Gastroenterology and Hepatology Research
OPEN ACCESS | Volume 7 - Issue 1 - 2026
ISSN No: 2836-2888 | Journal DOI: 10.61148/2836-2888/GHR


Running Title: Efficacy of Mirikizumab in patients having Inflammatory Bowel Disease
Aderinsola Wale-Oyedele¹, Afshan Jabeen², Sadia Siddiqui³, Lohana Pooja⁴, Amina Khalid⁵, Sunny Kumar⁶, Nisha Kumari⁴, Chandar Kanta Lohana⁴, FNU Gyaneshwari⁴, Bushra Ghafar⁷, Fizza Raza³, Keertan Khemani³, Hira Riaz⁸*
¹MBBS, Obafemi Awolowo University, Ile-Ife, Nigeria.
²MBBS, University of Rajasthan, Jaipur, India.
³MBBS, Jinnah Sindh Medical University, Karachi, Pakistan.
⁴MBBS, Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan.
⁵MBBS, Gannan Medical University, China.
⁶MBBS, The Wright Center for Graduate Medical Education, Pennsylvania, USA
⁷MBBS, Quaid-e-Azam Medical College, Bahawalpur, Pakistan.
⁸MBBS, Kabul Medical University, Kabul, Afghanistan.
*Corresponding author: Hira Riaz, MBBS, Kabul Medical University, Kabul, Afghanistan.
Received: April 24, 2026 | Accepted: April 04, 2026 | Published: May 25, 2026
Citation: Aderinsola Wale-Oyedele, Jabeen A, Siddiqui S, Pooja L, Khalid A. (2026) “Therapeutic Efficacy of Mirikizumab, a Novel IL-23p19 Monoclonal Antibody, in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis”. Gastroenterology and Hepatology Research, 6(2); DOI: 10.61148/2836-2888/GHR/066.
Copyright: © 2026. Hira Riaz. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited., provided the original work is properly cited.
Interleukin-23 (IL-23) is a critical cytokine involved in intestinal inflammation and plays a central role in the pathogenesis of inflammatory bowel disease (IBD). Mirikizumab (Omvoh), a humanized IgG4 monoclonal antibody targeting the p19 subunit of IL-23, has been developed for the treatment of ulcerative colitis (UC) and Crohn’s disease (CD). This meta-analysis aimed to assess the efficacy and safety of Mirikizumab in patients with IBD. A comprehensive literature search was conducted in PubMed, the Cochrane Library, and ClinicalTrials.gov up to May 1, 2025. Four randomized controlled trials comparing Mirikizumab to placebo in IBD populations were included. Data analysis was performed using RStudio and RevMan 5.4 under a random-effects model. The pooled results demonstrated that Mirikizumab significantly improved rates of endoscopic, clinical, symptomatic, and histologic remission compared to placebo. Additional benefits included greater improvements in IBD questionnaire scores, reductions in fecal calprotectin levels, and decreased bowel urgency. The incidence of serious adverse events was significantly lower in the Mirikizumab group, with no differences observed in mortality. These findings support Mirikizumab as a safe and effective treatment for UC and CD, with more pronounced benefits in CD. Nevertheless, further large-scale trials, particularly in CD, are warranted to confirm these outcomes.
Mirikizumab, Ulcerative Colitis, Crohns disease, IBD
IBD, or inflammatory bowel disease, has been a persistently rising global health concern[1]. It presents in two distinct types Crohons disease [CD] and Ulcerative Colitis [UC]. CD is distinct from UC as it can cause transmural inflammation of any part of the gastrointestinal tract (mostly the terminal ileum or the perianal area) and is associated with complications such as abscesses, fistulas and strictures whereas UC is characterized by a mucosal inflammation mostly associated with the colon [2].
The first class of biological drugs authorised for the treatment of individuals with IBD were factor-α inhibitors (TNFis), which include infliximab and adalimumab. These agents are very effective against the disease's luminal and extraintestinal symptoms [3][4][5].However, many patients treated with anti-TNFα drugs, including primary and secondary nonresponders, experience therapeutic failure.[6] Anti-TNF-α medications are also linked to uncommon but severe side effects, such as paradoxical autoimmune reactions, significant infection, and a slight but elevated risk of cancer [7]. Other innovative anti-inflammatory treatments that target inflammatory pathways have been developed with greater safety in this context. These include leukocyte trafficking (anti-integrin medicines e.g. Vedolizumab and Ertolizumab etc.) and cellular signalling (e.g., anti-interleukin (IL) 12/23 drugs (e.g. ustekinumab and mirikizumab etc.) and Janus kinase (JAK) inhibitors (e.g.Tofacitinib and Rigotinib etc.)[8][9] [10].
A member of the IL12 family of cytokines, IL23 is made up of two parts: the p40 subunit, which IL12 shares, and the p19 subunit, which is present in IL23 but absent from IL12. IL23 is essential for the upkeep and proliferation of T helper 17 cells as well as the activation of numerous innate immune cells, both of which are crucial for the pathophysiology of chronic inflammatory diseases like CD and UC[11-13]. Mirikizumab (LY3074828) is a humanised immunoglobulin G4 (IgG4)-variant monoclonal antibody currently undergoing phase 3 testing for psoriasis, ulcerative colitis, and CD. It binds selectively to the p19 subunit of IL23 and has demonstrated efficacy in treating these conditions[14-15].
A number of systematic reviews have synthesized data for various biological agents, including mirikizumab, in IBD [16][17]; However, these evaluations did not assess the relative dosages of mirikizumab at which the medication is most effective. Thus, as far as we are aware, we have carried out the first systematic review and meta-analysis to thoroughly assess the relative efficacy of mirikizumab at different dosages for the treatment of moderate to severe CD or UC.
Methods:
The current systematic review was performed using a pre-established protocol in OSF (Open Science Forum).
Data Sources and Search Strategy
For this meta-analysis, We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines to ensure transparency and rigor in reporting our review. The PRISMA framework provides a standardized checklist and flow diagram that guide authors in documenting the rationale, methodology, results, and interpretation of systematic reviews. By adhering to PRISMA, we enhanced the reproducibility of our methods, minimized reporting bias, and improved the clarity and completeness of our findings. PRISMA checklist can be found attached with the manuscript.
