International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Mushtary Mimi1,2, Rubina Oad3, G.U. Ahsan7, Shafi Bhuiyan4,5,6*
1North South University, Dhaka Bangladesh.
2Mcmaster University, Ontario, Canada.
3Western University of Ontario, Canada.
4University of Memphis, TN, USA.
5University of Toronto, Canada.
6Bangladesh University of Health Sciences.
7Canadian University of Bangladesh.
*Corresponding author: Shafi Bhuiyan, School of Public Health, University of Memphis, TN, USA.
Received: December 25, 2024
Accepted: December 30, 2024
Published: January 01, 2025
Citation: Mimi M, Rubina Oad, G.U. Ahsan, Bhuiyan S. (2025) “Assessment of Knowledge On The Maternal & Child Health Handbook (Mch) Contents Among Pregnant Women In Selected Health Facilities At Northern Districts, Bangladesh”. International Journal of Epidemiology and Public Health Research, 6(1); DOI: 10.61148/2836-2810/IJEPHR/102
Copyright: © 2025. Olivia M Kimario. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Despite provision of many health services by public healthcare facilities including availability of qualified healthcare professionals, and free diagnostic and treatment services, the Maternal & Infant Mortality Rates (MMR & IMR) in Northern Bangladesh remain high. An important reason for the enduring high rates is lack of health literacy among pregnant women and their families.
Existing hospital-based health-record tools in Northern Bangladesh do not contain sufficient information and thus have not been very helpful in reducing the MMR & IMR so far. Significant information can be provided to the pregnant women, their families & the healthcare professionals by using the Maternal & Child Health (MCH) Handbook. The Handbook documents personalized home & facility-based health records of the mother and the child, including information pertaining to pregnancy, delivery, postnatal period, immunizations & growth monitoring etc. This information enhances healthcare workers' ability to provide appropriate patient care, by referencing their well-documented records. Furthermore, the Handbook equips patients and health professionals with detailed medical histories, rendering both parties better suited to respond to emergency situations. This will significantly improve the healthcare of the mother & the child, which would ultimately lead to decreased MMR & IMR.
Developing such a handbook requires assessment of the prior level of health literacy of women and their families, in terms of maternal & child-health. A handbook was then developed based on the knowledge assessment results. For example, the data revealed that the people lacked information on when and what vaccine their child needed, and thus vaccination schedules were included in the MCH Handbook. Healthcare workers, community leaders and other stakeholders were involved during the entire process. The MCH Handbook was thus developed to increase awareness related to maternal and childcare that would contribute to better health outcomes leading to a decrease in Maternal & Infant Mortality Rates (MMR & IMR).
Introduction
The Sustainable Development Goals (SDGs), targets reducing maternal mortality, newborn mortality and under-five mortality to 12, 25 and fewer than 70 per 100,000 live births respectively by 2030. The Sample Vital Registration System (SVRS) Report 2019 shows that the Maternal Death Rate (MDR) of Bangladesh is 165 per 100,000 live births and that more than 50% of infants are born with the help of birth attendants lacking any formal training. In developing countries like Bangladesh, increased MMR & IMR prevails, especially in underprivileged communities, due to many factors including, low socioeconomic status, illiteracy, early motherhood, cultural attitudes, inadequate access to healthcare and untrained birth attendants. [21]
The Maternal & Child Health (MCH) Handbook is a comprehensive home-based health-record that contains significant information including specific health-records related to pregnancy, delivery, neonatal period, & infancy, and records of doctor’s visits. It enables the women and healthcare professionals to make better and informed decisions regarding patient care. It may also assist patient’s family members, including their spouses, in case they wish to become engaged in maternal and childcare.[11]
The Handbook may be tailored to the patient, based on factors like culture, socioeconomic status, and education level etc. For example, Graphics were added to a MCH Handbook in Cambodia to make it useful for illiterate women. More than 50 nations including Kenya, Palestine, Thailand, Indonesia, the Netherlands, Dominica, Lao, Afghanistan, & Vietnam, have been using MCH Handbooks. In Kenya, the MCH Handbook was implemented where pediatric and obstetric data was merged to facilitate HIV screening. HIV diagnostic services were included in the handbook.
