International Journal of Clinical Otorhinolaryngology
OPEN ACCESS | Volume 2 - Issue 1 - 2025
ISSN No: - | Journal DOI: -

E.N. Oghenekaro1, O.B da Lilly-Tariah1, L.O. Onotai1, U.A. Oparaodu2*, A.O. Peterside1
1ENT Department, University of Port Harcourt teaching Hospital.
2ENT Department, College of Medical Sciences, Rivers State University, Port Harcourt.
*Corresponding author: U.A. Oparaodu, ENT Department, College of Medical Sciences, Rivers State University, Port Harcourt.
Received: March 15, 2026 | Accepted: March 30, 2026 | Published: April 15, 2026
Citation: E.N. Oghenekaro, O.B da Lilly-Tariah, L.O. Onotai1, U.A. Oparaodu, A.O. Peterside., (2026) “The Correlation of Tympanic Membrane Perforation on Hearing Loss in Port Harcourt, Nigeria. Volume 3: The Effect of Middle Ear Volume on Hearing Loss.” International Journal of Clinical Otorhinolaryngology, 3(1). DOI: 10.61148/IJCO/004/005.
Copyright: © 2026 U.A. Oparaodu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The human middle ear plays a crucial role in sound transmission, as it serves as the conduit for the conduction of sound vibrations from the external ear to the inner ear. Despite the growing body of research on middle ear anatomy and its effects on hearing, there is a lack of studies investigating the specific relationship between middle ear volume and hearing loss in the Nigerian population. This study aims to enhance the understanding of the complex relationship between middle ear volume and hearing loss, particularly in the context of TM perforations. A structured, interviewer-administered questionnaire was used to gather demographic and clinical data from each participant. A hospital-based cross-sectional study was employed on 70 patients, focusing on patients with unilateral tympanic membrane (TM) perforation attending the ENT clinic, University of Port Harcourt using various assessment methods which include otoscopy, video otoscopy, pure tone audiometry, and tympanometry. The result indicates that external ear volume (control ear) and middle ear volume (perforated ear) had standard mean value of 1.45 ± 0.32mls and 4.35 ± 2.92mls. 52.9% of participants had small ear volume (≤ 4.3mls) while 47.1% participants had higher ear volume (>4.3mls). There is inverse correlation between middle ear volume and air conduction PTA values whereas no correlation between middle ear volume and bone conduction values. Comparing the hearing threshold (dB) between low and high PTA frequencies in the perforated ear, Air Conduction had a low frequency 42.21 ± 17.39 and high frequency of 43.93 ± 22.29 (dB) while Bone Conduction had a low frequency 0.39 ± 8.50 and high frequency of 9.11 ± 14.03 (dB). This research may inform the development of more targeted treatment strategies, such as the use of hearing aids or surgical interventions, for patients with tympanic membrane perforation. Ultimately, the findings of this study could contribute to improving the quality of life for individuals suffering from hearing loss due to tympanic membrane perforation in Nigeria.
Tympanic membrane perforation, human middle and external ear volume, Air Conduction, Bone Conduction
The human middle ear transmits sound from the external to the inner ear and includes structures such as the tympanic cavity, eustachian tube, aditus, attic, antrum, and mastoid air cells 1. These components work together to ensure effective sound conduction and pressure regulation 2 1. The eustachian tube also helps ventilate the middle ear and clear secretions 3. Understanding the volume of the middle ear is important, especially in cases of tympanic membrane (TM) perforation, as it can influence hearing loss and clinical outcomes 4, 5..
Mastoid pneumatization, the formation of air cells in the mastoid bone, is important for sound transmission. The mastoid antrum, a large and consistent mastoid air cell, communicates with the attic of the middle ear through the aditus3. Mastoid pneumatization commences from 33rd week before birth, and develops until the age of 15years for male and 10years for female 5. In a typical adult, the mastoid has a volume of about 2 milliliters 3. The mastoid antrum connects to the middle ear via the aditus. Well-pneumatized mastoids, with many thin septa, enhance sound conduction, while sclerotic mastoids, lacking air cells, impair sound conduction 1, 2.. The volume and status of mastoid air cells significantly influence hearing efficiency and are key factors in assessing and managing hearing loss 2.
