International Journal of Clinical Otorhinolaryngology
OPEN ACCESS | Volume 2 - Issue 1 - 2025
ISSN No: - | Journal DOI: -

E.N. Oghenekaro1, O.B da Lilly-Tariah1, L.O. Onotai1, U.A. Oparaodu2*, A.O. Peterside1
1ENT Department, University of Port Harcourt teaching Hospital.
2ENT Department, College of Medical Sciences, Rivers State University, Port Harcourt.
*Corresponding author: U.A. Oparaodu, ENT Department, College of Medical Sciences, Rivers State University, Port Harcourt.
Received: March 15, 2026 | Accepted: March 30, 2026 | Published: April 15, 2026
Citation: E.N. Oghenekaro, O.B da Lilly-Tariah, L.O. Onotai1, U.A. Oparaodu, A.O. Peterside., (2026) “The Correlation of Tympanic Membrane Perforation on Hearing Loss in Port Harcourt, Nigeria. Vol 2: The Effect of Size and Site of Tympanic Perforation on Hearing Loss.” International Journal of Clinical Otorhinolaryngology, 3(1). DOI: 10.61148/IJCO/004/006.
Copyright: © 2026 U.A. Oparaodu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: The tympanic membrane (TM), commonly referred to as the eardrum, plays a crucial role in the auditory system by facilitating sound transmission from the external environment to the middle ear. Several factors influence the degree of hearing loss associated with TM perforations. Among these, the size and location of the perforation are of particular interest.
Aim: To determine the correlation between the size and site of tympanic membrane perforation and hearing loss among adult patients with tympanic membrane perforation in Port Harcourt, Nigeria.
Methodology: prospective study involved 70 adults (≥18 years) with unilateral tympanic membrane perforation. Perforation size and site were documented using photographic images. Air and bone conduction thresholds were measured using pure tone audiometry. Data were analysed to assess correlations between perforation characteristics and hearing loss.
Results: Findings from the study reveal 17.64 ± 15.81% area of tympanic membrane (TM) perforation. The various classes of the sizes of tympanic membrane perforation for small, medium and large were 72.9%, 24.3% and 2.9% respectively. There was correlation between the size (area) of tympanic membrane perforation and air conduction PTA values whereas no correlation between size of tympanic membrane perforation and bone conduction values. The results further demonstrates the location of tympanic membrane perforation with anterior inferior quadrant being the most affected membrane by over 58.3% and size of perforation and middle ear volume were the main factors associated with hearing loss (PTA air conduction).
Conclusion and Recommendations: This study demonstrates that Small perforations were most common; larger size and posterior location caused greater hearing loss, emphasizing importance of size and site. Furthermore, these findings provide valuable evidence to support clinical decision-making regarding surgical intervention in tympanic membrane perforation.
Tympanic membrane perforation; perforation size; perforation site; hearing loss
The tympanic membrane (TM), commonly referred to as the eardrum, plays a crucial role in the auditory system by facilitating sound transmission from the external environment to the middle ear. When a perforation occurs, it compromises this function by reducing the available surface area for sound conduction and allowing direct entry of sound waves into the middle ear 1, 2. Research has shown that TM perforation can result in conductive hearing loss (CHL), ranging from negligible to as much as 50 decibels (dB) 3.
Several factors influence the degree of hearing loss associated with TM perforations. Among these, the size and location of the perforation are of particular interest. Multiple studies indicate a direct correlation between the size of TM perforation and the severity of hearing loss: the larger the perforation, the greater the loss 4, 5. Additionally, hearing loss varies inversely with the volume of air within the middle-ear and mastoid cavity, meaning that individuals with smaller middle ear cavities tend to experience more severe CHL for the same perforation size 6, 7.
The impact of the location of TM perforation on hearing loss, however, remains a topic of debate. Some researchers suggest that the perforation site does not significantly influence hearing loss 3, 4, while others propose that perforations in the postero-inferior quadrant, near the round window, result in greater hearing impairment 2, 8. The theoretical basis for this observation is that posteriorly located perforations may allow sound energy to bypass the ossicular chain, leading to an inefficient transmission of sound and a more pronounced hearing deficit.
Moreover, the chronicity of TM perforations also contributes to variations in hearing loss severity. Long-standing perforations, especially those associated with recurrent infections, may lead to sclerotic changes in the mastoid air cells, further compounding the hearing impairment 9, 10. Although acute perforations resulting from trauma or acute otitis media often heal spontaneously, persistent perforations may necessitate surgical intervention, such as tympanoplasty, to restore auditory function 11.