According to Dr. Shafi Ullah Bhuiyan, Associate Professor of Clinical Public Health at University of Toronto’s Dalla Lana School of Public Health, the MCH Handbook significantly improved the knowledge of mothers and thus the utilization of MCH services like breastfeeding & child immunizations etc., since introduction of MCH Handbook in Japan in 1966. These results were based on the outcomes of the first pilot MCH Handbook project in 2002, at Gazipur, Bangladesh. [5]
Another research study found that the MCH Handbook helped women understand prenatal care, pregnancy risk factors, labor and delivery symptoms, breastfeeding, and vaccine coverage. The pregnant women who followed the handbook improved their maternity and child health (MCH) practices and used more MCH services because of their enhanced awareness. (3)
The MCH Handbook was introduced in Bangladesh in 2002 by Dr.Shafi Bhuiyan. In 2006, he conducted research with support of the Obstetrical & Gynecological Society of Bangladesh (OGSB) & Japan International Cooperation Agency (JICA) to find the impact of the Handbook on MCH services. From 2007-2009, JSPS GrantAid Research provided support for the project. Many Organizations are now using the MCH Manual. However, its use in Northern Bangladesh is yet to be evaluated. This study aims to assess the existing knowledge of the pregnant women of the northern Bangladesh regarding maternal and infant care. This information will be used to produce an MCH Handbook relevant to their context.
Methodology
Objectives :
General: Assess the knowledge of pregnant women on maternal & child health.
Specific: To assess knowledge related to:
i) ANC & PNC services
ii) Vaccine & its impact on utilization of service facilities
iii) Nutrition services are important during ANC & PNC
iv) Breastfeeding & its effect on quality MCH services.
And to improve:
v) Culturally appropriate MCH Handbook contents.
Study Design
This is a cross-sectional hospital-based study.
Target Population:
192 pregnant women in their first trimester and on their first visit at selected local community-clinics and NGO hospitals in Rangpur and Joypurhat District, Bangladesh.
Study site & Area:
North Bengal Region of Bangladesh
Study Period:
January 2023- February 2023
Sample Size(n):
n=96 as per the Sample Size Formula.
For more accuracy, double the number of participants were included, which makes n=192
Inclusion criteria:
Exclusion Criteria:
Sampling technique:
Convenience sampling technique was used to collect data.
Data collection tools:
Bangla Questionnaire previously used to develop the MCH Handbook for Bangladesh by Dr. Shafi Ullah Bhuiyan prepared in 2002-2007 (at Osaka University, Japan), was modified to collect data.
Data Management & Analysis Plan:
Data was collected by trained data collectors and the whole data collection process, from beginning till end, was supervised by the researchers. All the interviewers at 3 facilities were trained (including role planning and trial) prior to data collection.
Quantitative data was analyzed by using SPSS 28.
Quality Control & Quality Assurance:
To ensure quality control and assurance, regular help and guidance was taken from the project’s supervisor. The Questionnaire was designed using simple language in Bangla and it was pre-tested before collecting data from the field to assess its effectiveness. To maintain quality, data was collected by the researcher and a team of highly trained healthcare providers/volunteers. The patients were contacted and interviewed over the phone by one of the trained healthcare providers. Details related to the study were provided. If they were not willing to answer, the data was not collected. Data was cross-checked for reliability.
Ethical Consideration:
The study protocol was approved by the authorities of North South University,Bangldesh.
Detailed consent was taken from the participants. They were not forced to respond to the questionnaire. All information was kept confidential.
Limitations of the study:
Outcome of this study cannot be generalized for nationwide decision support. The study was limited to two community clinics and one NGO based local hospital in Northern Bangladesh.
Results:
Respondent Mother’s age: (Table 1, Figure 1)
43.75% were aged less than 20 years, 42.18% were aged between 20-24 years, 11.97% were between 25-29 years and only 2.08% were older than 30 years.