We conducted systematic electronic searches of the Cochrane Library (which includes the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects, and the Health Technology Assessment database), PubMed, and Clinicaltrial.gov. Medical subject headings and free-text phrases were used to create search techniques. All searches were conducted from the beginning to May 1, 2025. Search strategy is given in Table 4.
Table 4. Search Strategy
|
Database |
Search Strategy |
Filters / Limits |
Date of Last Search |
|
PubMed/MEDLINE |
("Mirikizumab"[All Fields] OR "LY3074828"[All Fields] OR "Omvoh"[All Fields]) AND ("Inflammatory Bowel Disease"[MeSH Terms] OR "IBD"[All Fields] OR "Ulcerative Colitis"[MeSH Terms] OR "UC"[All Fields] OR "Crohn Disease"[MeSH Terms] OR "Crohn’s Disease"[All Fields] OR "CD"[All Fields]) AND ("Randomized Controlled Trial"[Publication Type] OR "RCT"[All Fields] OR "clinical trial"[All Fields]) |
Humans, English language |
May 1, 2025 |
|
Cochrane Library (CENTRAL, Cochrane Reviews, DARE, HTA) |
("Mirikizumab" OR "LY3074828" OR "Omvoh") in Title Abstract Keyword AND ("Inflammatory Bowel Disease" OR "IBD" OR "Ulcerative Colitis" OR "UC" OR "Crohn Disease" OR "CD") |
Trials only, English language |
May 1, 2025 |
|
Condition/Disease: Inflammatory Bowel Disease, Ulcerative Colitis, Crohn’s Disease; Intervention: Mirikizumab OR LY3074828 OR Omvoh |
Completed, Recruiting, Active, Not Yet Recruiting |
May 1, 2025 |
Study design
Clinical trials were included for the analysis. We used the PICO (Patient/Population, Intervention, Comparison and Outcomes) framework to establish the following inclusion criteria for all relevant original articles.
Participants:
Participants with a diagnosis of ulcerative colitis for at least 3 months before the planned start date for the study medication were included. Studies that involved participants with recent treatment of Ulcerative colitis like cyclosporine or thalidomide within 30 days of screening; corticosteroid enemas, corticosteroid suppositories, or topical treatment with 5-aminosalicylic acid within 1 week of screening endoscopy were excluded. Review articles, systematic reviews and meta-analyses, guidelines, conference papers which were not written in the English language as well as animal studies were also excluded.
Interventions:
We included trials which evaluated Mirikizumab on various dosing regimens. These were given to the patients as Placebo, 50mg Mirikizumab, 200 mg Mirikizumab, 300 mg Mirikizumab, 600 mg Mirikizumab and 1000 mg Mirikizumab. Dosage regimens were necessary to match the approved medication’s summary of product characteristics (SmPC) or the SmPC of the original product for biosimilars that have not been approved.
Comparision:
The comparator arm consisted of patients receiving placebo under identical conditions, consistent with the design of placebo-controlled induction studies in ulcerative colitis. The use of a placebo control allowed for unbiased assessment of efficacy and safety outcomes and served as a reference point for calculating treatment effect sizes. In cases where ethical considerations required rescue therapy, predefined criteria for crossover or withdrawal were applied.
Outcomes:
A blinded central reader graded the results of endoscopies conducted at study weeks 24 (after extended induction dose) and 52 (following extended induction dosing) to offer an unbiased assessment of the intestinal mucosa's appearance. At trial weeks 24 and 52weeks, we noted the propotion of patients entering the following endpoints : clinical remission, clinical response, endoscopic remission, endoscopic response, Histologic remission, symptomatic remission, fecal calprotectin levels, bowel urgency, Inflammatory Bowel Disease Questionnaire (IBDQ) scores. In addition, number of patients experiencing any adverse events were also noted in this time duration.
Clinical Remission
Clinical remission was defined using components of the Mayo Clinic Score.(34) Patients were considered to be in clinical remission if they achieved a rectal bleeding subscore of 0 and a stool frequency subscore of 0 or 1, with the additional requirement of at least a 1-point decrease in the stool frequency subscore from baseline.
Clinical Response
Clinical response was defined as a decrease of at least 2 points and 35% from baseline in the total 9-point partial Mayo subscore (part of Mayo clinic score), which includes stool frequency, rectal bleeding, and endoscopic appearance. In addition, patients had to demonstrate either a decrease in the rectal bleeding subscore by ≥1 point or achieve a rectal bleeding subscore of 0 or 1.
Symptomatic Remission
Symptomatic remission was defined as a stool frequency subscore of 0 or 1 combined with a rectal bleeding subscore of 0, indicating resolution of patient-reported symptoms.
Endoscopic Remission
Endoscopic remission was defined as a Mayo endoscopic subscore (Part of Mayo Clinic score) of 0, indicating the absence of visible mucosal inflammation on endoscopy.
Histologic Remission
Histologic remission was defined as the absence of active inflammation on histopathology, specifically requiring a Geboes histologic score(35) of 0 for neutrophils in the lamina propria, neutrophils in the epithelium, and the presence of erosions or ulceration.
Change from Baseline in IBDQ:
The Inflammatory Bowel Disease Questionnaire (IBDQ) is a 32-item, patient-reported instrument that evaluates health-related quality of life in individuals with inflammatory bowel disease. It encompasses four domains: bowel symptoms, systemic symptoms, emotional function, and social function. Each item is rated on a 7-point Likert scale (1 = very severe problem; 7 = no problem at all), with total scores ranging from 32 to 224. A higher score reflects better quality of life. In this study, the change from baseline in IBDQ was calculated as the difference between baseline and post-treatment scores at defined time points during the trial.
Change from Baseline in Bowel Urgency (Symptomatic Score):
Bowel urgency was incorporated into the broader symptomatic score, which combined rectal bleeding and stool frequency subscores. Symptomatic remission was defined as a stool frequency subscore of 0 or 1 and a rectal bleeding subscore of 0. Changes from baseline were calculated by subtracting the week 24 or 52 symptom score from the baseline score. This provided a continuous measure of symptomatic improvement or deterioration over time.
Change from Baseline in Fecal Calprotectin (fCLP):
Fecal calprotectin levels were measured in patient-collected stool samples using an enzyme immunoassay (Bühlmann Laboratories). The change from baseline was calculated by comparing pre-treatment fCLP values to post-treatment values at designated follow-up weeks. Negative values indicated a reduction in intestinal inflammation, consistent with therapeutic response. The results were expressed in mg/kg of stool and presented as median changes with associated ranges and standard deviations.
