International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Olivia Michael Kimario1*, Miriam Jafary1Roger`s Machimu1
1Department of otorhinolaryngology Head and Neck, Catholic university of health and allied sciences p.0.box 1464 Tanzania.
*Correspondence Author: Olivia M Kimario, Department of otorhinolaryngology Head and Neck, Catholic university of health and allied sciences p.0.box 1464 Tanzania. ORCID ID: https://orcid.org/0009-0008-5499-7404.
Received: March 03, 2025
Accepted: March 07, 2025
Published: March 10, 2025
Citation: Olivia M Kimario. (2025) “Clinical Pattern, Comorbidities And Complications Of Allergic Rhinitis For Adolescence At Mwanza City”. International Journal of Epidemiology and Public Health Research, 6(1); DOI: 10.61148/2836- 2810/IJEPHR/110
Copyright: © 2025. Olivia M Kimario. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited., provided the original work is properly cited.
Allergic rhinitis is one of the commonest condition that occurs in our local environment. This condition has become more prominent as can attend more than 6patients in each clinic that attend at the OPD. The reasons can lie more on the climatically changes due to heavy industrialization and the new innovation that leads to disturb of the ecosystem. This study will help us to know the burden of the condition in adolescence and what will be the leading clinical presentation together with the associated complications.
This was community based descriptive cross-sectional study among students of selected secondary schools in Nyamagana district, Mwanza conducted from September 2024 to November, 2024.The findings will be analysed with SPSS version 21.
Participants involved in the study were 385.Male were 56% and female 44%.Male were more by 1.3:1.The age group that was involved more 13yrs to 16yrs by 78% followed by 17yrs to 19yrs which was 22%.Majority of the participants presented with symptoms of AR which was about 76%.Among the participants the leading symptoms were nasal congestion followed by Sneezing then reduce sense of smell,running nose,pharyngeal itching,cough,nasal mucosal itching,tearing,itching of the eyes then lastly is earfullness.The complications that encountered mostly was sleep disturbance.Other diseases that are accompany this condition the leading was asthma then conjunctivitis,eczema then sinusitis.
Allergic rhinitis is high among the participants aged from 13-19 years, with the leading symptoms been nasal congestion followed by sneezing this are commonly triggered by dust environment and cold weather. Asthma was the leading comorbities followed by allergic conjunctivitis.
Introduction
Allergic rhinitis (AR) is condition that results when IgE immunoglobulin mediate its repetitive reaction on the nasal mucosal leading to enlarged turbinate,mucosal edema which causes nasal blockage,sneezing rhinorrhoea, post-nasal drip and nasal itching.It also causes extra nasal symptoms such as itching of the eyes,ear,throat and palate, irritation of the conjunctival and erythema, snoring and sleep disturbance(1) . The WHO classifies allergic disease as the fourth most important chronic disease in the world. It is associated with significant morbidity and impact the quality of life of millions of individuals. Lost productivity at work or school and total healthcare expenditure exceeds several billion dollars annually in United States (1).
Allergic rhinitis is frequently ignored, under diagnosed, misdiagnosed, and mistreated, which not only is detrimental to health but also has social costs (2) with an estimation of >$6 billion spent on prescription medications alone (3). The total burden of allergic rhinitis lies on impaired physical and social functioning and also in a financial burden for treatment of its co-morbid diseases (4). The prevalence of allergic rhinitis differs among age groups. During childhood allergic rhinitis is found to be more numerous in boys but in adulthood is more frequent in women. (16-17). In the global synthesis of international studies of asthma and allergies in children reveals that the global average prevalence of AR in children aged 6-7 years was 8.5 % and13-14 years was 14.6% (14-15)
The prevalence of allergic rhinitis is estimated to range from 10% to 20% in the USA and Europe (17). A cross-sectional Study in Lebanon in 2009 with 3,115 students (13-14 yr.) selected from 13 schools in 5 Lebanese provinces to determine prevalence and characteristics of allergic rhinitis among Lebanese school children where by prevalence of allergic rhinitis was 45.2% (16).
In Africa a study which was done in South Africa for adolescents, from 1995 to 2002 has shown that there was increase prevalence of symptoms of Allergic rhinitis in a 12-month period from 30.4% in 1995 to 38.5% in 2002. This study was comparing the cross-sectional data from two international studies of Asthma and allergies (19).
In a follow-up study done in Kenya, there was a rise in prevalence of Allergic rhinitis in school children aged 13-14 yrs. from 14.9% in 1995 to 38.6% in 2001 (21).