Research shows that middle ear volume is a key factor in hearing loss, particularly in cases of tympanic membrane (TM) perforation. Studies across different populations (Asia and America) have found that smaller middle ear spaces correlate with larger air-bone gaps and greater conductive hearing loss 5, 6. Mehta et al., Park et al., and Ahn et al. all support this link, emphasizing that reduced mastoid air cell volume or sclerotic mastoids worsen hearing 4 5, 7.
Middle ear (ME) volume has been identified as a key factor in determining the degree of hearing loss in ears with tympanic membrane (TM) perforations. Smaller ME volumes are associated with larger air-bone gaps, and identical perforations can result in hearing losses that differ by up to 35 dB if ME volumes vary significantly 4, 7, 8.
The degree of mastoid pneumatization varies widely among individuals. Normal mastoid volumes range from 2 to 20 ml 5. A Korean study reported an average mastoid pneumatization volume of 7,095.2 mm³ with a large standard deviation (3,087.1 mm³), indicating significant individual variation 5. Similarly, a Norwegian study found the average middle ear volume to be 6.5 ± 3.7 ml 6. These differences may result from postnatal pathological changes, such as otitis media and eustachian tube dysfunction 5.
Mehta et al. (2006) using tympanometry found that ears with ME volumes ≤4.3 ml had significantly greater conductive hearing loss than those with volumes >4.3 ml4. Park et al. (2015) found an inverse correlation between hearing loss and the combined volume of the middle ear and mastoid 5. Using temporal bone CT scans, they measured these volumes and grouped patients into four categories based on volume size, (group A: 1–2,400 mm3; group B: 2,401–4,800 mm3; group C: 4,801– 7,200 mm3; group D: >7,200 mm3)5. Importantly, their analysis showed that middle ear and mastoid volume was a more significant predictor of hearing loss than the size of tympanic membrane perforation 5.
Ahn et al. compared middle ear (ME) volume measurements using tympanometry and CT scans in patients with unilateral chronic otitis media. ME volumes measured by CT in normal ears were significantly larger than in lesioned ears. In ears with tympanic membrane (TM) perforation, tympanometry showed a strong linear correlation with CT measurements 7. Manjuran & Bahuleyan assessed mastoid air space volume via digital X-ray, grouping patients into sclerotic and cellular mastoids. They found that mastoid air space volume is inversely proportional to conductive hearing loss 2.
There is a lack of research in Port Harcourt, Nigeria, on how middle ear volume affects hearing loss in patients with tympanic membrane (TM) perforation. While previous studies have explored the size and site of TM perforations, the impact of middle ear volume, including mastoid pneumatization, remains under-investigated in this population. This study aims to address that gap by evaluating how different patterns of middle ear pneumatization (sclerotic vs. well-pneumatized) influence hearing outcomes in Nigerian patients. Understanding the inverse relationship between mastoid volume and conductive hearing loss could improve diagnostic accuracy. The study will assess the correlation between middle ear volume and hearing loss in patients with TM perforation. This research will contribute valuable knowledge to the clinical understanding of middle ear anatomy’s role in hearing loss and help shape future practices and research in the region.
Materials And MethoDS
Study Area: This study was conducted at the University of Port Harcourt Teaching Hospital (UPTH), Rivers State, Nigeria, a reference hospital with a bed capacity of 800. The ENT clinic operates four days a week, serving approximately 4,200 patients annually.
Study Design: A hospital-based cross-sectional study was employed, focusing on patients with unilateral tympanic membrane (TM) perforation attending the ENT clinic.
Study Population: The study included adult patients ≥18 years with unilateral TM perforation, while the contralateral non-perforated ear served as the control.
Inclusion Criteria
Exclusion Criteria
Study Duration: The study spanned from August 1, 2018, to July 31, 2019.