Adverse Events:
Adverse events (AEs) were categorized and coded using the Medical Dictionary for Regulatory Activities (MedDRA) versions 19–21. A treatment-emergent adverse event (TEAE) was defined as any event that first occurred or worsened in severity following administration of the study drug. AEs were classified by system organ class and preferred term, and were evaluated for severity and relationship to the investigational product. Both serious and non-serious adverse events were reported separately across study phases.
Study selection
Two independent authors extracted data using a standardized Excel spreadsheet and resolved disagreements following a discussion with a third author . The following data were abstracted:
1. Study characteristics including author, study type, period, setting.
2. Outcomes of clinical remission, clinical response, endoscopic remission, endoscopic response, symptomatic remission and histologic remission.
Data extraction and management
Up until May 2025, a thorough literature search was conducted using PubMed, Cochrane Library and ClinicalTrials.gov, with an emphasis on research assessing the safety and efficacy of mirikizumab. For both the dose-wise and overall mirikizumab and placebo groups, we retrieved data on endoscopic, clinical, and symptomatic remission and response, as well as related side events. The meta-analysis was carried out using RevMan 5.4 to compute risk ratios (RR) and mean differences (MDs) under a random-effects model, and Rstudio to pool outcome data under the common effects (CE) model.
Data synthesis and measures of treatment effect
Two independent analyses were conducted for patients with CD and UC, respectively, pooling data for each predetermined outcome of interest. A random-effects meta-analysis was used to aggregate the total proportions from each study after the results, which were presented as proportions (n: event; N: population), were examined. Studies were only included in a meta-analysis if they were judged to share similar features (e.g., study populations and treatments). Each meta-analysis's trials were evaluated for heterogeneity using the I2 statistic. Every statistical analysis was carried out using R (4.0.2).
Risk of bias assessment:
The risk of bias in the included randomized controlled trials was independently assessed using the Cochrane Risk of Bias 2.0 (RoB 2) tool, which is the recommended instrument for evaluating bias in randomized trials in systematic reviews and meta-analyses(32) . RoB 2 evaluates five specific domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result(33) . Each domain is assessed through a series of signaling questions to guide judgments, which are categorized as “low risk,” “some concerns,” or “high risk” of bias. An overall risk of bias judgment for each study was then derived based on these domain-level assessments following the tool’s algorithm. The assessments were performed independently by two reviewers, with disagreements resolved by discussion or consultation with a third reviewer. The results of the risk of bias assessment were incorporated into the interpretation of the meta-analysis findings to evaluate the certainty and robustness of the evidence. Visual summaries of the risk of bias judgments were prepared using standard traffic-light plots to facilitate transparent reporting. (Supplimentary figure 21).
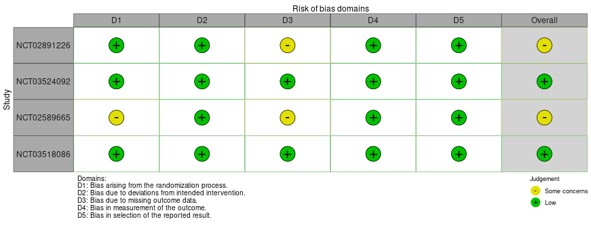
Supplementary Figure 21. Traffic Light Plot Showing Risk of Bias Assessments of Included Mirikizumab Randomized Controlled Trials Using the Cochrane RoB 2.0 Tool.
To evaluate the potential for publication bias, we conducted visual inspection of funnel plots for asymmetry, which may indicate small-study effects or selective reporting. For each primary outcome with ten or more included studies, we generated funnel plots plotting effect size against standard error. In addition, we performed Egger’s regression test to statistically assess the presence of asymmetry, with a p-value of <0.10 considered suggestive of significant publication bias.
Results:
Search strategy and study selection:
As shown in the PRISMA flow chart (Supplementary Figure 10), a total of 137412 articles were retrieved from three databases. Of those articles, 152 were excluded for duplication. The remaining 137260 studies were screened for eligibility. Title and abstract screening resulted in 137260 potentially eligible studies. Full-text evaluation resulted in the inclusion of four studies that included 2146 IBD patients receiving mirikizumab. The four studies included in the meta-analysis are all randomized controlled trials. The inclusion criteria for the studies included in the meta-analysis are that the weight should be more than 10 kg and must be a diagnosed case of IBD for at least 3 months prior to starting therapy, must have moderate to severe IBD as defined by Modified Mayo Score (MMS) and loss of response or intolerance to corticosteroids, immunomodulators, Janus kinase inhibitors, or other biologic therapies. The exclusion criteria for the studies included in the meta-analysis were the presence of indeterminate colitis , ulcerative proctitis primary sclerosing cholangitis, having undergone surgery to remove any or all of the colon, current evidence of toxic megacolon, taking cyclosporine or thalidomide within 30 days of screening, taking corticosteroid or topical 5-aminosalicylic acid 1 week before screening, and inadequate response to antiILp40 or exposure to antiIL-23p19 antibodies.
Study Characteristics:
This systematic review and meta-analysis included four randomized controlled trials (RCTs) comprising 2,146 patients with moderate-to-severe ulcerative colitis (UC) or Crohn’s disease (CD). Eligible studies compared mirikizumab (doses: 50–1000 mg) against placebo, with outcomes assessed at 12–52 weeks. Participants were adults (weight >10 kg) with confirmed IBD for ≥3 months, inadequate response/intolerance to prior therapies (corticosteroids, immunomodulators, biologics, or JAK inhibitors), and objective evidence of active inflammation (Modified Mayo Score [MMS] or Crohn’s Disease Activity Index [CDAI]). Exclusion criteria included indeterminate colitis, recent surgery, or prior anti-IL-23p19 exposure. Primary endpoints were endoscopic, clinical, symptomatic, and histologic remission; secondary outcomes included IBD Questionnaire (IBDQ) scores, fecal calprotectin reduction, and bowel urgency improvement. All 4 studies are summarized in Table 2.