Allergic rhinitis is one of the most common chronic diseases in childhood. Allergic disorders are encountered with a variable prevalence in different parts of the world. The prevalence of AR has increased in recent decades (15 In 2012 a study conducted in Tanzania, showed a prevalence of 14.7%, of which 92.6% manifested with co-morbidities that included adenoid hypertrophy, hypertrophy of inferior turbinate, nasal polyps, otitis media and sinusitis. Sleep disturbance was noted to be common in children with adenoids hypertrophy (11-13).
AR symptoms should be a red flag for a potentially serious lifelong effect, as the younger the child, the greater the likelihood of suffering severe and persistent disease and its related co- morbidities later in life (5). The negative effect of early symptoms should not be downplayed. Allergic Rhinitis is one of the most common as well synonyms of hay fever, which commonly arise as a response to allergens such as pollen, dust, animal dander (old skin) and mold. Classic symptoms of Allergic Rhinitis manifests as nasal congestion, nasal itch, rhinorrhea (runny nose), sneezing, and itchy eyes (5).
Allergic Rhinitis (AR) has major co-morbidities which are asthma, nasal polyps (NP), adenoid hypertrophy, tonsillitis, hypertrophied turbinate, conjunctivitis, rhino sinusitis (RS), otitis media with effusion (OME) and sleep apnea (6–9,11,25). Patients suffer from insomnia ,snoring, and obstructive sleep apnea syndrome which result in daytime somnolence, fatigue, irritability, depression, reduced productivity and memory and learning deficit. There is a strong correlation between severity of rhinitis symptoms, particularly nasal obstruction, and sleep impairment. So treatment of AR results in better sleep, reduced daytime somnolence, and improved quality of life. (10).]. Socially unacceptable behavior such as sniffing, sneezing, noisy breathing and coughing may lead to isolation and rejection at school and home. Further morbidity results from associated conditions such as sinusitis, adenoids, tonsil hypertrophy and otitis media [11].
There are limited studies done in Tanzania to determine the magnitude and pattern Allergic rhinitis among adolescents. So, this study aims to determine prevalence, comorbidities and complications of allergic rhinitis among adolescents.
Study area
Study was conducted among selected secondary schools in Nyamagana District, Mwanza region, Tanzania, where by using simple random sampling 2 secondary schools were selected among all secondary schools which are Mwanza secondary and Nyakabungo secondary school to participate in the study.
Study design
This was community based descriptive cross-sectional study among students of selected secondary schools in Nyamagana district, Mwanza conducted from September, 2024 to November, 2024.
Study population
The study population included students from the selected secondary schools in Nyamagana district aged 13-19 years old during the period of study.
Inclusion criteria
All secondary school students aged between 13-19 years old (adolescents’ group)
Exclusion criteria
Students that who have history of nasal or sinus surgery.
Students who are on medications that affecting nasal symptoms.
Sampling procedure
The study population was including secondary school students aged between 13 to 19 years of age in the selected secondary school, Using simple random sampling 2 secondary schools were selected from a list of 7 secondary schools obtained from Nyamagana education officer in Mwanza.At selected schools the present students who meet criteria were randomly selected from the first stage using simple random technique and consent and assent forms will be asked from students.
Data collection procedure
At selected secondary school, the primary researcher and research assistants introduced themselves and explain clearly the aim and purpose of the study that was conducted.
Consent forms were distributed to class teachers and teachers on duty of the selected schools and then collected.
Data were collected using self-structured questionnaires through interviewing the students. The questionnaire consist of four parties; Demographic information, triggered factors and symptoms, comorbidities and complications of Allergic rhinitis.
All student that consent, were interviewed using a structure questioner/clinical examination form.
The interview was conducted by either primary researcher or trained research assistants. Carefully history taking, physical examination were performed to the student.
Data analysis
Data were analyzed using SPSS version 21.
Results
Sociodemographic Characteristics
In this study, a total of 385 students were recruited from selected secondary schools in Nyamagana district, Mwanza. Majority were males (56%, n=216) than females (44%, n=169), giving a female to male ratio of 1.3:1. Based on ages about 78% of all participants aged 13-16years old while the rest about 22% aged between 17-19 years old. On level of education, both were taking ordinary level education as 126(33%) Were form one student, 85(22%) were form two students, 75(19%) were form 3 students and 99(26%) were form four students. (Table 1).