Scope of Study: The study assessed the degree, pattern, and type of hearing loss associated with TM perforations, alongside middle ear volume. Assessment methods included otoscopy, video otoscopy, pure tone audiometry, and tympanometry.
Sample Size Determination: Using Cochran’s formula, the minimum sample size was calculated to be 61, with a 10% allowance for non-response, resulting in a final sample size of 70 patients (140 ears).
Materials
Sampling Method: A cluster sampling technique was employed, selecting two clinic days (Monday to Thursday) randomly. All patients with unilateral TM perforation on those days were included in the study.
Data Collection
A structured, interviewer-administered questionnaire was used to gather demographic and clinical data from each participant. The questionnaire included questions on the patient's age, gender, and medical history, with particular focus on ear-related symptoms, such as pain, discharge, and hearing loss. It also addressed potential causes of tympanic membrane perforation, such as trauma, ear infections, or ototoxicity due to medication. Further details were collected regarding the patients’ medical history, including conditions like diabetes, sickle cell anemia, and prior ear surgeries. Information on any history of ototoxicity or retroviral infections was also documented. Following the interview, patients underwent pure tone audiometry (PTA), which was performed using a calibrated Madsen Itera audiometer inside a soundproof booth. The PTA evaluated both air and bone conduction thresholds at frequencies of 250, 500, 1000, 2000, 4000, and 8000 Hz to assess the type and degree of hearing loss 9, 10. Air conduction testing was done using supra-aural earphones, while bone conduction testing was performed using a bone oscillator placed over the mastoid bone 10. Air conduction masking was performed when the air conduction threshold in the perforated ear was 40 dB greater than the bone conduction threshold in the normal contralateral ear, using the plateau seeking method. Bone conduction masking was done for all patients at all frequencies. Pure-tone averages were calculated for air and bone conduction at 500, 1000, 2000, and 4000 Hz 10, 11. An air-bone gap greater than 10 dB in these frequencies was considered significant for diagnosing conductive hearing loss 10. Sensorineural hearing loss was defined as air and bone conduction averages within 10 dB, with thresholds above 25 dB HL 10. Mixed hearing loss was defined as a gap greater than 10 dB between air and bone conduction averages, with thresholds above 25 dB HL at any frequency 10. Results was used to grade hearing threshold into mild, moderate, severe and profound hearing according to WHO 12.
A tympanometric assessment of the middle ear volume (MEV) was conducted for both ears of each patient. A 226Hz frequency tympanometer probe with a clean tip of appropriate size and shape was used to ensure an airtight seal in the ear canal 7, 13. The probe was directed towards the tympanic membrane for accurate measurements. For patients with a perforated tympanic membrane (TM), both the middle ear volume and external auditory canal (EAC) volume were measured, and a type B tympanogram (flat) was expected .4, 7. In contrast, for non-perforated ears, only the EAC volume was recorded.
For patients with unilateral TM perforation, the MEV was calculated by subtracting the EAC volume of the contralateral normal ear from the total estimated MEV of the perforated ear 4, 5, 7. Studies have shown no significant difference between the right and left EAC volumes in individuals 7.
The MEV was then categorized into four groups based on Park et al.'s classification: Group A (1–2,400 mm³), Group B (2,401–4,800 mm³), Group C (4,801–7,200 mm³), and Group D (>7,200 mm³) 5. The maximum volume measurable with the Madsen Zodiac 901 tympanometer was 9.99 mL.
These assessments provided critical data for analyzing the relationship between tympanic membrane perforations and hearing impairment in the study population..
Data Analysis
Data were analyzed using SPSS version 20. Descriptive statistics (mean, standard deviation) were used for numerical data, while categorical data were analyzed using frequencies and proportions. Paired t-tests, Chi-square tests, Pearson’s correlation, and linear regression analyses were used to assess the correlation between TM perforation size, site, and hearing loss. A p-value of ≤ 0.05 was considered statistically significant.
Ethical Considerations
Ethical approval was obtained from the Research and Ethics Committee of UPTH. Informed consent was obtained from all participants, with full disclosure of the study procedure.