|
Mothers Age |
n=192 |
Percentage (%) |
|
<20 Years |
84 |
43.75% |
|
20-24 Years |
81 |
42.18% |
|
25-29 Years |
23 |
11.97% |
|
≥30 Years |
4 |
2.08% |
Table 1: Age of the mothers
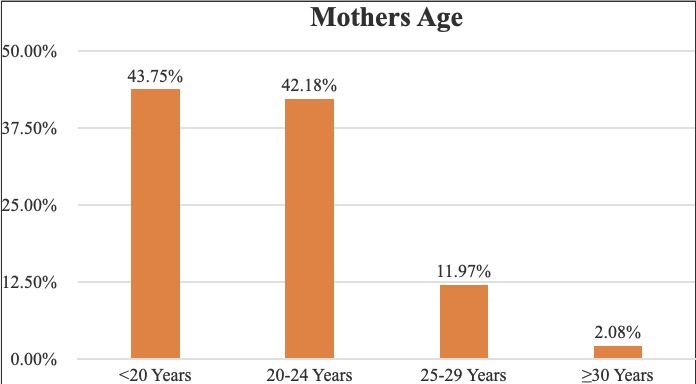
Figure 1: Age of the mothers
Mother’s Education: (Table 2, Figure 2)
41.70% of the mothers had secondary school education, 25.80% received College education, and 22.40% received university education. 8.85% of the mothers attended primary school and 2.08% had no formal education at all.
|
Education |
n=192 |
Percentage (%) |
|
Primary school (1-5) |
17 |
8.85% |
|
Secondary school (6-10) |
80 |
41.70% |
|
College (11-12) |
46 |
25.80% |
|
University (>12 grade) |
43 |
22.40% |
|
No formal education |
4 |
2.08% |
Table 2: Mother’s Education
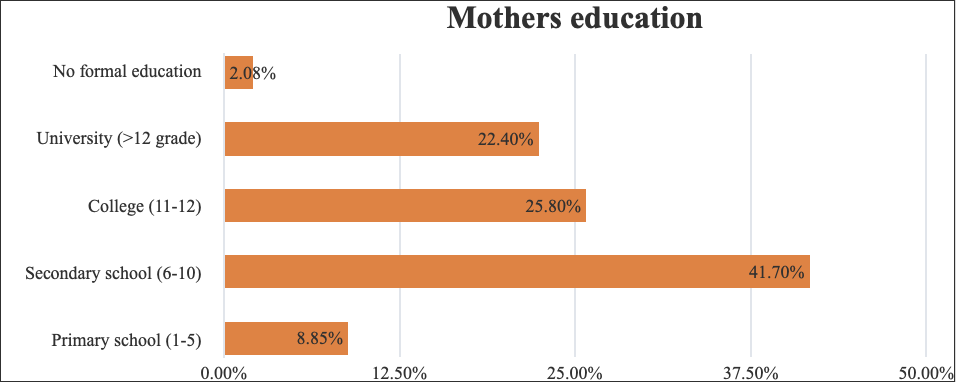
Figure 2: Mother’s education
Father’s Education: (Table 3, Figure 3)
33.86% received secondary education. 29.69% received university, 22.92% college and 10.93% primary education. 2.60% had no formal education at all.
|
Education |
n=192 |
Percentage (%) |
|
Primary school (1-5) |
21 |
10.93% |
|
Secondary school (6-10) |
65 |
33.86% |
|
College (11-12) |
44 |
22.92% |
|
University (>12 grade) |
57 |
29.69% |
|
No formal education |
5 |
2.60% |
Table 2: Education of the Fathers
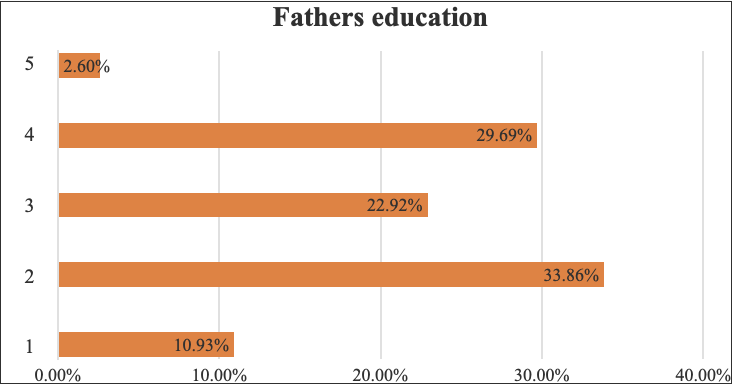
Figure 3: Father’s education
Mother’s Occupation: (Table 4, Figure 4)
93.22% are housewives. Private jobs 3.64%. Govt.jobs, business & student 1.04% each.