Table 1: social demographic information’s.
|
|
Variable |
Frequency (n) |
Percentage (%) |
|
Sex |
Male |
216 |
56 |
|
|
Female |
169 |
44 |
|
Age |
13-16 |
299 |
78 |
|
|
17-19 |
86 |
22 |
|
Class |
Form 1 |
126 |
33 |
|
|
Form 2 |
85 |
22 |
|
|
Form 3 |
75 |
19 |
|
|
Form 4 |
99 |
26 |
Among all 385 participants the analysed symptoms of allergic rhinitis were answered by all participants and among them, 293 (76%) reported to experience symptoms of rhinitis while 92 (24%) denied symptoms of rhinitis where by majority 229(59%) were in the age group 13-16 years old and the remaining 64 (17%) were in the age group 17-19 years.
Among 293 participants with AR, male were 164 (43%) as compared to female 129(34%). In case of symptom, nasal congestion and sneezing were the most common symptoms reported by majority of students 89% and 87% respectively. (Table2).
Table 2: Distribution of clinical symptoms of AR.
|
Symptom |
Developed (%) |
Not developed (%) |
|
Nasal Congestion |
89 |
11 |
|
Nose itching |
44 |
56 |
|
Sneezing |
87 |
13 |
|
Runny nose |
68 |
32 |
|
Itching eyes |
29 |
71 |
|
Tearing eyes |
39 |
61 |
|
Reduced sense of smell |
79 |
21 |
|
Ear fullness |
27 |
73 |
|
Pharyngeal itching |
60 |
40 |
|
Cough |
48 |
52 |
Triggers.
As the rhinitis has different symptom triggers which differ from one individual to another. About 88% of all participants with rhinitis had the recurrent history of developing rhinitis symptoms when exposed to dust, while 13% of all participants with rhinitis when exposed to animal products, 22% when exposed to smoke, 53% when exposed to cold weather, 22% when exposed to strong odour and 12% when exposed to the pollen grains.
Comorbidities.
It has observed that 36% of all participants with rhinitis had asthma, 9% has eczema, 7% of all has chronic sinusitis, and 18% has conjunctivitis. (Figure 1).
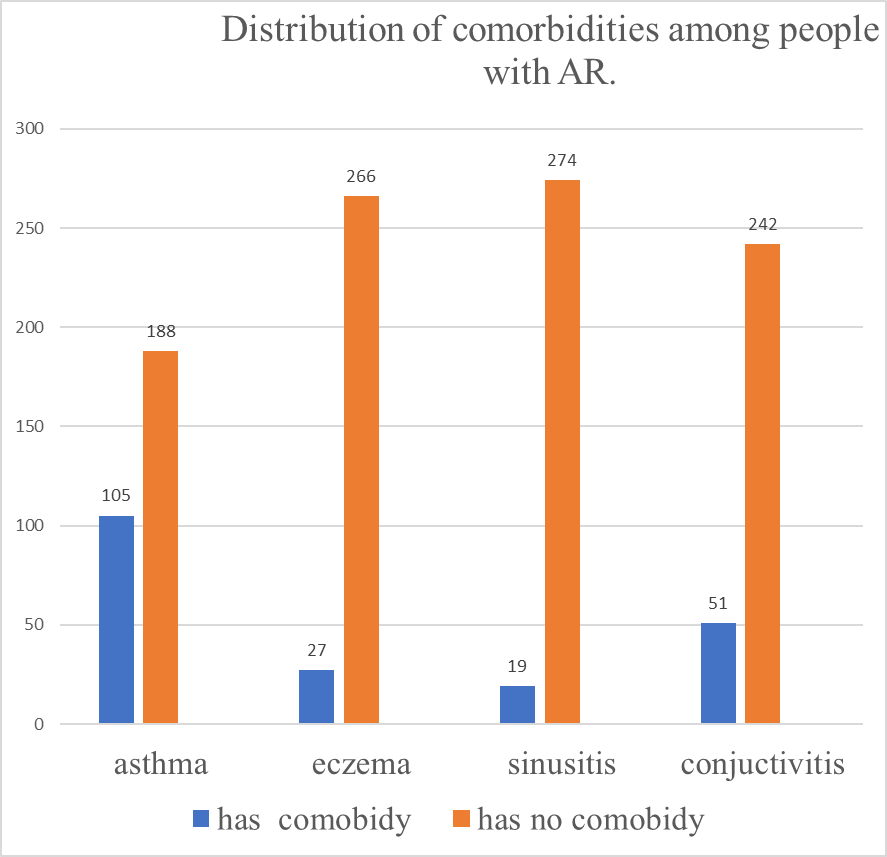
Figure 1: showing distribution of comorbidities among participants with AR.