Table 2: Study Characteristics. IV; Intravenous, SC; subcutaneous, CD; Crohn's disease, UD; Ulcerative colitis, AE; Adverse effects, SAE; Severe adverse effects, SF; Stool frequency, Q4W; Every 4 weeks, RCT; Randomized control trial, RB; Rectal bleeding, SES-CD; Simple endoscopic score for crohn’s disease.
|
STUDY (YEAR) |
DESIGN |
POPULATION |
INTERVENTION |
COMPARATOR |
PRIMARY OUTCOME |
KEY RESULTS |
SAFETY FINDINGS |
|
Sands et al. (2022) |
Phase 2 RCT |
191 patients with moderate-to-severe Crohn’s disease (CD) |
IV Mirikizumab (200 mg, 600 mg, 1000 mg Q4W) for 12 weeks, then SC (300 mg Q4W) or continued IV for maintenance |
Placebo |
Endoscopic response (50% reduction in SES-CD) at Week 12 |
- Week 12: Endoscopic response rates: 25.8% (200 mg), 37.5% (600 mg), 43.8% (1000 mg) vs. 10.9% (placebo; all P<0.1). - Week 52: 58.5% (IV) and 58.7% (SC) maintained response. |
AE rates similar to placebo. SAEs higher in non-responders. No dose-related safety concerns. |
|
Sandborn et al. (2022) |
Phase 2 RCT (extension |
249 patients with moderate-to-severe ulcerative colitis (UC) |
IV Mirikizumab (50–600 mg Q4W) for 12 weeks; non-responders received extended IV (600/1000 mg Q4W) for 12 weeks |
Placebo |
Clinical response (Mayo score reduction ≥2 points and ≥35% + rectal bleeding improvement) at Week 24 |
- Extended induction: 50% (600 mg) and 43.8% (1000 mg) achieved clinical response. - Week 52: 65.8% maintained response; 26.3% achieved remission. |
No new safety signals. SAEs are rare (e.g., UC worsening, infections). Rectal cancer reported in 2 patients. |
|
LUCENT-1 (Sandborn et al., 2023) |
Phase 3 RCT (Induction) |
1,281 adults with moderate-to-severe UC |
IV Mirikizumab (300 mg at Weeks 0, 4, 8) |
Placebo |
Clinical remission at Week 12 (Mayo score: stool frequency [SF] ≤1, rectal bleeding [RB] =0, endoscopic subscore ≤1) |
- Week 12: ・ Clinical remission: 24.2% (Mirikizumab) vs. 13.3% (placebo; P<0.001). ・ Endoscopic remission: 37.5% vs. 19.8% (P<0.001). ・ Symptomatic remission: 45.9% vs. 28.1% (P<0.001). |
AE rates similar to placebo. - Most common AEs: nasopharyngitis, headache, arthralgia. - No new safety signals. |
|
LUCENT-2 (D’Haens et al., 2023) |
Phase 3 RCT (Maintenance) |
544 responders from LUCENT-1 |
SC Mirikizumab (200 mg Q4W) for 40 weeks |
Placebo |
Clinical remission at Week 40 (maintained from Week 12) |
- Week 40: ・ Clinical remission: 49.9% (Mirikizumab) vs. 25.1% (placebo; P<0.001). ・ Endoscopic remission: 57.7% vs. 30.7% (P<0.001). ・ Durable remission (Weeks 12–40): 39.5% vs. 17.3% (P<0.001). |
- Low discontinuation rates due to AEs (3.1% Mirikizumab vs. 3.9% placebo). - No malignancy or opportunistic infections. |
Risk of bias assessment:
The risk of bias assessment using the Cochrane RoB 2 tool indicated that the majority of included randomized controlled trials demonstrated a low risk of bias across most domains. [32] Specifically, all four studies showed low risk in the domains of deviations from intended interventions, outcome measurement, and selective reporting. However, some concerns were identified in the domain of missing outcome data for two studies, primarily due to incomplete information on participant dropouts and handling of missing data. One study exhibited some concerns regarding the randomization process due to limited details on allocation concealment. No studies were judged to have a high risk of bias overall. These findings suggest that while the included trials generally maintain methodological rigor, caution is warranted when interpreting results affected by incomplete outcome data. The detailed risk of bias judgments for each domain and study are summarized in Table 3. The risk of bias is illustrated in Supplimentary figure 20, as traffic lights plot.
Funnel plots of publication bias are shown in Supplimentary figure 12-20.
Table 3. Risk of Bias Assessment of Included Mirikizumab Randomized Controlled Trials Using the Cochrane RoB 2.0 Tool
|
Study (NCT ID) |
Randomization |
Allocation Concealment |
Blinding |
Incomplete Data |
Selective Reporting |
Other Bias |
Overall Risk |
|
NCT02891226 |
Low |
Low |
Low |
Some concerns |
Low |
Low |
Some concerns |
|
NCT03524092 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
|
NCT02589665 |
Low |
Low |
Low |
Some concerns |
Low |
Low |
Some concerns |
|
NCT03518086 |
Low |
Low |
Low |
Low |
Low |
Low |
Low |
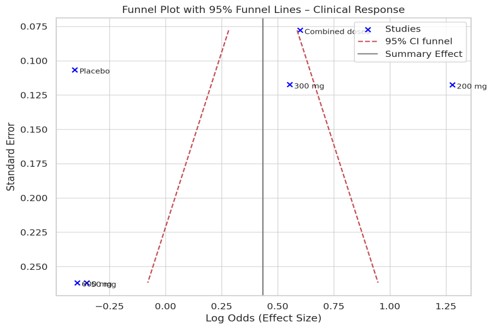
Supplementary Figure 14. Funnel plot assessing publication bias for Clinical response.

Supplementary Figure 15. Funnel plot assessing publication bias for Clinical remission.
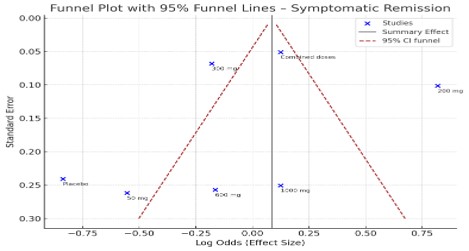
Supplimentary figure 16. Funnel plot showing publication bias in Symptomatic remission.
