International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Mesut Yavuz1, Alexandra Roth2 & Nicolai Savaskan3*
1YES Automation, Nürnberg, Germany.
2University Lübeck, Institute of Health Sciences, Department of Midwifery, Lübeck, Germany.
3Public Health Authority Neukölln, Berlin, Germany.
*Corresponding author: Nicolai Savaskan, Public Health Authority Neukölln, Berlin, Germany.
Received: February 10, 2026 | Accepted: February 28, 2026 | Published: March 09, 2026
Citation: Yavuz M, Roth A & Savaskan N., (2026) “Germany´s Public Health Service under Scrutiny: The Impact of Political Polarization on Health Authorities”. International Journal of Epidemiology and Public Health Research, 9(2); DOI: 10.61148/2836-2810/IJEPHR/190.
Copyright: © 2026. Nicolai Savaskan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Public health authorities have experienced significant political intervention in their enforcement work, particularly since the SARS-CoV-2 pandemic. This trend risks intensifying with increasing crisis situations and political polarization of the society and political parties in Germany. To ensure local public health authorities remain ethically resilient to crises under the principle of Germany’s historical heritage and reason-of-state “never again”, it is essential to foster an independent medical and scientific approach to gain medical expertise and resilience in crisis events. Public health experts in Germany’s public health service (PHS/ÖGD) should operate on people’s health free from political influences. Here, we highlight the challenges faced by public health authorities and propose solutions to create politically resilient structures for physicians and health experts in the public health service
Public health authority, health inequity, political partisanship, medical ethics, statutory health insurances, inpatients, outpatients, hospitals, Code of Geneva, political influence
Partisanship and professional orientation at local public health authorities
Constant successive disruptions including the corona pandemic, the ongoing war in Ukraine, Hamas' attack on Israel, and current political instability in countries such as Sudan, Yemen and Syria, have heightened societal polarization [1]. The public discourse in Germany is increasingly marked by polarizing terms such as ‘remigration,’ ‘irregular migration,’ identity politics’ including the social gender concepts, and ‘wokeness.’ Polarization has tangible effects: In a knife attack three people were killed and eight people stabbed during a German festival in Solingen. Such terroristic incidences as in Mannheim, Solingen, Magdeburg, Aschaffenburg Munich (all in Germany) and recently in Orem (USA) prompted an unforgiving debate surpassing stricter deportation policies for refugees, foreigners, and political opponents. Noteworthy, this discussion was mainly driven by parties known to be part the democratic core center. Germany’s public debate was marked with a new severity and reminds the announcement of mass deportation of undocumented migrants by the US president-elect [2]. Political shifts towards the far-right wings of Germany’s party spectrum also impact public health, as evidenced in Bautzen, a 38,000 people city in east Saxony. In fact, the district council of Bautzen abolished the office of the commissioner for foreigners arguing that such administration is not politically important anymore [3]. Germany faces such event for the first time in its recent federal history. The direction of such attack on public administration is clearly defined, however, the ultimate impact and outcome for society and public health remains uncertain.
Germanys Public Health Service heritage from the Nazi Era
Germany’s health system and in particular the public health authorities have a dark historical heritage. Physicians and other employees in public health offices played an active role during the deportation of Jewish, homosexuals, and disabled people. Shortly after the Nazis took over the lead, public health offices were aligned with the regime and transformed into a structure that largely persists today (Elsner, 2022). The ideology of so-called "racial hygiene" was subsequently implemented, particularly with the support of public health officers and other healthcare professionals. Before the National socialist’s era the ambulatory and stationary medical sector was self-governed by physicians (medical service providers) and statutory health insurances. This self-governed structure was reinstalled with the founding of the Federal Republic of Germany (Figure 1).
Figure 1: Germany’s health care system.
Germany’s health care system is based on three columns. A special feature of the public health service is its organization within the governmental institutions.
