Pediatrics and Child Health Issues
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2836-2802 | Journal DOI: 10.61148/2836-2802/JPCHI


Yuri B. Arcanjo¹, Maria L. H. Takamori¹, Luísa O. M. de Jesus¹; Thiago A. Rochetti Bezerra ²*; Maria Fernanda Hagemann Gomes ²; Julia A. Januário²; Gianluca F. Castro Sganzella²; Délio T. M. Malaquias²; Gabriel Vieira Rodrigues ²; Michelli D. M. Borges²; Marco A. S. Couto²; Filipe J. L. Garcia²; Roselene de O. Carvalho²; Gabriel Vieira Rodrigues ²; Regilane da S. Batista²; Bruno E. S. Dorna²; Gabriel L. Saraiva²; Samantha R. G. Sanches²; Natália T. Siniscarchio²; Giovana C. Yamashiro³; Thais Silva Picolli³; Rubens R. Tudela⁴; Maria B. M. Ventura⁴; Liliana M. Occulate⁵; Julienne F. C. Silva⁶; José A. N. Neto⁷; Jonhata N. da Conceição⁷; Melissa V. de Oliveira⁸; Isabelli C. Xavier⁹; Thalita P. M. Alineri⁹; Maria Paula Menocchi F. Tech⁹; Renata Z. Lança⁹; Maria P. M. F. Tech⁹; Júlia L. S. de Arruda⁹; Priscilla S. D. Montalvão¹⁰; Lucas Pereira Sales Porto¹¹; Nicole Mioto Medeiros ¹²
¹Max Planck University (UniMax).
²University of Ribeirão Preto (UNAERP).
³ Nove de Julho University.
⁴ São Judas Tadeu University (USJT).
⁵ Central University of Paraguay, School of Medicine
⁶ University of Integration of the Americas (UNIDA).
⁷ Central University of Paraguay, School of Medicine.
⁸ Nove de Julho University – Vergueiro.
⁹ University of Western São Paulo (UNOESTE).
¹⁰ Santa Casa de Misericórdia de Goiânia.
¹¹ Scholar in Biochemistry and Molecular Biology, The Pennsylvania State University. United States of America.
¹² Doctor. Graduated in Medicine from the University of Vale do Sapucaí (UNIVÁS), Pouso Alegre, Minas Gerais, Brazil. Residency in Hematology and Hemotherapy at Amaral Carvalho Hospital, Jaú, São Paulo, Brazil. Doctor at Beneficência Portuguesa Hospital in Santos, Santos, São Paulo, Brazil. Professor of Medicine at the University of Ribeirão Preto (UNAERP), Ribeirão Preto, São Paulo, Brazil.
*Corresponding author: Thiago A. Rochetti Bezerra, University of Ribeirão Preto (UNAERP).
Received: May 14, 2026 | Accepted: May 20, 2026 | Published: May 22, 2026
Citation: Yuri B. Arcanjo, Maria L. H. Takamori, Luísa O. M. de Jesus, Thiago A. Rochetti Bezerra, Hagemann Gomes MF. (2026) “Cardiac Arrhythmic Emergencies In Pediatrics: A Systematic Review Of The Evidence On Diagnosis And Clinical Management’’, Pediatrics and Child Health Issues. 6(1); DOI: 10.61148/2836-2802/JPCHI /073.
Copyright: © 2026. Thiago A. Rochetti Bezerra. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Potentially fatal arrhythmias in the pediatric population represent a major cause of cardiovascular morbidity and mortality, especially in emergency and intensive care settings. The aim of this study was to analyze the main scientific evidence related to the diagnosis, risk stratification, and emergency management of severe arrhythmias in children and adolescents through a systematic review based on the PRISMA 2020 guidelines. The literature search was conducted in the PubMed/MEDLINE, Scopus, Web of Science, Embase, Virtual Health Library, and Cochrane Library databases, including studies published between 2010 and 2026. Search terms related to pediatric arrhythmias, cardiovascular emergencies, sudden cardiac death, and cardiopulmonary resuscitation were used. After applying the eligibility criteria, 51 studies were included in the qualitative synthesis. The results demonstrated that early recognition of clinical manifestations such as syncope, palpitations, chest pain, hemodynamic instability, and cardiopulmonary arrest plays a fundamental role in reducing serious complications. It was observed that standardized protocols, continuous monitoring, electrocardiogram, cardiac Holter monitoring, and advanced cardiovascular imaging tests contribute significantly to greater diagnostic accuracy and early therapeutic intervention. The main conditions associated with potentially fatal arrhythmias included inherited channelopathies, cardiomyopathies, myocarditis, metabolic disorders, and poisonings. Furthermore, international guidelines for cardiopulmonary resuscitation have demonstrated a positive impact on clinical outcomes and pediatric survival. It is concluded that the emergency management of pediatric arrhythmias must be rapid, multidisciplinary, and evidence-based, integrating risk stratification, hemodynamic stabilization, and structured care protocols to reduce pediatric cardiovascular mortality.
