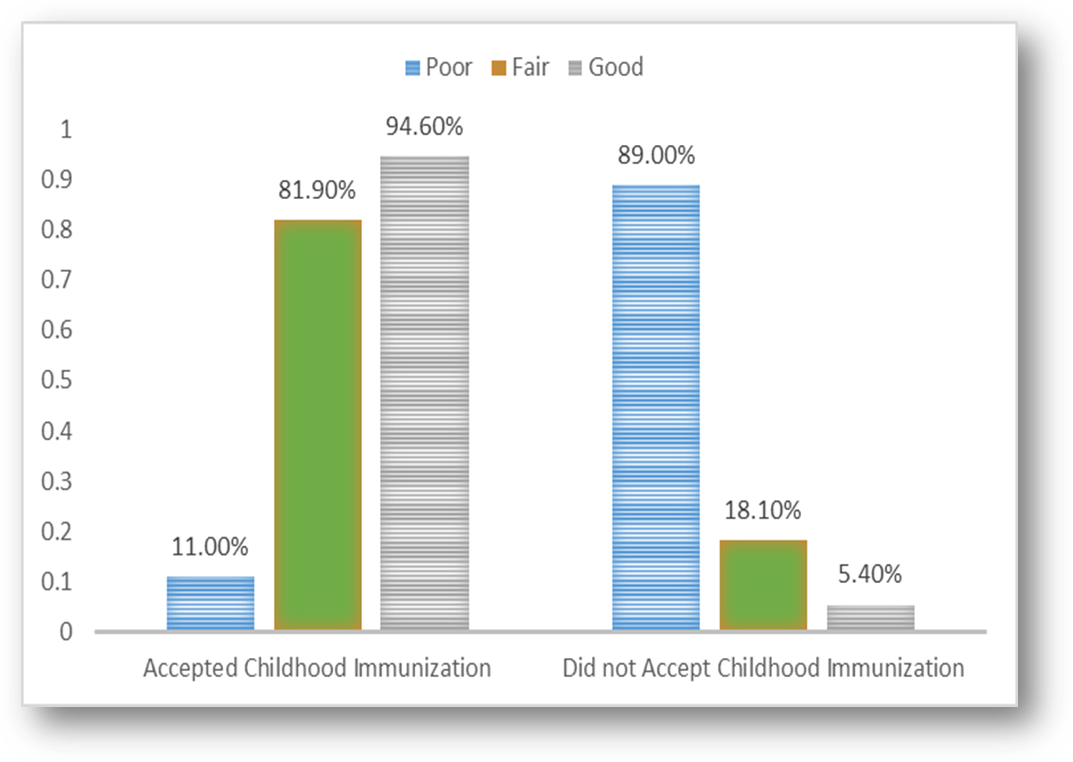
Figure 2 is a clustered bar chart illustrating the percentage distribution of childhood immunization acceptance based on parental level of knowledge regarding vaccine-preventable diseases. Among parents with poor knowledge, only 11.0% accepted childhood immunization. For those with a fair level of knowledge, 81.9% accepted childhood immunization and Parents with good knowledge of vaccine-preventable diseases demonstrated the highest acceptance rate at 94.6% accepting childhood immunization. The chart clearly illustrates that as parental knowledge increases, so does the likelihood of accepting childhood immunization.
Hypothesis One: Parents’ residential location has no significant influence on acceptance of childhood immunization in North -East, Nigeria. This hypothesis is tested using Table 14.
Table 4: Binary Logistic Regression Analysis Showing the Influence of Parents’ Residential Location on Acceptance of Childhood Immunization (n = 392).