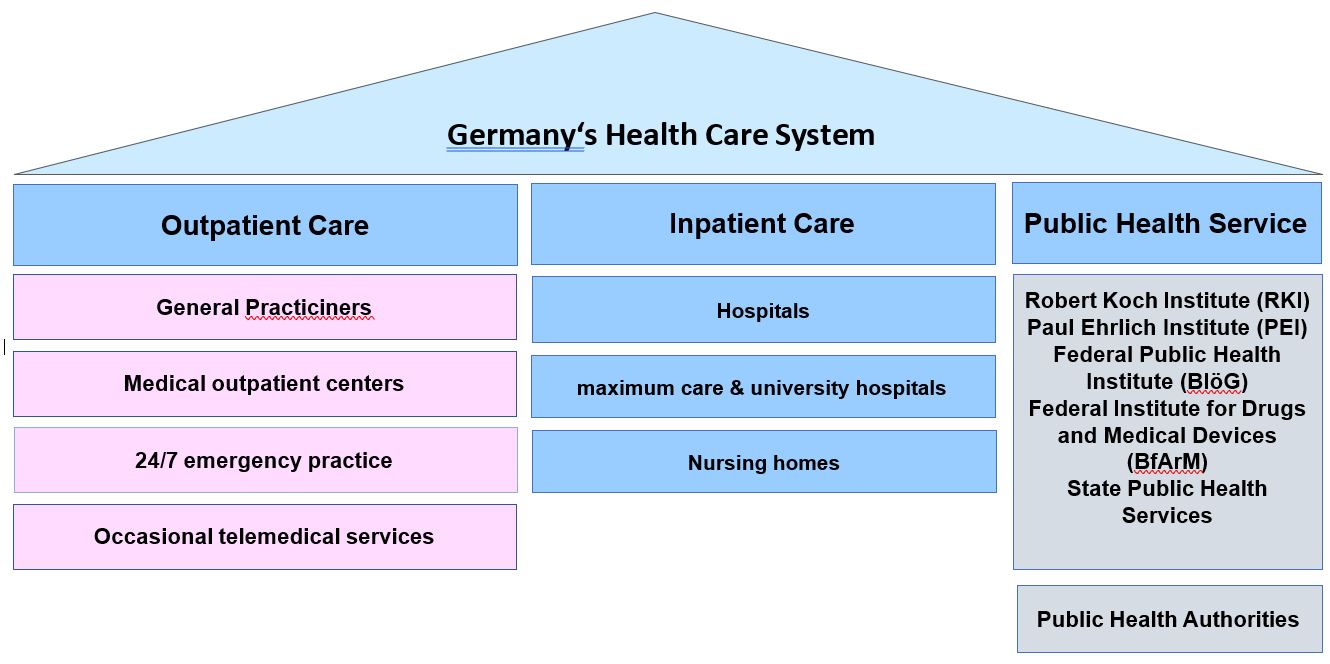
The health system focuses mainly on curative and individualized approaches for inpatients, outpatients, hospitals, rehabilitation centers, and nursing [3]. In fact, the German statutory health insurance system has a longer tradition in Germany and was first introduced in 1883 by the Chancellor Otto von Bismarck. Since then, German health system has been financed solitarily, i.e. all insured persons, irrespective of health risk, contribute the same percentage (about 8% as of today) of their income. In this pooled-risk system these contributions cover all benefits according to health needs as outpatients and inpatients. Outpatient and inpatient care are regarded as the two pillars of medical supply. Here, governmental influence is restricted to setting up the legal frames.
However, the German public health service as the third pillar of supply is completely located in governmental and public administration and is excluded from the medical self-governance [4].
The separation of powers between the executive government and health authorities is increasingly strained. Health authorities face a delicate balance between political loyalty and adherence to professional standards [5]. Their dual role—implementing political directives while making decisions based on medical expertise—creates operational conflicts. These conflicts could escalate when civil service obligations clash with the medical code of conduct (Code of Geneva), a fundamental guideline for medical practice worldwide [6].
Nearly half of all medical directors in health authorities were dismissed during the pandemic, according to one study [6]. At the federal level, scientific findings were often subordinated to political objectives without critical examination. Germany’s national public health agency, the Robert Koch Institute (RKI) itself admitted to ‘complying with political directives and wishes,’ undermining confidence in the scientific independence of official decisions [7]. This practice highlights the tension between administrative and political objectives. Such dynamics foster suspicion of an epistemology of the political process, wherein tailored expertise presents political directives as scientifically inviolable and politically ‘there is no alternative’ TINA rhetorics [8]. While this issue affects multiple administrative domains, the targeted instrumentalization of science in public health undermines democratic legitimacy and ethical principles. The resilience of health authorities is weakened, jeopardizing both the “never again” principle and fundamental ethical and professional values.
Health Authorities Between State Control and Medical Ethics
In Germany, medical officers bore significant responsibility for crimes during the National Socialist regime, particularly in dehumanized medicine [9]. Health authorities were instrumental in collecting hereditary-biological data, which facilitated forced sterilizations, deportations, and killings. These actions were not solely driven by individual motives or obedience but were embedded in a centralized public health structure that aligned health authorities with ideological objectives [9]. This organizational framework persists to some extent today. Current research continues to explore the role of health authorities during the Third Reich, leaving many questions unresolved [10].