Given the variability in findings regarding the effect of perforation site and size on hearing loss, this study aims to determine the correlation between the size and site of tympanic membrane perforation and hearing loss among adult patients with tympanic membrane perforation in Port Harcourt, Nigeria
Materials and Methods
Study Area: This study was conducted at the University of Port Harcourt Teaching Hospital (UPTH), Rivers State, Nigeria, a reference hospital with a bed capacity of 800. The ENT clinic operates four days a week, serving approximately 4,200 patients annually.
Study Design: A hospital-based cross-sectional study was employed, focusing on patients with unilateral tympanic membrane (TM) perforation attending the ENT clinic.
Study Population: The study included adult patients ≥18 years with unilateral TM perforation, while the contralateral non-perforated ear served as the control.
Inclusion Criteria
Exclusion Criteria
Study Duration: The study spanned from August 1, 2018, to July 31, 2019.
Scope of Study: The study assessed the degree, pattern, and type of hearing loss associated with TM perforations, alongside middle ear volume. Assessment methods included otoscopy, video otoscopy, pure tone audiometry, and tympanometry.
Sample Size Determination: Using Cochran’s formula, the minimum sample size was calculated to be 61, with a 10% allowance for non-response, resulting in a final sample size of 70 patients (140 ears).
Materials:
Sampling Method: A cluster sampling technique was employed, selecting two clinic days (Monday to Thursday) randomly. All patients with unilateral TM perforation on those days were included in the study.
Data Collection: A structured, interviewer-administered questionnaire was used to gather demographic and clinical data from each participant. The questionnaire included questions on the patient's age, gender, and medical history, with particular focus on ear-related symptoms, such as pain, drainage, and hearing loss. It also addressed potential causes of tympanic membrane perforation, such as trauma, ear infections, or ototoxicity due to medication. Further details were collected regarding the patients’ medical history, including conditions like diabetes, sickle cell anemia, and prior ear surgeries. Information on any history of ototoxicity or retroviral infections was also documented. Following the interview, patients underwent pure tone audiometry (PTA), which was performed using a calibrated Madsen Itera audiometer inside a soundproof booth. The PTA evaluated both air and bone conduction thresholds at frequencies of 250, 500, 1000, 2000, 4000, and 8000 Hz to assess the type and degree of hearing loss 1, 12. Air conduction testing was done using supra-aural earphones, while bone conduction testing was performed using a bone oscillator placed over the mastoid bone 12. Air conduction masking was performed when the air conduction threshold in the perforated ear was 40 dB greater than the bone conduction threshold in the normal contralateral ear, using the plateau seeking method. Bone conduction masking was done for all patients at all frequencies. Pure-tone averages were calculated for air and bone conduction at 500, 1000, 2000, and 4000 Hz 12, 13. An air-bone gap greater than 10 dB in these frequencies was considered significant for diagnosing conductive hearing loss 12. Sensorineural hearing loss was defined as air and bone conduction averages within 10 dB, with thresholds above 25 dB HL 12. Mixed hearing loss was defined as a gap greater than 10 dB between air and bone conduction averages, with thresholds above 25 dB HL at any frequency 12. Results was used to grade hearing threshold into mild, moderate, severe and profound hearing according to WHO 14. These assessments provided critical data for analyzing the relationship between tympanic membrane perforations and hearing impairment in the study population. Video otoscopy was performed using a probe with an appropriate speculum, and the tympanic membrane was fully visualized. A digital image of the perforation was captured, and its size was analyzed with Image J software by measuring the perforated area in relation to the tympanic annulus1. The site of the perforation was recorded, referencing an imaginary line through the manubrium of the tympanic membrane (TM). Sites included anterio-superior, posterio-superior, anterio-inferior, posterior-inferior, subtotal, and central perforations1.
These assessments provided critical data for analyzing the relationship between tympanic membrane perforations and hearing impairment in the study population..
Data Analysis
Data were analyzed using SPSS version 20. Descriptive statistics (mean, standard deviation) were used for numerical data, while categorical data were analyzed using frequencies and proportions. Paired t-tests, Chi-square tests, Pearson’s correlation, and linear regression analyses were used to assess the correlation between TM perforation size, site, and hearing loss. A p-value of ≤ 0.05 was considered statistically significant.
Ethical Considerations: Ethical approval was obtained from the Research and Ethics Committee of UPTH. Informed consent was obtained from all participants, with full disclosure of the study procedure.