|
Variable |
B |
SE |
Wald ꭓ2 |
df |
P |
OR |
95% CI |
|
Residential Location
|
|
|
78.373 |
2 |
<.001 |
|
|
|
Rural (Ref.) |
-1.705 |
.291 |
34.427 |
1 |
<.001 |
0.182 |
|
|
Semi-urban |
2.736 |
.343 |
63.712 |
1 |
<.001 |
15.427 |
7.879-30.203 |
|
Urban |
2.927 |
.352 |
69.276 |
1 |
<.001 |
18.667 |
9.370-37.186 |
Note: B = unstandardized regression coefficient, SE = standard error, Wald χ² = Wald Chi-Square statistic, df = degrees of freedom, p = p-value, OR = odds ratio, CI = confidence interval, Ref. = Reference category
Table 4 presents binary logistic regression analysis testing the null hypothesis that parents' residential location has no significant influence on the acceptance of childhood immunization in North-East Nigeria. The results showed that the model was statistically significant, Wald χ² (2, N = 392) = 78.373, p < .001, indicating that parents’ residential location significantly influenced acceptance of childhood immunization in North-East Nigeria.
Using rural residence as the reference category, results showed that parents residing in semi-urban areas had significantly higher odds of accepting childhood immunization (B = 2.736, SE = 0.343, Wald χ² = 63.712, p < .001, OR = 15.43, 95% CI [7.88-30.20]). This suggests that parents in semi-urban areas were 15.43 times more likely to accept childhood immunization compared to their rural counterparts.
Similarly, parents living in urban areas also had significantly increased odds of accepting childhood immunization (B = 2.927, SE = 0.352, Wald χ² = 69.276, p < .001, OR = 18.67, 95% CI [9.37-37.19]), indicating that urban parents were 18.67 times more likely to accept immunization for their children relative to those in rural areas. Based on these findings, the null hypothesis is not accepted. This implies that parents’ residential location has significant influence on acceptance of childhood immunization in North-East Nigeria.
Hypothesis Two: Parental level of knowledge of vaccine-preventable diseases has no significant influence on acceptance of childhood immunization in North -East, Nigeria. This hypothesis is tested using Table 5.
Table 5: Binary Logistic Regression Analysis Showing the Influence of Parental Level of Knowledge of Vaccine-preventable Diseases on Acceptance of Childhood Immunization (n = 392).
|
Variable |
B |
SE |
Wald ꭓ2 |
Df |
P |
OR |
95% CI |
|
Level of Knowledge
|
|
|
145.351 |
2 |
<.001 |
|
|
|
Poor (Ref.) |
-2.088 |
0.274 |
58.169 |
1 |
<.001 |
0.124 |
|
|
Fair |
3.597 |
0.358 |
101.041 |
1 |
<.001 |
36.475 |
18.090-73.547 |
|
Good |
4.946 |
0.475 |
108.244 |
1 |
<.001 |
140.590 |
55.375-356.943 |
Note: B = unstandardized regression coefficient, SE = standard error, Wald χ² = Wald Chi-Square statistic, df = degrees of freedom, p = p-value, OR = odds ratio, CI = confidence interval, Ref. = Reference category
Table 5 presents binary logistic regression analysis on influence of parental level of knowledge of vaccine-preventable diseases on acceptance of childhood immunization. The results showed that the overall model was statistically significant, Wald χ² (2, N = 392) = 145.35, p < .001, indicating that the level of knowledge of vaccine-preventable diseases significantly influenced the likelihood of childhood immunization acceptance in North-East Nigeria.
Using parents with poor knowledge as the reference group, those with fair knowledge were significantly more likely to accept childhood immunization, with an odds ratio (OR) of 36.475, 95% confidence interval (CI) [18.090-73.547], p < .001. This suggests that parents with fair knowledge were approximately 36 times more likely to accept immunization compared to those with poor knowledge. Similarly, parents with good knowledge of vaccine-preventable diseases were more likely to accept childhood immunization, with an OR of 140.590, 95% CI [55.375-356.943], p < .001. This indicates that parents with good knowledge of vaccine-preventable diseases were about 141 times more likely to accept childhood immunization compared to parents with poor knowledge. These findings provide strong evidence against the null hypothesis, supporting the conclusion that the level of knowledge of vaccine-preventable diseases significantly influences parental acceptance of childhood immunization in North-East Nigeria.