Complications.
During attack 86% of all participants reported the sleep disturbance, 41% reported poor school performance and 81% reported reduced smell sensation while only 17% reported ear fullness. (Figure 2).
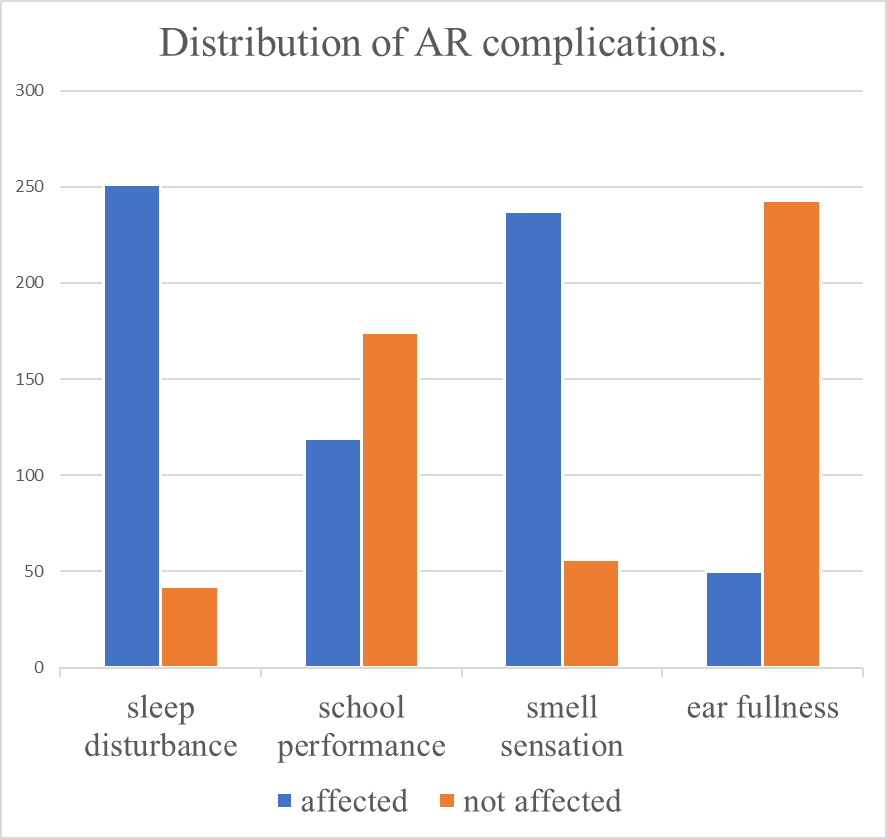
Figure 2: showing distribution of AR complications
Discussion
In this study, we found that the presentation of the allergic rhinitis was 293 (76%) on clinical symptoms reported by participants while 92 (24%) denied symptoms of rhinitis. The findings of this study are higher compared to the study done in south Africa and Kenya which involved children aged 13-14 years old [19,20]. In the study done in South Africa prevalence of Allergic rhinitis was noted to increase from 30.4% to 38.5% over a period of seven years [19]. Whereas in Kenya study the prevalence was 38.6%. [20].
Also the study done in Tanzania at Bugando Mwanza had a lower prevalence of allergic rhinitis which was 14.7% [24] and the one done in Muhimbili national hospital which was 10.3% [25]. In comparison to the study these two studies where hospital based studies while this study is the community based study.This shows the presentation of allergic rhinitis is high in our community and we a missing certain number of people that seek medical treatment.
The higher prevalence’s of the study could be attributed by various factors such as climatic changes, dietary change and environmental changes, factors like dust which has been reported by 87.6% of the participant and cold weather (53%) also urban area which is highly polluted by vehicle pollution and industrialization which all can attribute to higher prevalence of allergic rhinitis as supported by the studies [7, 19] which showed that the more urbanized the area the higher the prevalence of allergic rhinitis.
Regarding prevalence of allergic rhinitis by age, this study shows that the more affected participants were in the age group 13-16 years by the prevalence of 59% and prevalence of 17% in age group 17-19yrs.in comparison to other studies, this study is align with other studies such as the study done in BMC, Mwanza Tanzania which showed overall prevalence of AR to be 14.7% among which 69% of participants were aged below 20 years [24]. The reason for this can be due to increased exposure to allergen, irritant when they play around and execercibate to allergic rhinitis.