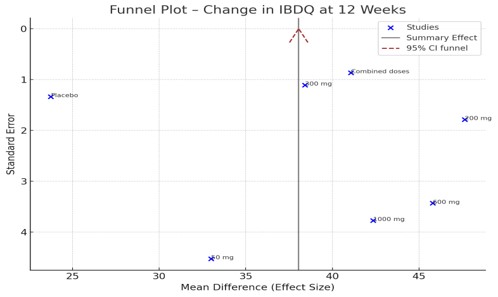
Supplimentary figure 17. Funnel plot showing publication bias in change in IBDQ at 12 weeks
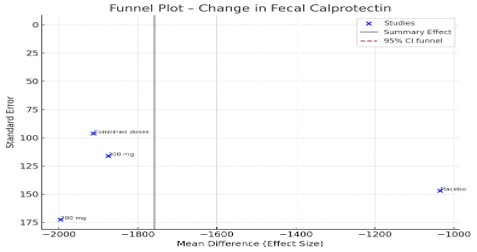
Supplimentary figure 18. Funnel plot showing publication bias in fecal calprotectin outcome

Supplimentary figure 19. Funnel plot showing publication bias in Bowel urgency outcome
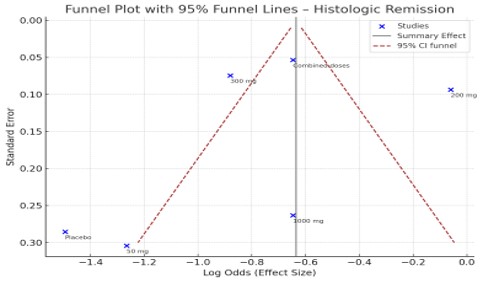
Supplimentary figure 20. Funnel plot showing publication bias in change in Histologic remission.
Main results:
Different doses of mirikizumab were administered and compared to placebo. These doses were 50 mg, 200 mg, 300 mg, 600 mg, and 1000 mg. The effects of all the different doses of mirikizumab were also added together and compared to placebo. The outcome measures included endoscopic response, endoscopic remission, clinical response, clinical remission, Symptomatic remission, Histologic remission, change from baseline on IBDQ at 12 weeks, change from baseline in fecal calprotectin, change from baseline in bowel urgency based on urgency NRS.
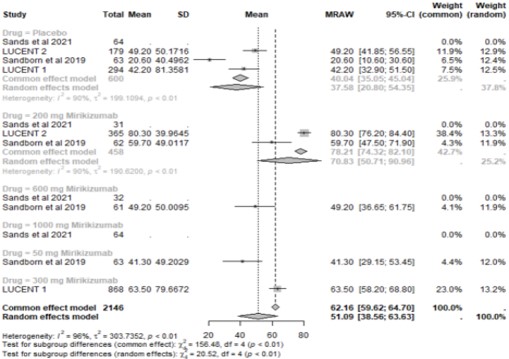
Endoscopic response:
The endoscopic response for all the doses of mirikizumab was better than that of placebo, except for the 50 mg dose of mirikizumab, which was not calculated due to a lack of data. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 67.32 [62.99; 71.65] (95%CI). The response for 300 mg was 55.40 [52.10; 58.70] (95%CI), 600 mg was 37.5 [23.40; 51.60] (95%CI), and 1000 mg was 43.8 [33.65; 53.95] (95%CI), and the pooled proportion of the endoscopic response of all the different doses together was 58.11 [55.60; 60.61] (95%CI). (Supplementary Figure 1).
Supplementary Figure 1: Forest plot showing endoscopic response in placebo group and respective doses of mirikizumab group.
Endoscopic remission:
The endoscopic remission for all the doses of mirikizumab was better than that of placebo, except 50 mg and 600 mg, which were less than that of placebo. The best response was observed in participants who were administered 300 mg mirikizumab with a pooled proportion of 36.30 [31.00; 41.60]. The pooled proportion for 50 mg was 3.20 [-0.55; 6.95] (95%CI), for 200 mg it was 20.48 [17.71; 23.26] (95%CI), for 600 mg it was 2.29 [-0.05; 4.63] (95%CI), and for 1000 mg it was 20.30 [12.00; 28.60] (95%CI), and the pooled proportion of all the different doses together was 11.28 [9.76; 12.80] (95%CI). (Supplementary Figure 2).
Supplementary Figure 2: Forest plot showing Endoscopic Remission in placebo group and respective doses of mirikizumab group.
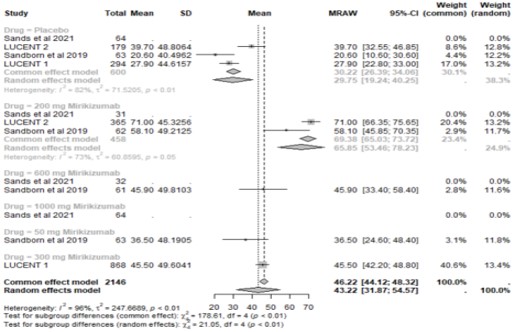
Clinical response:
The Clinical response for all the doses of mirikizumab was better than that of placebo, except 1000 mg which could not be calculated because of insufficient data. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 78.21 [74.32; 82.10] (95%CI). the clinical response for 50 mg was 41.3 [29.15; 53.45] (95%CI) for 300 mg was 63.50 [58.20; 68.80 (95%CI), 600mg was 49.20 [36.65; 61.75] (95%CI) and pooled proportion of all the different doses together was 29.65 [26.77; 32.54] (95%CI). (Supplementary Figure 3).
Supplementary Figure 3: Forest plot showing Clinical Response in placebo group and respective doses of mirikizumab group.
Clinical Remission:
The Clinical remission for all the doses of mirikizumab was better than that of placebo, except 1000 mg which could not be calculated because of insufficient data. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 44.52 [39.91; 49.14] (95%CI). the clinical remission for 50 mg was 15.9 [6.85; 24.95] (95%CI) , for 300 mg was 24.20 [19.50; 28.90] (95%CI), 600mg was 11.50 [3.50; 19.50] (95%CI) and pooled proportion of all the different doses together was 29.65 [26.77; 32.54] (95%CI). (Supplementary Figure 4).
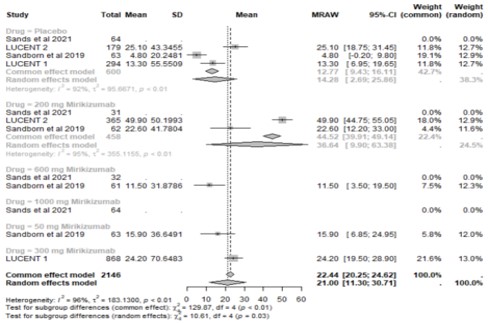
Supplementary Figure 4: Forest plot showing Clinical Remission in placebo group and respective doses of mirikizumab group.