Discussion of Findings
This study investigated influence of parent’s location of residence and knowledge of vaccine-preventable diseases on acceptance of childhood immunization in North-East Nigeria. The study first of all, found that the proportion of parental acceptance of childhood immunization in North-East Nigeria stood at 52.8%. This finding suggests a moderate level of acceptance, indicating that just over half of the population surveyed were willing to immunize their children. While this may be seen as a positive step towards improving child health outcomes, it also implies that nearly half of the population still harbours doubts, fears, or opposition towards childhood immunization. In a region that is characterized by high child mortality rates and frequent outbreaks of vaccine-preventable diseases, such a proportion of acceptance of childhood immunization is worrisome. This proportion is nearly same with the 52% of parental acceptance of childhood immunization against influenza in Germany reported by [9]. However, it is important to consider the very different socio-economic and health system contexts of the two countries. Germany has a highly developed healthcare infrastructure, widespread access to health services, and a generally well-educated population. Despite this, moderate acceptance of immunization against seasonal influenza exists because it is often viewed by parents as a mild illness that does not warrant vaccination. In North-East Nigeria, on the other hand, the moderate acceptance of childhood immunization may be influenced more by structural and socio-cultural challenges. These may include poor access to immunization services, insecurity caused by insurgency, mistrust in government-led health programs, and misconceptions about the safety and purpose of vaccines.
This study also found disparity in the parental acceptance of childhood immunization based on residential location. The study found that parents who resided in urban areas were more receptive to childhood immunization, followed by those who resided in semi-urban areas, and the lowest in in rural areas. This trend was statistically confirmed through the test of hypothesis, which showed that parents living in urban areas had significantly higher odds of accepting childhood immunization compared to those in rural areas. Similarly, parents in semi-urban areas were also more likely to accept immunization than their rural counterparts. These findings are consistent with the results reported by Sibeudu et al, who investigated rural-urban differentials in the acceptance and utilization of routine childhood immunization in Anambra State, Nigeria. Their study also found that parents in urban areas were more likely to accept and utilize routine immunization services for their children than those in rural communities [10]. This finding could be attributed to a combination of structural, educational, and informational advantages commonly associated with urban locations. Urban residents typically have better access to healthcare facilities, more frequent exposure to health promotion messages through media and community outreach, and higher levels of education, all of which contribute to a more positive disposition towards childhood immunization and increased utilization of immunization services [10]. In contrast, parents in rural areas may face logistical barriers such as long distances to health centres, poor transportation, irregular vaccine availability, and limited health literacy, which could collectively discourage them from accepting immunization of their children [10].
Regarding the influence of parental knowledge of vaccine-preventable diseases on acceptance of childhood immunization in North-East Nigeria, the finding from this study indicates a strong positive relationship between parental knowledge of vaccine-preventable diseases and acceptance of childhood immunization. Parents who had good knowledge of such diseases demonstrated the highest rate of immunization acceptance (94.6%), while those with fair knowledge followed closely. In sharp contrast, parents with poor knowledge showed the least acceptance. Result from the corresponding hypothesis revealed that parents with good knowledge of vaccine-preventable diseases and those with fair knowledge were approximately 141 and 36 times, respectively, more likely to accept immunization compared to those with poor knowledge of vaccine-preventable diseases.
This finding aligns with that of Grandahl et al, who reported a significant association between parents’ knowledge of the Human Papillomavirus (HPV) and their willingness to vaccinate their female children. In both studies, knowledge served as a critical determinant of immunization acceptance. Parents with a clear understanding of Human papilloma virus vaccine (HPVV) and its potential to cause cervical cancer were more inclined to authorize vaccination for their daughters [11]. Similarly, in the North-East Nigeria study, has revealed that, knowledge of diseases such as measles, polio, or tuberculosis likely heightened parents’ sense of urgency and responsibility towards childhood immunization. These patterns emphasize that targeted health education and awareness campaigns can significantly improve vaccine uptake, especially in communities where misconceptions and misinformation remain prevalent. Ultimately, increasing parental knowledge can create a foundation for informed decision-making and promote broader public health compliance.
Conclusions
Based on the findings of this study, the following conclusions are made
5.4 Recommendations
Based on the conclusions, the following recommendations were made:














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org