|
Occupation |
n=192 |
Percentage (%) |
|
Housewife |
179 |
93.22% |
|
Private jobs |
7 |
3.64% |
|
Govt. jobs |
2 |
1.04% |
|
Businessman |
2 |
1.04% |
|
Student |
2 |
1.04% |
Table 4: Mother’s Occupation
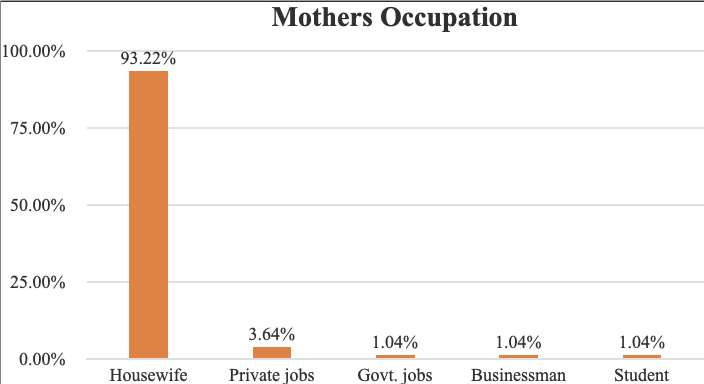
Figure 4: Mother’s Occupation
Family Income: (Table 5, Figure 5)
30.20% earn between 10,000-14499 BDT, 29.16% earn more than 15,000 BDT. 26.04% earn between 5000-999 BDT. 14.58% range 2000-4999.
|
Family income |
n=192 |
Percentage (%) |
|
2000-4999 |
28 |
14.58% |
|
5000-9999 |
50 |
26.04% |
|
10000-14499 |
58 |
30.20% |
|
>15000 |
56 |
29.16% |
Table 5: Family Income
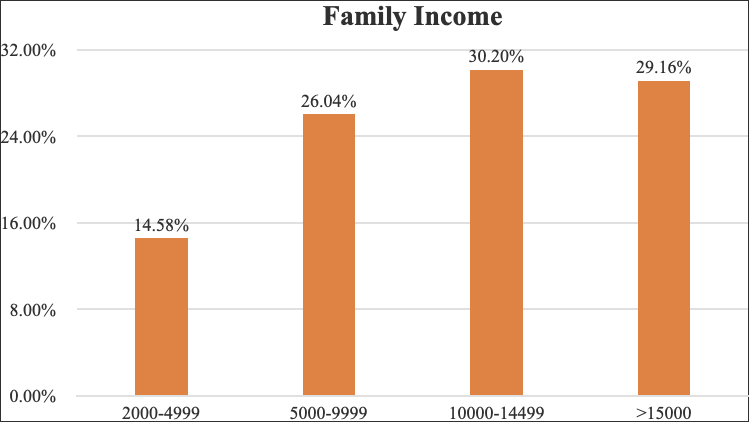
Figure 5: Family Income
Accompanying Person:(Table 6, Figure 6)
35.93% were accompanied by husbands, 13.54% by mothers-in-law, 6.77% by sisters, 2.60% by brothers and 3.64% by others. 6.67% alone, and 0.52% with friends.
|
Accompanying person |
n=192 |
Percentage (%) |
|
Husband |
69 |
35.93% |
|
Mother-in-law |
26 |
13.54% |
|
Girlfriend |
1 |
0.52% |
|
Brother |
5 |
2.60% |
|
Sister |
13 |
6.77% |
|
Single |
13 |
6.77% |
|
Other |
7 |
3.64% |
Table 6: Accompanying Person
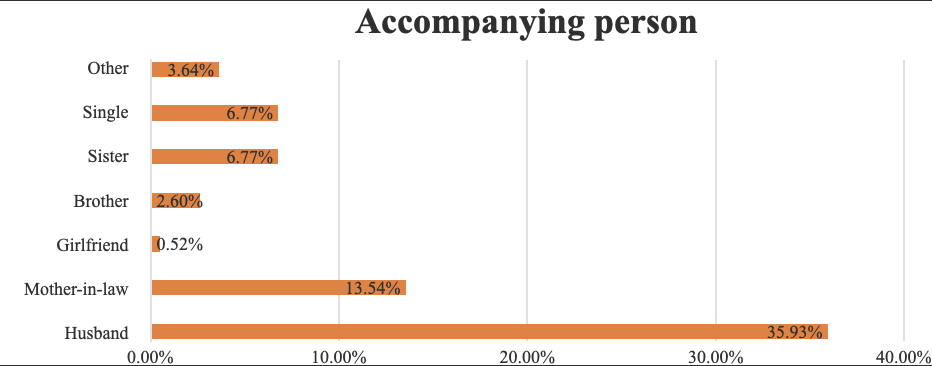
Figure 6: Accompanying Person
Transportation Used: (Tabe 7, Figure 7)
35.93% came walking, 13.54% used rickshaw, 2.60% used local vehicle Tempu, 0.52% used Van and 6.77% used other modes.