Results
Table 1: Summary measures of the area of tympanic membrane (TM) perforation in percentages
|
|
|
|
Summary measures |
Area of TM Perforation (%) |
|
Mean ± SD |
17.64 ± 15.81 |
|
Median |
13.04 |
|
Minimum |
0.08 |
|
Maximum |
60.54 |
SD – Standard deviation
As seen in figure 1, the distribution shows the various classes of the sizes of tympanic membrane perforation. The class small accounted for 72.9% while large was 2.9%. Very large perforation was not seen in any ear.
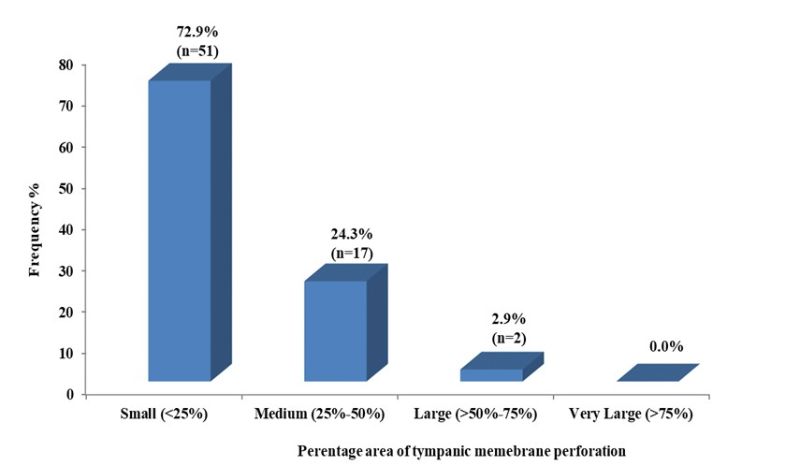
Figure 1: Distribution of the categories of percentage area of tympanic membrane perforation.
As shown in figure 2, there is a correlation between the size (area) of tympanic membrane perforation and air conduction PTA values. This is reflected in the p-value of 0.001 being significant and the Pearson’s correlation r = 0.376 showing a weak correlation.
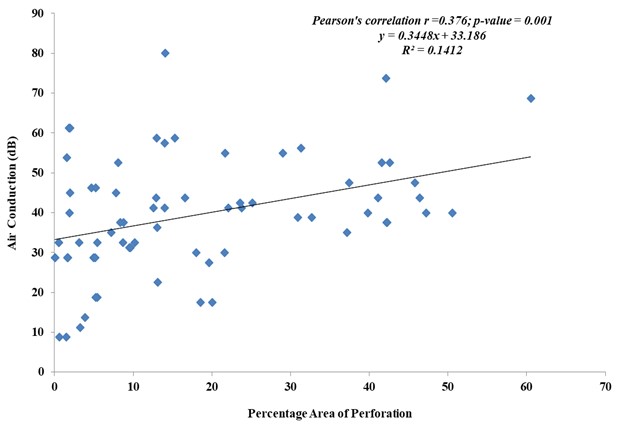
Figure 2. Correlation between area of perforation (%) and air conduction hearing threshold (dB).
From figure 3 below. There is no correlation between size of tympanic membrane perforation and bone conduction values as illustrated with the p-value not being significant 0.949 and the Pearson’s correlation also showing no correlation with values of r=0.008
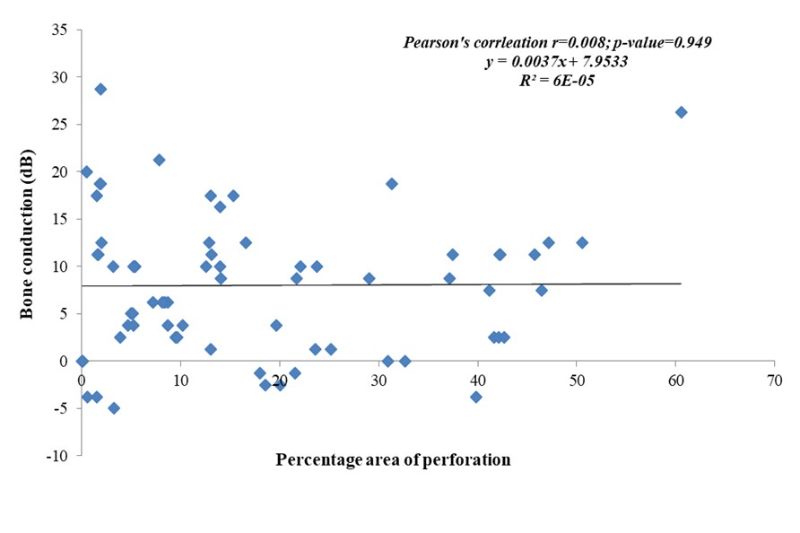
Figure 3. Correlation between area of perforation (%) and bone conduction hearing threshold (dB).