The Symptomatic remission for all the doses of mirikizumab was better than that of placebo, except 1000 mg which could not be calculated because of insufficient data. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 69.38 [65.03; 73.72] (95%CI). The Symptomatic remission for 50 mg was 36.5 [24.60; 48.40] (95%CI) the pooled proportion for 300 mg was 45.5 [42.20; 48.80] (95%CI), 600mg was 45.90 [33.40; 58.40] (95%CI) and pooled proportion of all the different doses together was 53.10 [50.59; 55.61] (95%CI). (Supplementary Figure 5).
Supplementary Figure 5: Forest plot showing Symptomatic remission in placebo group and respective doses of mirikizumab group.
Histologic remission:
The histological remission for 200mg and 300 of mirikizumab were better than that of placebo. The
histological remission at 50mg, 600mg and 100 mg could not be calculated because of lack of sufficient data available. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 48.50 [43.40; 53.60] (95%CI). The histological remission for 300mg was 29.30 [26.25; 32.35] (95%CI). The pooled proportion for all the different doses together was calculated to be 34.36 [31.74; 36.98] (95%CI). (Supplementary Figure 6).
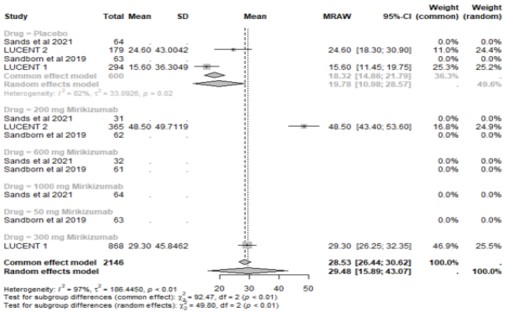
Supplementary Figure 6: Forest plot showing Histologic remission in placebo group and respective doses of mirikizumab group.
Change from baseline on IBDQ:
The Change from baseline on IBDQ at 12 weeks for all the doses of mirikizumab was better than that of placebo. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of 47.63 [44.13; 51.13].
The Change from baseline on IBDQ at 12 weeks for 50 mg was 33.00 [24.14; 41.86], for 300 mg was 38.42 [36.25; 40.59], 600mg was 45.79 [39.06; 52.51] and pooled proportion of all the different doses together was 53.10 [50.59; 55.61] (95%CI). (Supplementary Figure 7).
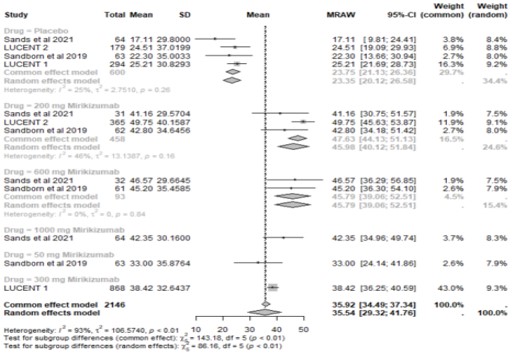
Supplementary Figure 7: Forest plot showing Change from baseline on IBDQ at 12 weeks in placebo group and respective doses of mirikizumab group.
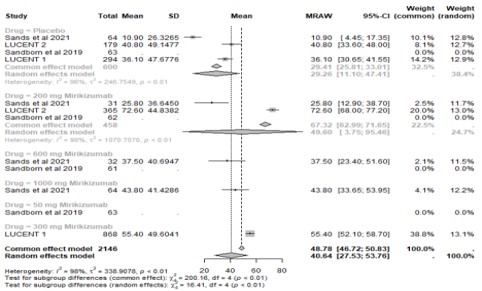
Change from baseline in fecal calprotectin:
The Change from baseline in fecal calprotectin for 200mg and 300 of mirikizumab was better than that of placebo. The histological remission at 50mg, 600mg and 100 mg could not be calculated because of lack of sufficient data available. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of -1995.47 [-2333.45; -1657.49] (95% CI). The pooled proportion for 300mg was -1875.29 [-2102.92; -1647.66] (95%CI). The pooled proportion for all the different doses together was calculated to be -1912.79 [-2101.59; -1723.99] (95%CI.) (Supplementary Figure 8).
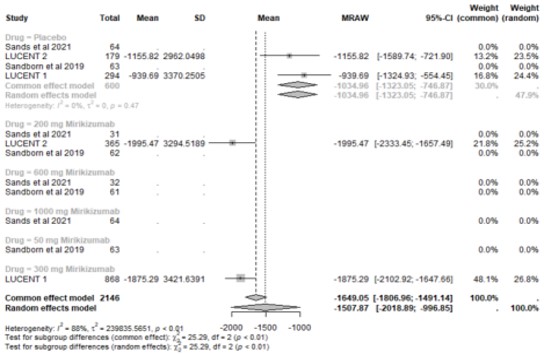
Supplementary Figure 8: Forest plot showing Change from baseline in fecal calprotectin in placebo group and respective doses of mirikizumab group.
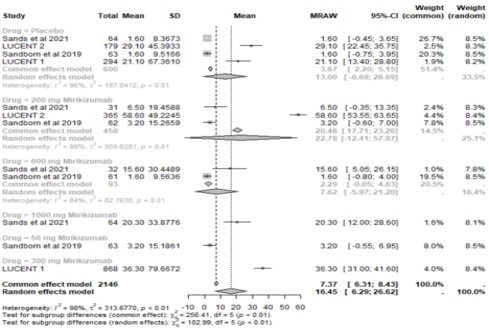
Change from baseline in bowel urgency:
The Change from baseline in bowel urgency based on urgency NRS for 200mg and 300 of mirikizumab was better than that of placebo. The histological remission at 50mg, 600mg and 100 mg could not be calculated because of lack of sufficient data available. The best response was observed in participants who were administered 200 mg mirikizumab with a pooled proportion of -3.8 [-4.07; -3.53] (95% CI). The pooled proportion for 300mg was - 2.59 [-2.75; -2.43] (95%CI). The pooled proportion for all the different doses together was calculated to be -2.91 [-3.05; -2.77(95%CI). (Supplementary Figure 9).