Results
Table 1: Summary measures of external ear volume (control ear) and middle ear volume (perforated ear)
|
|
Control Ear |
|
Perforated Ear |
|
Summary measures |
External Ear Volume |
|
Middle Ear Volume |
|
Mean ± SD |
1.45 ± 0.32mls |
|
4.35 ± 2.92mls |
|
Median |
1.44mls |
|
4.25mls |
|
Minimum |
0.47mls |
|
0.07mls |
|
Maximum |
2.43mls |
|
8.18mls |
SD – Standard deviation
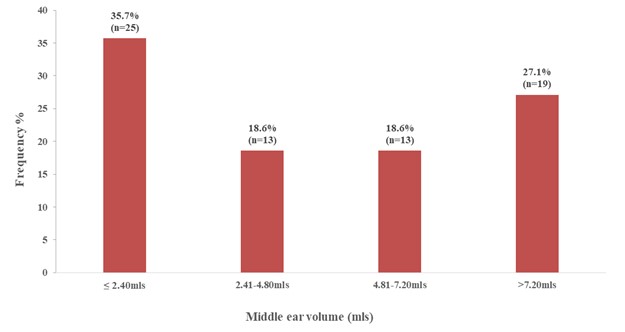
Figure 1. Distribution of middle ear volume categories
Based on the classification by Mehta et al., the figure 2 below Small (≤ 4.3mls) represented 52.9% and large (>4.3mls) representing 47.1% of the patient recruited for this study.
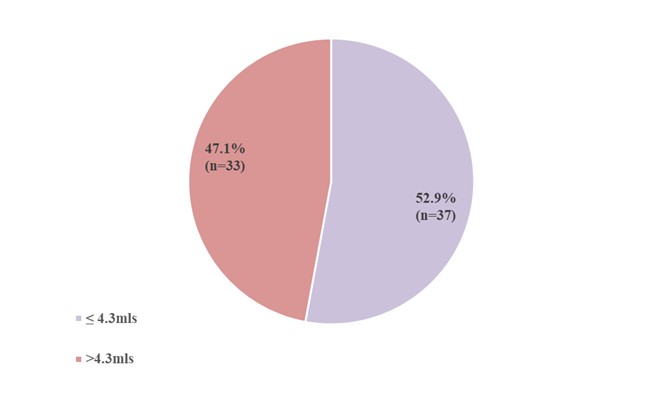
Figure 2. Distribution of middle ear volume in affected ears
As shown in figure 3, there is an inverse correlation between middle ear volume and air conduction PTA values. This is reflected in the p-value of 0.001 being significant and the Pearson’s correlation r = 0.452 showing a near moderate correlation.
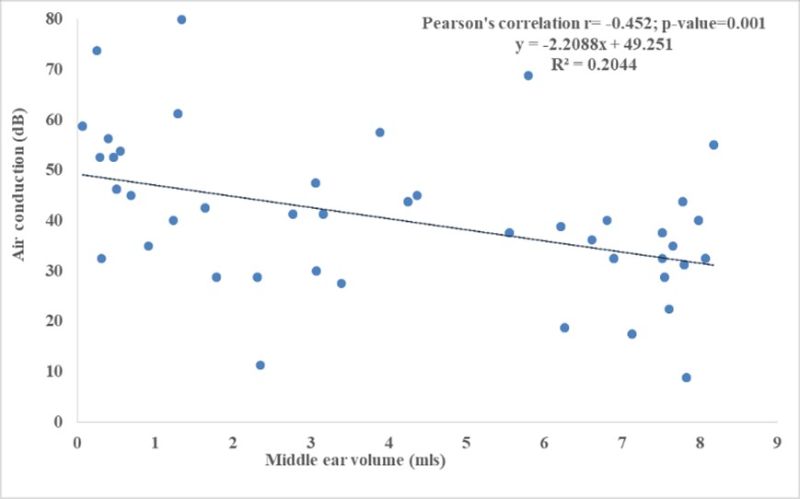
Figure 3. Correlation between middle ear volume and air conduction hearing threshold
On the contrary the figure 4 below, shows no correlation between middle ear volume and bone conduction values as noticed. The p-value is not significant 0.600 and the Pearson’s correlation also showing no correlation with values of r = -0.0041
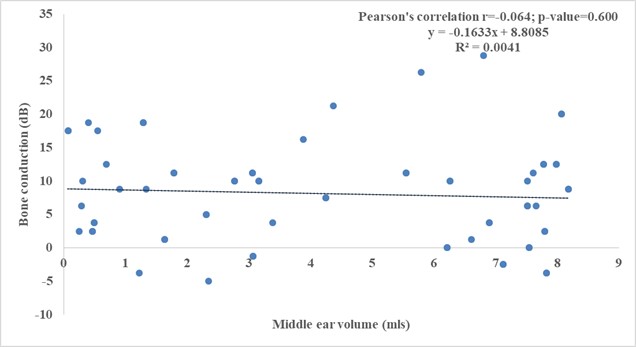
Figure 4. Correlation between middle ear volume and bone conduction hearing threshold
Table 2: Correlations between middle ear volume and patient’s characteristics (age, BMI, duration of symptoms and height)
|
|
Middle Ear Volume |
|
|
Variables |
Correlation Coefficient |
p-value |
|
Age |
-0.040 |
0.747 |
|
BMI |
-0.254 |
0.043* |
|
Duration of Symptoms |
-0.332 |
0.005* |
|
Height |
0.167 |
0.187 |
*Statistically Significant
It was noticed that 8000Hz was the most affected frequency with a mean air conduction value of 46.81dB followed by 250Hz. The least affected frequency was 1000Hz with 34.31dB as seen in figure 5 below.
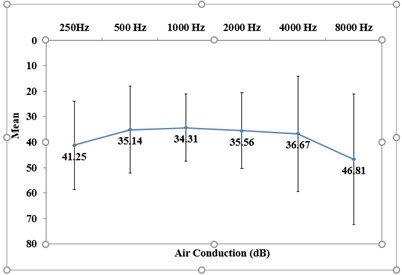
Figure 5: Mean values across PTA frequencies (Air Conduction)