From the illustration below as shown in figure 4, the means area of tympanic membrane perforation was lest among patient with normal hearing and highest among patient with mixed hearing.
However, the p-value was not significant.
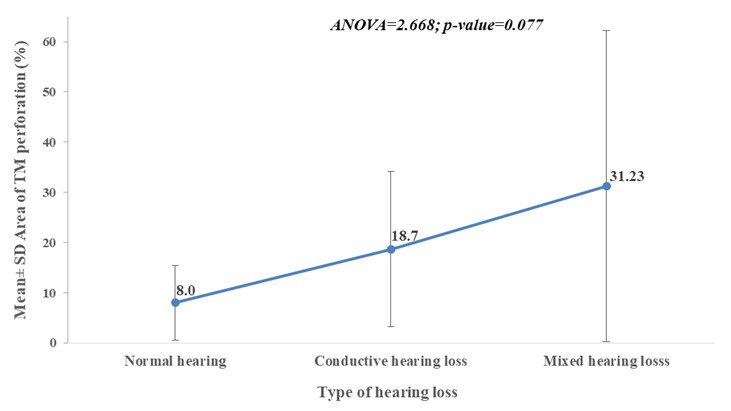
Figure 4: Error bar chart showing mean area of tympanic membrane perforation across category of hearing loss in the affected ear.
Table 2: Number of segments involved in tympanic membrane perforation
|
Number of quadrants |
Frequency |
Percentage % |
|
One quadrants only |
36 |
51.4 |
|
Two quadrants only |
16 |
22.9 |
|
Greater than two quadrants |
18 |
25.7 |
|
Total |
70 |
100.0 |
The distribution as shown in figure 5, demonstrates the location of tympanic membrane perforation. With anterior inferior quadrantbeing the most affected 58.3%. membrane
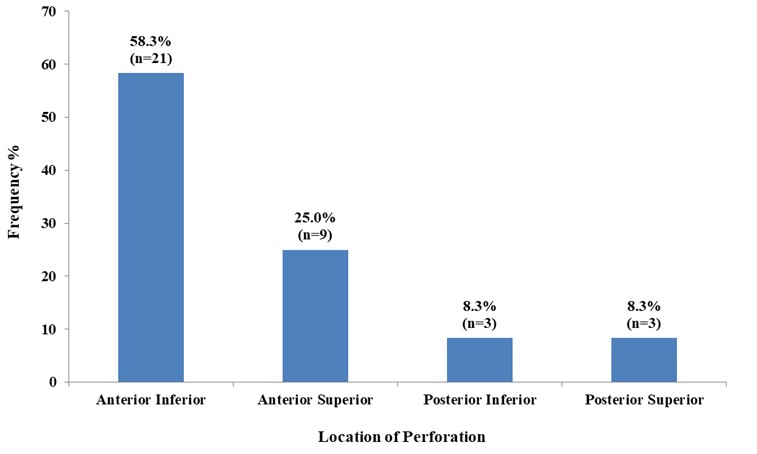
Figure 5: Location of perforation among the patients with only one quadrant perforation (N=36).
Table 3: Tympanic membrane location and hearing threshold (dB)…….. (N=36).
|
Location |
Number |
Hearing threshold (dB) Mean±SD |
|
Anterior Superior |
9 |
27.50±11.40 |
|
Anterior Inferior |
21 |
24.06±13.40 |
|
Posterior Superior |
3 |
37.00±15.58 |
|
Posterior Inferior |
3 |
43.67±12.26 |
SD—Standard deviation ANOVA=4.858; p-value=0.007* *Statistically significant
As demonstrated in figure 6, there is no correlation between air conduction and the number of quadrants involved. The p-value of 0.066 is not significant and spearman’s correlation value of 0.221 signify no correlation.
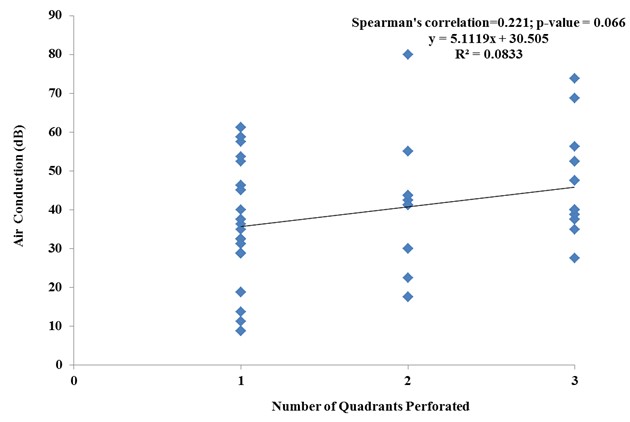
Figure 6. Correlation between number of segments of tympanic membrane location and air conduction hearing threshold.