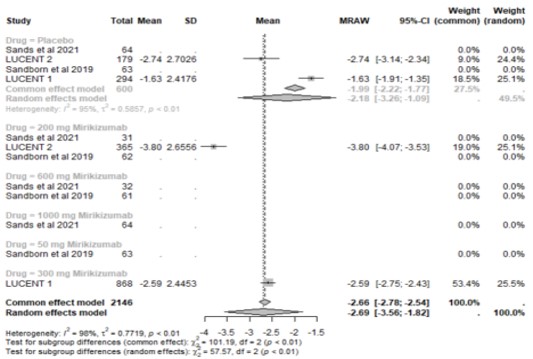
Supplementary Figure 9: Forest plot showing Change from baseline in bowel urgency based on urgency NRS in placebo group and respective doses of mirikizumab group.
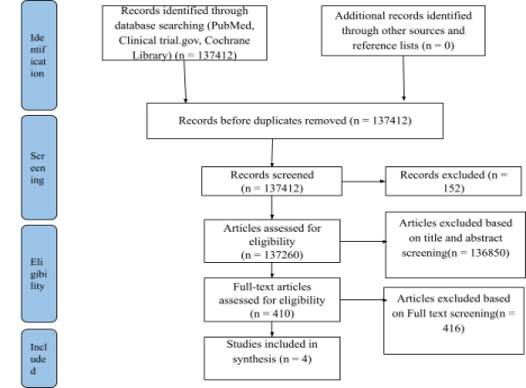
Supplementary Figure 10: Prisma Flow Chart
Adverse events:
Results also depicted that the use of mirikizumab reduced the overall risk of serious adverse events (RR 0.44, 95% CI: 0.28-0.72, p=0.0008).
All the results are summarised in the barchart provided in Supplementary Figure 11, and the forest plot data is summarised in Table 1.
Table 1. Summary of the results. N/A; Data not available
|
Outcomes |
Placebo |
50 mg mirikizumab |
200 mg mirikizumab |
300 mg mirikizumab |
600 mg mirikizumab |
1000 mg mirikizumab |
Combined mirikizumab doses effect |
||||||||||||||
|
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
n |
pooled proportion (95%Cl) |
I2 value (%) |
|
|
Endoscopic response (%) |
600 |
29.41 [25.81; 33.01] |
96 |
NA |
NA |
NA |
458 |
67.32 [62.99; 71.65] |
98 |
868 |
55.40 [52.10; 58.70] |
0 |
32 |
37.5 [23.40; 51.60] |
0 |
64 |
43.8 [33.65; 53.95] |
0 |
1546 |
58.11 [55.60; 60.61] |
95 |
|
Endoscopic remission (%) |
600 |
3.67 [2.20; 5.15] |
96 |
63 |
3.20 [-0.55; 6.95] |
0 |
458 |
20.48 [17.71; 23.26] |
99 |
868 |
36.30 [31.00; 41.60] |
0 |
93 |
2.29 [-0.05; 4.63] |
84 |
64
|
20.30 [12.00; 28.60] |
0 |
1546 |
11.28 [9.76; 12.80] |
99 |
|
Clinical response (%) |
600 |
40.04 [35.05; 45.04] |
90 |
63 |
41.3 [29.15; 53.45] |
0 |
458 |
78.21 [74.32; 82.10] |
90 |
868 |
63.50 [58.20; 68.80] |
0 |
61 |
49.20 [36.65; 61.75] |
0 |
NA |
NA |
NA |
1546 |
29.65 [26.77; 32.54] |
96 |
|
Clinical remission (%) |
600 |
12.77 [9.43; 16.11] |
92 |
63 |
15.9 [6.85; 24.95] |
0 |
458 |
44.52 [39.91; 49.14] |
95 |
868 |
24.20 [19.50; 28.90] |
0 |
61 |
11.50 [3.50; 19.50] |
0 |
NA |
NA |
NA |
1546 |
29.65 [26.77; 32.54] |
96 |
|
Symptomatic remission (%) |
600 |
30.22 [26.39; 34.06] |
82 |
63 |
36.5 [24.60; 48.40] |
0 |
458 |
69.38 [65.03; 73.72] |
73 |
868 |
45.5 [42.20; 48.80] |
0 |
61 |
45.90 [33.40; 58.40] |
0 |
NA |
NA |
NA |
1546 |
53.10 [50.59; 55.61]
|
95 |
|
Histologic remission (%) |
600 |
18.32 [14.86; 21.79] |
82 |
NA |
NA |
NA |
365 |
48.50 [43.40; 53.60] |
0 |
868 |
29.30 [26.25; 32.35] |
0 |
NA |
NA |
NA |
NA |
NA |
NA |
1546 |
34.36 [31.74; 36.98] |
98 |
|
Change from baseline on IBDQ at 12 week |
600 |
23.75 [21.13; 26.36] |
25 |
63 |
33.00 [24.14; 41.86] |
0 |
458 |
47.63 [44.13; 51.13] |
46 |
868 |
38.42 [36.25; 40.59] |
0 |
93 |
45.79 [39.06; 52.51] |
0 |
64 |
42.35 [34.96; 49.74] |
0 |
1546 |
41.07 [39.37; 42.76] |
75 |
|
Change from baseline in fecal calprotectin |
600 |
-1034.96 [-1323.05; -746.87] |
0 |
NA |
NA |
NA |
365 |
-1995.47 [-2333.45; -1657.49] |
0 |
868 |
-1875.29 [-2102.92; -1647.66] |
0 |
NA |
NA |
NA |
NA |
NA |
NA |
1546 |
-1912.79 [-2101.59; -1723.99] |
0 |
|
Change from baseline in bowl urgency based on urgency NRS |
600 |
-1.99 [-2.22; -1.77] |
0 |
NA |
NA |
NA |
365 |
-3.8 [-4.07; -3.53] |
0 |
868 |
-2.59 [-2.75; -2.43] |
0 |
NA |
NA |
NA |
NA |
NA |
NA |
1546 |
-2.91 [-3.05; -2.77] |
98 |
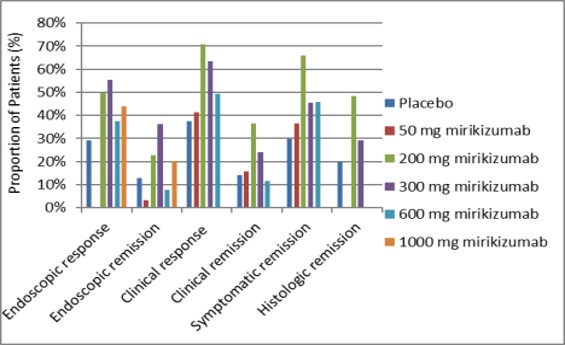
Supplementary Figure 11: Bar chart showing direct comparison of placebo versus various Mirikizumab dosing on endoscopic, clinical, symptomatic, and histologic remission and response.