The Geneva Declaration of the World Medical Association emerged as a response to the unforgivable atrocities of the Nazi era. This declaration, now integral to the German medical code of conduct, emphasizes the special responsibility of doctors to act as advocates for their patients and oppose discrimination in any form [4]. However, professional codes alone are insufficient to protect physicians in public health service from political pressures and specifications. Disciplinary mechanisms often act as subtle threats, fostering anticipatory conformity [4]. The Geneva Declaration was designed primarily for individual medical care and solely inadequately addresses the ethical challenges in public health. The LANCET commission on medicine during National Socialism and the Holocaust underscores the need for a specific code of ethics tailored to public health including all professions involved [10]. Such a code could define clear boundaries of ethical action and guide medical doctors and experts in public health service. While the Geneva Declaration provides a foundation, it does not fully resolve the ethical conflicts inherent in public health service.
Physicians Independence in Health Authorities
As of 2023, health authorities employed 26,320 individuals, including approximately 20% physicians and dentists. However, only 545 possessed a board certification in public health [11]. This shortage in specialized physician underscores structural challenges. Physicians in public health departments operate within public administration and are subject to political directives, unlike their counterparts in ambulance and clinical settings, who enjoy greater independence.
Traditionally, health authorities were managed by physicians due to their medical responsibilities. However, during the pandemic, this principle was frequently abandoned. Cities like Hanover, Düsseldorf, and Dresden removed or exchanged public medical officers. In addition, it is seemingly hard appointing physicians in public health service due to insufficient training, low recruitment, poor remuneration, and the unattractive image of public administration [11]. Instead of eliminating the causes, individual federal states have, as an emergency measure, put public health physicians under the direction of people who have no medical expertise whatsoever. In some cases, non-specialists replaced public medical officers and thereby undermining the professional integrity of public health authorities. What was overlooked was that health authorities are legally classified as medical institutions such as hospitals and are primarily active in population medicine. In addition, such emergency constructs collide with medical professional regulations. Such measures contravene the medical code of conduct, which mandates independence from non-physicians [5]. And this is for good reason: measures such as the imposition of quarantine, bar vaccinations, and forced accommodation when there is a risk to oneself or others are medical tasks [5]. However, the core issue extends beyond inadequate medical expertise. Germany’s public health authorities lack centralized structures for medical training and professional development. Approval, doctorate, habilitation, and specialist medical qualifications are literally foreign words in public administration. Furthermore, democratic trust in health authorities as non-partisan entities is eroding, compromising their effectiveness and credibility. This deficit became starkly evident during the pandemic. Strengthening the independence and professionalization of health authorities is critical in restoring public trust.
Health Authorities: Resilient and Future-Proof for the Challenges of the 21st Century The pandemic exposed structural weaknesses in Germany’s public health authorities. Although the acute crisis has subsided, political polarization and health inequalities persist. At the same time, health inequalities have worsened in Germany, with increased mortality and shorter life expectancies of more than eight years in disadvantaged groups compared to middle- and high-income groups [12, 13]. Despite having one of the world's most expensive healthcare systems, Germany's public health outcomes are indeed declining [13]. The current focus creates burdens on population health through inefficiencies. Prevention and health promotion should be significantly strengthened and the quality of care should be improved, especially for target groups under risk. This requires impulses from academic population medicine regarding existing over-, under- and incorrect care and various vulnerable population groups. Health authorities can act as a moderator, advocate and, if necessary, also through the provision of subsidiary services. Therefore, the sector boundary between individual medical care and public health should be opened and public health authorities should be linked in a triad with outpatient and inpatient care based on needs. However, this can only be implemented by creating the appropriate legal basis and allocating the resources required for this. Within public administration, improved population health care should be achieved through an independent branch of administration with medical responsibility at all hierarchical levels and with appropriate independence. A reorganization of health authorities into independent medical-scientific institutions is imperative. Historical models like the ‘Königsberg system’— developed by Hans Lohmeyer and Carl-Friedrich Goerdeler — offer valuable lessons and may lay the ground of a blue print. This system prioritized lean, needs-oriented structures, contrasting with the bureaucratic rigidity later imposed by the Nazi regime [9]. However, to consistently overcome the sector barriers and heterogeneity of health authorities (large city authorities vs. small health authorities in rural areas), a solution outside of public administration is required. Transforming health authorities into public corporations is feasible and aligns with precedents in the German healthcare system. Examples include university medical schools and the medical service of the health insurance companies, which gained independence through similar reforms. Public corporations enable efficient, independent operations while maintaining ethical integrity [3, 11]. Here, the established forms of institutions or corporations under public law offer a democratic alternative. In any case, the state's mandate to provide general health services, prevention, health promotion and the enforcement of health laws could be secured in such institution. In addition, such reform could resolve the conflict of instructions and restore the medical autonomy and self-administration provided for in the medical professional code. On the governmental site municipalities benefit as well: They would no longer have to rely solely on their public administration to fulfill their tasks, but would be able to access population-based health service from the public health corporation as a service on demand and needs-based. In this way, personnel and technical bottlenecks can be better solved and support and priorities in rural areas can be implemented as needed. Healthy living environments could be harmonized in Germany. In the current administrative corset, questions of responsibility often stand in the way of medical needs. In addition, special requirements for administrative assistance are required in public administration. It often fails due to political will or the party membership. However, viruses do not adhere to party colors and district boundaries, as we learned the hard way during the pandemic.