|
Transport used |
n=192 |
Percentage (%) |
|
Walk |
69 |
35.93% |
|
Rickshaw |
26 |
13.54% |
|
Van |
1 |
0.52% |
|
Tempu |
5 |
2.60% |
|
Others |
13 |
6.77% |
Table 7: Transport used to visit the clinic
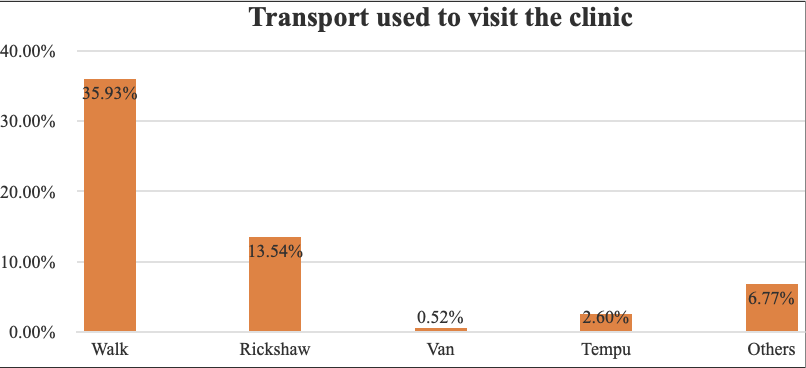
Figure 7: Transport used to visit the clinic
Reasons for Clinic Visit: (Table 8, Figure 8)
|
Reasons for Clinic Visit |
n=192 |
Percentage (%) |
|
ANC |
191 |
99.47% |
|
PNC |
1 |
0.52% |
Table 8: Reasons for Clinic Visit
Mother’s Knowledge: (Table 9)
Of 192 pregnant mothers, only 34.37% (66) mothers had the necessary knowledge about maintaining a healthy pregnancy. 57.81% had knowledge about Antenatal Health Care. 45.31% women knew about nutrition requirements during pregnancy. 21.35% of them were aware of the TT vaccine. Only 10.93% had knowledge about pregnancy related dangers and warning signs. 4.16% of participants were informed about postpartum risk signs. 3.64%, 3.12% & 3.12% of the mothers possessed knowledge about postpartum care, birth planning and postpartum birth control respectively.
|
Mothers' knowledge |
n=192 |
Percentage (%) |
|
TT vaccine |
41 |
21.35% |
|
Antenatal health care |
111 |
57.81% |
|
Nutrition during pregnancy |
87 |
45.31% |
|
Pregnancy signs and warning information |
21 |
10.93% |
|
Birth planning |
6 |
3.12% |
|
Postpartum risk signs |
8 |
4.16% |
|
Postpartum care |
7 |
3.64% |
|
Postpartum birth control |
6 |
3.12% |
|
All |
66 |
34.37% |
Table 9: Knowledge of the mothers
Discussion
Bangladesh is a densely populated country with high Maternal and Infant Mortality Rates. Women, in particular, do not receive appropriate gender-sensitive services from health facilities. They are not given sufficient information related to their health which could enable them to make informed decisions about their health.
Prenatal and postnatal cards, vaccination cards, and other such cards are the typical forms of health communication in Bangladesh. Despite the possibility that such a tool could lower the rate of maternal mortality, there is no evidence that mothers in Bangladesh are persuaded of the benefits of the cards, and no research-based validated tool has yet been established in Bangladesh to meet clients' needs for MCH health information and health and healthcare records. [5] MCH handbooks are comprehensive, health-promoting at-home pamphlets that frequently give clients information on emergency care, family planning, immunization, neonatal and childcare, emergency care related to pregnancy (including schedules), labor and delivery, postnatal care, and records for both clients and medical professionals. They promote high-quality care and risk-free parenting by fostering communication among doctors, expecting women, and their families, and by disseminating health-related information. [1] It promotes their involvement in decision-making and management of their family's health. [2]
According to a study conducted in Vietnam, the MCH Handbook helped expecting mothers comprehend and practice exclusive breastfeeding and increase their attendance at prenatal care sessions from one to three. The study supported the role of the MCH Handbook as a catalyst for continuity in maternal, neonatal, and pediatric care. [20] Another research study found that women who used alternative health cards were more knowledgeable about MCH concerns, better at taking care of their MCHs, and more likely to utilize MCH services. [1] Women in Palestine who couldn't read the manual for themselves got support from their medical personnel who had access to the information it contained, according to Hagiwaraa et al (2013). The involvement of their healthcare professionals demonstrates its efficacy and the benefits it offers to women with various educational backgrounds. [3] After their education about the typical symptoms and hazards associated with pregnancy and delivery, women reported feeling more at ease and confident. Their confidence enabled them to discuss their situation with medical specialists and get better care for both themselves and their children. According to the study, many women felt that the health education suggestions in the MCH handbook had assisted them in sifting through the inaccurate information regarding prenatal care and childcare that their mothers-in-law and other relatives had given them.