Discussion:
It has been more than 200 years since the disease ‘’Inflammatory bowel disease’’ was first described [18]. Over the years several different medications and treatment options have been used in the management and treatment of this disease with varying degrees of success but no treatment modality has so far been able to manage the disease effectively for a long time without causing significant side effects [19]. This meta-analysis explores the efficacy of a drug called ‘’mirikizumab’’ in the management of inflammatory bowel disease. Mirikizumab is a monoclonal antibody which works against IL-23, an inflammatory marker, by attaching to the p19 subunit of IL-23 [20]. It therefore reduces inflammation by blocking the binding of IL-23 with its receptor [21]. It has already been approved in some countries as an acceptable treatment modality for ulcerative colitis [22,23] . As the data on the drug has increased thanks to a number of clinical trials conducted recently it is very important to summarize all the information and data gathered through these studies to determine with a degree of confidence the efficacy of the drug in the management of inflammatory bowel disease.
Four clinical trials were included in the study which studied the efficacy of mirikizumab against inflammatory bowel disease. The results showed that mirikizumab significantly improved patients suffering from inflammatory bowel disease especially when the drug dose was kept at 200mg. At 200 mg a significant clinical response was observed in 78.21% of the participants. This is much higher than what is achieved by other medications. For example, Aminosalicyclates which have been used historically for the management of ulcerative colitis and Crohn's disease have a much lower remission and clinical response rate as compared to mirikizumab[24,25]. Another drug which has been used very frequently in management of inflammatory bowel disease is infliximab which is an anti-tumor necrosis factor (Anti TNF) antibody [26]. although the overall remission rates with infliximab have been very high with studies reporting a clinical response in more than 80% of the patients[26]. But even this drug has not been able to conveniently manage patients over the long run as almost 50% of the patients lose response to the drug over time [26]. A number of other drugs have also been used for the treatment of inflammatory bowel disease which includes corticosteroids, azathioprine, 6-mercaptopurine etc. [27]. But most are either not very effective in treating or managing the condition or have a significant number of side effects which limits their long-term use or in some cases both [28,29]. Thus, the development of a new alternative in the shape of mirikizumab would be very helpful in the long term in the treatment and management of inflammatory bowel disease. Another meta analysis also reproduced similar results earlier in which mirikizumab was found to be superior to placebo in both clinical response and remission[30].
The conducted study does carry a number of limitations. Firstly, the number of studies included in the meta-analysis is limited to four thus further research and clinical trials need to be done before a consensus can be reached about the efficacy of the medication. Another thing to consider is that this meta-analysis only compares the use of mirikizumab mono-therapy against placebo and does not compare the effectiveness of mirikizumab against other treatment modalities like infliximab so as to determine with significance the efficacy of the medication against other accepted treatment modalities. In addition, inflammatory bowel disease is now mostly treated by a combination of different medications [31]. Thus, further clinical trials comparing efficacy of mirikizumab against such combination therapies would also need to be performed. Within the studies included in the meta – analysis a high degree of heterogeneity is also present which shows that there exists marked variance between different studies included. Furthermore, the side effects profile of the drug has not been the focus of the meta-analysis. Thus, a lot more research is required before mirikizumab can be considered as a therapy for inflammatory bowel disease.
Conclusion:
This systematic review and meta-analysis demonstrate that mirikizumab, a novel anti-IL23p19 monoclonal antibody, offers significant efficacy in inducing and maintaining clinical and endoscopic remission in moderate-to-severe IBD, particularly at the 200 mg dose. Pooled data from four RCTs revealed robust improvements across endpoints: endoscopic response (67.3% at 200 mg vs. placebo), clinical remission (44.5%), and histologic healing (48.5%), with a favorable safety profile (RR 0.44 for serious AEs). Notably, mirikizumab outperformed placebo in symptom control (69.4% symptomatic remission at 200 mg) and quality-of-life metrics (IBDQ improvement: +47.6 points), addressing critical gaps in IBD management where conventional therapies like anti-TNFs and immunomodulators often lose efficacy over time. However, limitations—including heterogeneity among studies, the absence of head-to-head comparisons with other biologics, and small sample sizes for higher doses (600–1000 mg)—warrant cautious interpretation. Future studies should explore mirikizumab’s role in combination regimens and long-term durability beyond 52 weeks. Despite these constraints, our findings position mirikizumab as a promising therapeutic option, particularly for biologic-experienced patients, with optimal efficacy observed at 200–300 mg doses. Regulatory agencies and clinicians should consider these data when evaluating mirikizumab’s place in the IBD treatment paradigm.
Declaration Of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Financial Disclosure
There were no financial interests in any of the procedures, devices, or products mentioned in this manuscript for any of the authors. In addition, no funding or grant was received for this study.
Ethical Statement
This study is a meta-analysis of previously published randomized controlled trials and did not involve the direct collection of new data from human participants. As such, ethical approval and informed consent were not required. All included studies had obtained appropriate ethical approval from their respective institutional review boards.
IRB Approval
No IRB approval required for this manuscript as no human subjects were involved.
Data Availability Statement
Data supporting the findings of this study are available within the article and Supplementary material files.
Registration and Protocol
Our study was registered with the OSF: https://doi.org/10.17605/OSF.IO/C9Q6G
Supplementary Materials
Supplementary materials associated with this article can be found in the Supplementary Figure 1-11 in the supplementary files attached.
Declaration of AI usage:
No generative artificial intelligence (AI) tools or AI-assisted technologies were used in the conception, design, data analysis, writing, or editing of this manuscript. All content was developed and prepared entirely by the authors without the assistance of AI.
Author contribution:
Z.B searched databases for studies
B.H searched databases for studies
S.S performed screening for inclusion and exclusion criteria
L.P performed screening for inclusion and exclusion criteria
M.T.K performed screening for inclusion and exclusion criteria
S.K performed data extraction
N.K performed data extraction
C.K.L performed data extraction
F.G, performed analysis
N.A, performed analysis
Z.A performed analysis
M.J wrote manuscript
H.R Supervised the research project.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org