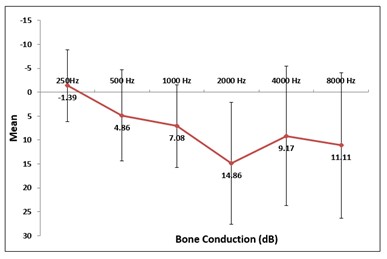
Figure 6: Mean values across PTA frequencies (Bone Conduction)
Table 3: Comparison of hearing threshold (dB) between low and high PTA frequencies in the perforated ear
|
Hearing threshold |
Low frequency PTA Mean ± SD |
High frequency PTA Mean ± SD |
t* |
p-value |
|
Air Conduction (dB) |
42.21 ± 17.39 |
43.93 ± 22.29 |
7.748 |
0.001** |
|
Bone Conduction (dB) |
0.39 ± 8.50 |
9.11 ± 14.03 |
0.907 |
0.366 |
SD – Standard deviation *Paired t-test **Statistically significant
Table 5: Multiple linear regression analysis of factors associated with hearing loss (PTA air conduction)
|
Factors |
Coefficient (B) |
95% Confidence Interval Lower Upper |
p-value |
|
|
Duration of symptoms |
-0.159 |
-0.415 |
0.098 |
0.222 |
|
Site of perforation |
0.015 |
-4.155 |
4.186 |
0.994 |
|
Size of perforation |
0.346 |
0.116 |
0.576 |
0.004* |
|
Middle ear volume |
-2.312 |
-3.377 |
-1.248 |
0.0001* |
|
Constant |
45.023 |
- |
- |
0.0001 |
*Statistically significant
Discussion:
Middle ear volume is a critical anatomical factor that plays a significant role in sound transmission and hearing function2. Variations in middle ear volume can contribute to different patterns of hearing loss, particularly conductive hearing loss. In this study, the mean middle ear volume and its correlation with air conduction testing were evaluated in a population of black Africans, and the findings were then compared with those from American and Asian populations. The results indicated that the mean middle ear volume in this cohort was 4.35 ± 2.92 mL, which closely aligns with the findings of Mehta et al. and Casale et al., both of which reported similar volumes among American populations 4, 14. Specifically, Mehta et al. observed a mean of 4.3 mL, while Casale et al. noted a mean of 4.4 mL in their respective studies in the United States 4, 14. These findings suggest that the middle ear volume in black Africans is comparable to that of Americans, although it is important to note the multi-racial complexity of the American population, which could contribute to variability in the results.