The results of the study suggest that the MCH handbook may be a useful tool for improving client-health provider communication as well as women's knowledge- and health-seeking behaviors related to pregnancy, new-born, and child health. [3] Yanagisawa et al. (2015) discovered that MCH Handbook users among pregnant Cambodian women had a better comprehension of pregnancy-related danger signals such edema, frequent vomiting, and seizures. Also, the guidance raised expectant women's knowledge of certain danger indicators, such as protracted labor, unusual presentation, and placenta accrete after delivery (Yanagisawa et al., 2015). Further information on anemia, parasites, and HIV infection was also included in the MCH guidebook. [4] According to 2009 Bangladeshi research, 78.0% of the women who used the MCH handbook understood the value of prenatal care, as opposed to the women in the control group. 55.9% of the women who used the MCH HB guide attended ANC visits as compared to 35.5% of the women in the control group, this difference demonstrates that the increase in knowledge may also have had an impact on behaviors. [5] Kawakatsu et al. (2015) assert that Western Kenyans' understanding of and conduct toward health concerns connected to fever and diarrhea were improved as a result of the MCH handbook. [6].
According to a study by Jeong, pregnant women in Korea who used the MCH Handbook knew more about the DPT vaccination than their peers (Jeong, 2004). Women were considerably more likely to get the vaccine after using the MCH handbook and learning about the DPT vaccination, demonstrating the connection between action and information (Jeong, 2004). [7]
According to Osaki et al. (2013), 47% of Indonesian women who had both the general record given to patients and the MCH handbook received all 12 doses of the immunization, as opposed to 25.1% of Indonesian women without both records. [8]
According to a 2007 study by Kusumayati and Nakamura, pregnant women in Indonesia who had access to an MCH handbook were 2.5 times more likely to utilize family planning and 3 times more likely to engage a trained birth attendant. Also, it was shown that women receiving ANC had read the MCH manual at least four times. According to a study by Osaki et al., women in Indonesia who used the MCH handbook attended ANC visits about 6.3 times more often than women in the control area, who only did so 5.6 times (2018). According to Osaki et al2018's [10] study, 54.6% of women who attended an ANC visit more than six times had an MCH guidebook. According to research by Isaranurug, in 2009, 83% of Thai women who used the MCH handbook had finished the pregnancy record in their handbook, 91.1% had finished the record of tetanus vaccinations, and 99% had finished the record of infant immunizations (Isaranurug, 2009). These percentages surpass the information that was first obtained in 1995 [11]. According to a research by Mori et al., pregnant women in Mongolia who utilized the MCH handbook visited prenatal clinics on average 6.9 times as compared to 6.2 times for the control group (2015). In 2015, Mori and co. Also, it was shown that women who read the MCH handbook had a higher likelihood of recognizing pregnancy-related problems (Mori et al., 2015). The reasons might be linked to women who read the guidebook being able to identify that they have one or more risk factors and then telling a healthcare professional about this knowledge (s).