Is a change of public administration organization feasible? At least this is not something new in the German healthcare system. On one side, almost all medical service providers are organized into self-governed corporations. On the other hand, university medical schools were reformed into public self-governed corporations at the beginning of 2000 due to the recommendations of the federal science council [14]. In this way, university medical schools got rid of the organizational incompatibilities of public administration and became self- governed, independent, and internationally competitive. The most recent example is the medical service of the statutory health insurance companies (MD aka the former MDK). Formerly the medical service of the health insurance companies served solely in the interest of health insurances, whereas the MD was then legally transformed into a self-governed corporation under public law. Its independence from health insurance companies was strengthened and more independent assessments of care for citizens were ensured.
The organizational form of the corporation under public law as an indirect state administration allows, on the one hand, the fulfillment of sovereign tasks while maintaining ethical and medical behavior. On the other hand, this form of organization has self-administrative responsibility for finances and administration [14]. In addition to the government (at the state and local level), representatives of medical self-administration (state medical associations, university hospitals, association of statutory health insurance physicians and health insurance companies) are particularly suitable and permeable for democratic supervision. To secure the tasks from a budgetary perspective, representation from the state audit office as well as members of the civil society and patients should be included as a regulator.
Health as a Non-Partisan Responsibility
Promoting equitable health outcomes, irrespective of socioeconomic status, ethnicity, or political affiliation, is a pressing task for Germany. The current political polarization and the integration of health authorities into public administration compromise medical independence and public health (Figure 2).
Figure 2: Current determinants of health.
This graph displays an extended rainbow model of determinants of health inequities. In addition to general socio-economic, cultural and environmental conditions there are evidence to theorize and operationalize political polarization as an independent determinant of health inequities.
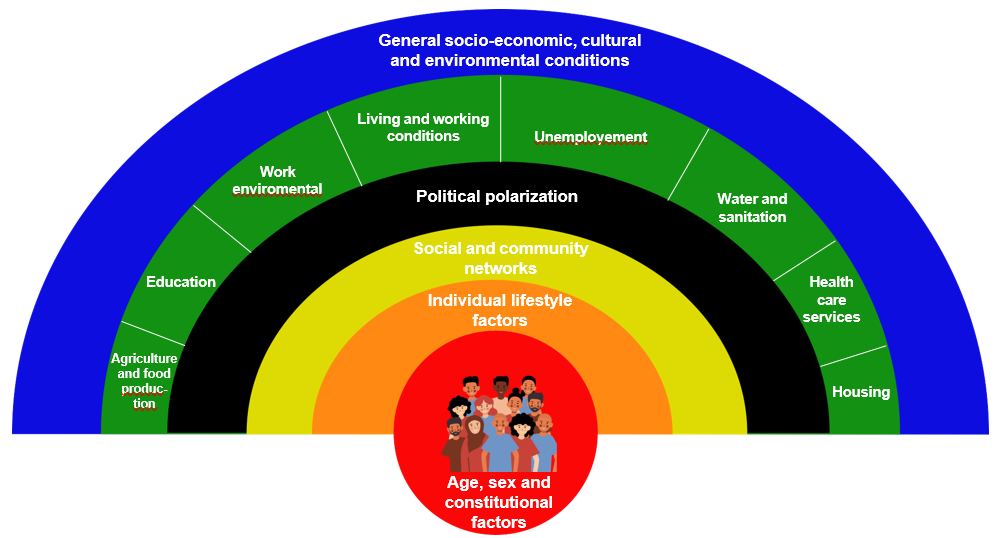
In fact, political polarization influences public health and undermines health equity [1]. Thus, health authorities need to be reorganized as independent medical institutions with a scientific approach to safeguard their neutrality and medical effectiveness. Ensuring a non-partisan structure is crucial to making health authorities resilient and future-proof, ready to meet the challenges of the 21st century. The course for a non- partisan, crisis-proof medical organization should be set before the next crisis.
Ethics statement
For this study an ethical approval was not required.
Acknowledgements
The authors thank the board of the German Society of Population Medicine & Public Health (DGöGB) for constructive discussions and remarks on the main concept of this paper.
Declaration of Interest statement
The authors declare that there is no conflict of interest.
Author contributions:
MY was part of the conceptualization of this study and wrote the original draft. AR developed the concept and wrote the original draft. NS administered the project, developed the concept, and wrote the original draft.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org