Regarding male to female in this study it has observed that 43% of male has allergic rhinitis while 34% female has allergic rhinitis led to 1.3:1 this is almost the same to the study done at bugando medical Centre among the patients attended ENT clinic, the results came out with the male to female prevalence ratio of allergic rhinitis to be 1:1 [24], also other study done at MNH found that male to female ratio of AR is 1:1 [25].The findings of the study are almost the same there is no sexual predominance.
In this study, it has been observed that 36% of all participants with rhinitis had asthma , 18% has allergic conjunctivitis. In comparison to the other studies the higher prevalence of asthma in this study is aligning to the findings in the study done at Bugando medical centgre Mwanza Tanzania [24] though the study reveal other comorbidity like Adenoid hypertrophy, tonsillitis, hypertrophy of inferior turbinate, nasal polyps, otitis media and sinusitis were the most common co-morbidities affecting 92.6% of cases and were the major reason for attending hospital services. Also the high prevalence for conjunctivitis (18%) as a common co-occurrence due to shared inflammatory pathway as reported to the stud done in Lebanon [18] and Kenya [20] and compared to the study done in BMC allergic conjunctivitis was found to be 51.9% [24], thus more studies have to be done in community for comparison rather than compare the sick one to the healthy.
The leading complication was found to be sleep disturbance by (86%), this was contributed by presentation of nasal congestion, sneezing, rhinorrhea and pruritus. Allergic rhinitis affect sleep as reported by our participants. This is almost similar to the study done in Bugando mwanza were 74.2% reported sleep disturbance [24] and similar to the one done in south Africa which reported 76.6% had sleep disturbances [27].This is led to impairment in the quality of life leading to fatigue, daytime sleepiness memory deficit and poor concentration as a result of indirect impact in academic performance of students. [26]. All these shows the chronic burden of allergic rhinitis and its comorbidities.
Study Limitation.
The study was based on self-reported data for the symptoms and questionnaire responses which may led to underreporting or over reporting of symptoms also lack of clinical confirmation e.g. Skin-prick test led to misclassification of symptoms.
Seasonal variations and environmental factors as the study could not assess detailed environmental exposure which could provide more insight to the triggers of allergic rhinitis.
The study has limited generalizability as the findings are specific from 2 schools and only for adolescents while exclude younger children, this may not be representative of broader Tanzania children populations was excluded.
Conclusion.
Allergic rhinitis is high among the participants aged from 13-19 years, with the leading symptoms been nasal congestion followed by sneezing this are commonly triggered by dust environment and cold weather. Asthma was the leading comorbities followed by allergic conjunctivitis. The leading complication was sleep disturbance which significantly impact the quality of life in this population. Therefore, there is need for target intervention to reduce the burden.
Recommendations.
More study need to be conducted to the community to determine the prevalence of allergic rhinitis in our setting by assess both clinical features, physical examinations and diagnostic tools in order to elevate the prevalence of this disease.
Early detection and treatment of Allergic rhinitis in children and avoidance of triggering factors as the first line of management.
Improve access to health care services including ENT clinics to ensure timely diagnosis and treatment of allergic rhinitis and its comorbidities.
The government should advocate national policies to address allergic rhinitis in schools and community in general.
Declaration
I Olivia M Kimario declare that this is my work it has not been presented or copied anywhere as of the other journal. The study protocol was approved by the Ethics committee of the joint CUHAS/BUGANDO committee.
Ethical approval
This was soughed from the Joint BMC/CUHAS Research Ethical Committee and Director of research and innovation CUHAS. Consent was obtained from the study respondents after providing them with enough information about the benefit of the study. Written informed consent from participants was soughed before recruitment into the study. For those less than 18 years old, informed consent was obtained from their class teachers/ teachers on duty. Potential study participants were informed of the study objectives and of their right to participate, to withdraw from it whenever they wish to, or not to participate at all.
Funding: Not applicable
Acknowledgment:Would like to appreciate the work of surgical OPD staff and my colleagues surgeons for seeing this off and tireless making the possible contribution making this possible.
Competing interests: No authors declare competing interests
Authors` Contributions
OMK-drafting the manuscript, review of literature and discussions.
MJ-Literature search, discussion of the data.
RM-General overview of the manuscript and discussion.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org