Pregnancy-related constipation and morning sickness may be avoided by eating a balanced diet the whole time you're expecting (Stanford Children's Health, 2018). [13] A pregnant woman's diet is important for a healthy fetus since the nutrients that a developing infant acquires rely on the mother's diet (Ramakrishnan et al., 2012). [19] According to research by Osaki et al, moms who followed the advice in the MCH handbook were more likely to give their kids extra foods like fruit or fruit extract, meals high in protein, vitamins, and oil, two snacks per day, and vitamin A. 2018 (Osaki et al). in Osaki et al. Also, women who used the MCH handbook reported having less underweight neonates (5.2% vs. 14%) and children with delayed development (26.3% vs. 40.3%) than mothers in the control group. in Osaki and co. (2018). [10]
It has been shown that breastfeeding lowers the risk of gastrointestinal issues, upper and lower respiratory infections, and otitis media. The systolic blood pressure of older kids who have been breastfed for at least six months has been demonstrated to decrease (Allen and Hector, 2005). Babies who were exclusively breastfed for at least four months had a three times reduced chance of acquiring a major respiratory illness than newborns who were formula-fed, according to research by Bachrach et al. Moreover, research suggests that breastfeeding may lower the incidence of diarrhea-related mortality and morbidity, with the effect being highest in young children who are exclusively breastfed during the first six months of life. Despite the fact that breastfeeding has been shown to be a preventative measure against premenopausal breast cancer, prolonged nursing sessions are associated with greater protection. This may also be advantageous for mothers (Issaranurak et al., 2006; Ministry of Health – Thailand, 2006). [17]
According to studies by Fujimoto et al., in the Japanese cities of Gifu, Hiroshima, Niligata, Shizoaka, and Yokohama, 98.3% of pregnant women were found to be able to read and write in MCH handbooks (2001). 0.9 percent of the ladies lost the handbook (Fujimoto et al., 2001). 81.6% of the women said the MCH guide was helpful for learning about the suggested and needed immunizations, and 87% of the women thought it was helpful for getting ready for delivery. [18]
Hagiwaraa et al. found that reading the MCH Handbook increased users' perceptions of their ability to influence both their own and their children's health. The third step is planning for the family. In research by Dr. Shafi Bhuiyan, 42.1% of case group women and 35.3% of control group mothers used family planning during their most recent pregnancies, respectively. [1]
The population of Northern Bangladesh is overlooked and undervalued. They follow certain pregnancy-related superstitions, beliefs, and behaviors. Several expecting moms die because of them. Tools like the MCH HB guide will help to prevent these unfortunate occurrences by enhancing the health-related knowledge of women and their families and aiding them in taking early and appropriate action at the right time.
The results of this study shows that majority of the patients were young (<25 years), and had low levels of education, and were housewives. They had low socioeconomic status and their spouses were also not very educated and had low earning as well. In terms of women having health literacy, the overall results were less than 60%. The knowledge about maintaining a healthy pregnancy was seen in 34.37% women, Antenatal Health Care was found in 57.81%, knowledge about nutrition requirements during pregnancy was seen in 45.31%, knowledge about TT vaccine was shown by 21.35%, and 10.93% were found to know about pregnancy related dangers and warning signs. However, the area where women lacked significant knowledge was related to postpartum i.e., women who possessed knowledge about postpartum risk signs were only 4.16%, the ones with postpartum care information were 3.64%, whereas 3.12% knew about birth planning and postpartum birth control.
The results of this study show various areas that need improvement in order to provide better health care to women in Bangladesh. Difficulties in seeking health care due to lack of transportation, financial and emotional support are a concern, but the lack of information related to their healthcare is the most important factor that needs attention. The existing health record tools e.g., ANC, PNC, immunization, and treatment cards do not provide sufficient information. Due to lack of knowledge, these women have no pregnancy care such as ANC, PNC, delivery, and neonatal care. Also in rural areas, females give birth usually at home, without the help of any skilled birth attendant. Such pregnancies and deliveries are full of risks and thus the MMR and IMR stay high. Access to health information and provision of quality healthcare should therefore be a priority.
Conclusion
The cross-sectional study reveals that of the 192 pregnant women, only 34.37% have necessary knowledge required to continue a healthy pregnancy. 57.81% have knowledge about antenatal Care.45.31% of them knew about the necessary nutrition needed for them .21.35% were aware of TT Vaccine. Only 10.93% of the mothers had knowledge about pregnancy-related dangers and warning signs, 4.16% had knowledge about Postpartum risk signs, 3.64% women had knowledge about Postpartum Care, and those having Birth Planning and Postpartum Birth Control knowledge were 3.12% each.
Recommendations
According to the result of the Study, most pregnant women are less educated and unaware of the services that are available for their health and well-being. To understand this better, a Multi-Centre Study is recommended. An interventional study on Maternal and Child Health Handbook (MCH Handbook) that provides health information to the participants, may also increase the knowledge and utilization of facility based MCH services and safe deliveries for pregnant women.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org