In contrast, Jae-Yoon Ahn et al. in Seoul, Korea, reported a significantly smaller mean middle ear volume of 1.5 ± 1.4 mL, which raises the possibility of smaller middle ear volumes among Asians 7. This difference may be attributed to various factors, including the generally smaller stature of Asians compared to African Americans, Caucasians, and other populations, as suggested by previous studies 15-17. The significant variation in middle ear volume observed between these groups underscores the need for population-specific normative data when assessing middle ear health. The mean external canal volume in this study was 1.45 ± 0.32mls. This closely mirrors the finding of Jae-Yoon Ahn et al who recorded 1.4 ± 0.3 mL but differs from Mehta R.P. et al that observed 1.14mls.4, 7
An intriguing finding from this study was the inverse correlation between middle ear volume and conductive hearing loss. This was statistically significant and aligns with findings from previous studies by Park et al., Mehta et al and others.4, 5, 8, 18. The diminished resonation space in individuals with smaller middle ear volumes likely results in poorer sound transmission, which may explain the observed association between reduced middle ear volume and increased conductive hearing loss. This relationship highlights the importance of considering middle ear volume when diagnosing and managing hearing loss in affected populations.
Further analysis revealed that there was a correlation between the duration of symptoms, body mass index (BMI), and middle ear volume. However, no significant correlation was reported between height and age of the patient and middle ear volume, as shown in Table 3. These findings suggest that while BMI and the duration of symptoms may influence the middle ear volume, factors like height and age do not have a considerable effect. The lack of correlation with age may indicate that other factors, such as systemic health conditions or ear infections, play a more significant role in middle ear volume changes than age alone.
Regression analysis in this study was conducted for various co-factors to evaluate which of these distinct co-factors independently affects hearing loss in these patients. It was noted that middle ear volume was the most significant independent co-factor affecting hearing loss, followed by the size of the perforation. Interestingly, the site of perforation and the duration of symptoms were not statistically significant, suggesting that these factors may not have as substantial an impact on hearing loss as previously thought. This finding challenges the conclusions of some previous studies, such as those by Mehta et al., which highlighted the site and duration of perforation as key factors in determining hearing outcomes 4. This may reflect the complexity of hearing loss in patients with middle ear dysfunction, which is influenced by a range of interrelated factors that can vary across populations.
The study also examined frequency-specific hearing loss, noting that the most affected frequencies for air conduction were 8000 Hz (46.81 dB) and 250 Hz (41.25 dB), with speech frequencies being the least affected. This finding is consistent with the inverted V-shaped audiogram observed by Nahata et al., where higher and lower frequencies were more affected than mid-range frequencies 19. However, contrasting results have been reported by Orji and Agu, who noted that high frequencies were most affected, while Ristovska et al. found that lower frequencies were more severely impacted 10, 20. These variations could be attributed to differences in the underlying causes of conductive hearing loss, such as the site of tympanic membrane perforation, the duration of perforation, or the presence of middle ear pathology, factors that could have influenced the results.
Conclusion
This study provides valuable insights into the relationship between middle ear volume and hearing loss in Black Africans. An inverse correlation was observed between middle ear volume and hearing levels in patients with tympanic membrane perforations, with most patients having a large middle ear volume. The study also demonstrates that both BMI and symptom duration have a statistically significant impact on middle ear volume. These findings highlight the importance of assessing middle ear volume in the clinical management of these patients.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org