From figure 7 below, there is no correlation between bone conduction and the number of quadrants involved. The p-value of 0.368 is not significant and spearman’s correlation value of 0.221 signify no correlation.
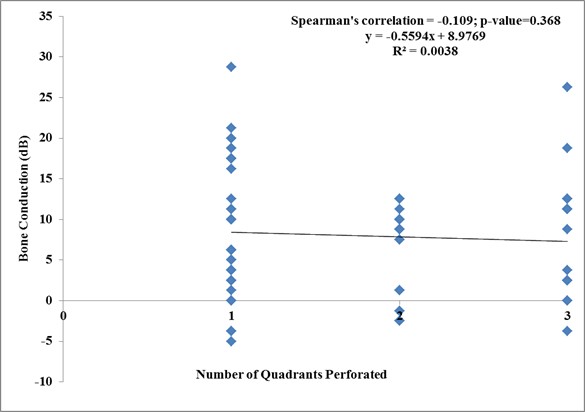
Figure 7. Correlation between number of quadrants perforated bone conduction hearing threshold.
Discussion
The size and site of tympanic membrane perforation play a crucial role in determining the degree of hearing loss. The tympanic membrane acts as an essential component in sound conduction, and its integrity is necessary for efficient sound transmission. The impact of perforation on hearing loss depends on multiple factors, including the extent of the remaining functional membrane, the involvement of different quadrants, and the anatomical positioning of the perforation. This discussion explores the correlation between tympanic membrane perforation size, location, and the resultant hearing impairment.
The mean size of tympanic membrane perforation was 17.64 ± 15.81, while the range was 0.08% – 60.54%. Figure 1 showed that a large number of patients (72.9%) had small perforations (<25%
of the total surface area of the tympanic membrane), similar to the report by Orji and Agu in 2009 in Nigeria and others 12, 15, 16. This differs from the finding of Nahata et al. in 2016 in India, who noted that patients with large perforations were the most commonly affected 5.
It is imperative to state that a linear correlation and significant p-value were observed between the size of tympanic membrane perforation and air conduction hearing (conductive hearing loss) in this study, as shown in Figure 2. This is in keeping with documentation in several works 1, 2, 6, 8, 17. This implies that the tympanic membrane plays a major role in sound transmission, such that even though there is a perforation, the size of the remnant tympanic membrane is still important. Larger perforations decrease the physiologic vibrating area of the tympanic membrane and also reduce the proportional difference between the tympanic membrane and the stapes footplate (loss of hydraulic action) 8, 18, 19, thus resulting in reduced amplification and hearing loss. It was also observed that there was no correlation and significant p-value for bone conduction testing. Other studies have reported similar findings; this is most likely due to the fact that the main pathology in these patients affects the conduction pathway 9, 12.
This study observed that more patients had only one quadrant affected, 36 (51.4%), out of which the anterior inferior quadrant had the highest occurrence, 21 (58.3%). Similar to Aslıer et al. in 2019, they reported more anterior perforations 16. This is at variance with the study by Ibekwe et al. in 2009 and Sood A.S. et al. in 2018, who reported more multi-quadrant perforations, 77.9% and 80%, respectively 1, 19. Although some patients with single T M perforation had more than one quadrant involved, there was no patient with multiple perforations.
It was observed, as shown in Table 4, that posterior perforations had higher hearing thresholds compared to anterior perforations with a significant p-value (0.007). This is in agreement with studies by Maharjan et al. and Pannu et al. 2, 10, but differs from other works that reported that the site/location of tympanic membrane perforation does not have a significant effect on hearing loss 3, 4, 6, 17, 20. The posterior quadrant being associated with greater hearing loss is possibly due to the widely held theory of the “round window baffle,” which is the shielding effect the tympanic membrane has over the round window 1, 4. On the contrary, Figures 6 and 7 showed no correlation between the number of quadrants affected and the hearing threshold of both air and bone conduction. Therefore, small and anterior tympanic membrane perforations and large middle ear volume could explain why some patients still have normal hearing with tympanic membrane perforation.
Conclusion
This study revealed that small-sized perforations were the most common, with a direct correlation between perforation size and the degree of hearing loss. Anterior perforations were the most frequently observed type, whereas posterior perforations were associated with greater hearing loss, demonstrating statistical significance. These findings highlight the importance of considering both the size and location of tympanic membrane perforations in the clinical management of patients.
Declarations:

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org