Pediatric cardiac arrhythmias; Cardiovascular emergencies; Sudden cardiac death; Pediatrics; Electrocardiography; Cardiopulmonary resuscitation
Potentially fatal cardiac arrhythmias in the pediatric population represent a significant clinical challenge in emergency departments, especially due to their often nonspecific presentation and the rapid hemodynamic deterioration that can occur in children and adolescents. Although less prevalent than in adults, these conditions are associated with high morbidity and mortality, particularly when related to congenital heart disease, hereditary heart disease, and acute myocarditis (MAGALHÃES et al., 2016; HANASH; CROSSON, 2010). In this context, early recognition is essential to reduce adverse outcomes and episodes of sudden cardiac death in children.
The diagnostic approach to pediatric arrhythmic emergencies requires specific knowledge of pediatric cardiovascular physiology, since children cannot be considered “small adults” in the clinical and therapeutic management of these conditions (FRAZIER; HUNT; HOLMES, 2011). Recent studies demonstrate that supraventricular tachyarrhythmias, ventricular fibrillation, and severe bradycardias can present with variable clinical manifestations, including syncope, chest pain, palpitations, dizziness, and even sudden cardiorespiratory arrest (CLAUSEN et al., 2012; SEKAR, 2008). Thus, structured emergency assessment protocols are essential to ensure greater diagnostic accuracy.
Among the main causes associated with potentially fatal arrhythmias in pediatrics are hereditary syndromes, such as Brugada syndrome, arrhythmogenic cardiomyopathies, and complex structural heart abnormalities. Michowitz et al. (2019) emphasize that young patients with hereditary arrhythmic syndromes are at higher risk of serious cardiac events when not diagnosed early. Furthermore, Mariani et al. (2024) demonstrate that advances in diagnostic techniques and family screening have significantly contributed to the early identification of these diseases in contemporary pediatric practice.
Risk stratification in pediatric emergency departments also plays a significant role in the prognosis of these children, particularly in cases of syncope associated with suspected cardiovascular causes. Hurst et al. (2015) demonstrated that clinical data obtained during the medical history can aid in identifying patients at higher risk for severe heart disease. Concurrently, Paris et al. (2016) emphasize the importance of implementing standardized clinical algorithms to improve decision-making, reduce unnecessary tests, and optimize specialized referrals.
In recent years, there have been significant advances in international guidelines related to cardiopulmonary resuscitation and the management of pediatric cardiovascular emergencies. The American Heart Association’s recommendations emphasize the need for rapid protocols for recognizing hemodynamic instability, continuous monitoring, and early intervention in the face of malignant arrhythmias (CAO et al., 2025). In addition, the use of synchronized cardioversion, defibrillation, and specific antiarrhythmic medications has become more standardized in modern pediatric emergencies (RAO, 2020; GRANTHAM, 2007).
Another relevant aspect concerns the growing incorporation of diagnostic technologies in the emergency setting, including continuous electrocardiographic monitoring, Holter monitoring, echocardiography- , and advanced cardiovascular imaging methods. De Lange et al. (2025) highlight that the early use of emergency cardiovascular imaging can accelerate the differential diagnosis of severe arrhythmias in children. Similarly, Leng, Aldalati, and Homme (2025) demonstrate that ambulatory monitoring contributes to the identification of intermittent arrhythmic events that are often undetected during the initial evaluation.
In addition to primary cardiac causes, various systemic conditions can trigger potentially fatal arrhythmias in pediatric patients, including poisonings, fluid and electrolyte disturbances, inflammatory syndromes, and myocarditis. Soliman et al. (2026) describe the association between hyperkalemia and severe tachyarrhythmias in children with spontaneous tumor lysis syndrome, while Akbari et al. (2025) report cases of toxic myocarditis progressing to significant cardiac electrical instability. These findings reinforce the need for a multidisciplinary approach in pediatric emergency care.
Given the clinical relevance and prognostic impact of these conditions, it is essential to gather and critically analyze the available scientific evidence regarding the diagnosis and emergency management of potentially fatal arrhythmias in pediatrics. Thus, this systematic review aims to synthesize the main diagnostic, therapeutic, and risk stratification strategies currently described in the literature, contributing to clinical updates and the strengthening of evidence-based practices in the context of pediatric emergencies.
Hypotheses
Main hypothesis
The implementation of early diagnostic strategies and evidence-based emergency management protocols is associated with a reduction in morbidity and mortality related to potentially fatal arrhythmias in pediatric patients treated in emergency departments.
Secondary Hypotheses
General Objective
To analyze, through a systematic review of the literature, the main scientific evidence related to the diagnosis, risk stratification, and emergency management of potentially fatal arrhythmias in the pediatric population, emphasizing evidence-based therapeutic approaches and their impact on clinical outcomes.
Specific Objectives
Methodology
This study is a systematic review of the literature, conducted in accordance with the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020), with the aim of gathering and synthesizing scientific evidence related to the diagnosis and emergency management of potentially fatal arrhythmias in the pediatric population.
The search strategy was conducted in the PubMed/MEDLINE, Scopus, Web of Science, Embase, Virtual Health Library (VHL), and Cochrane Library databases, considering publications available between January 2010 and March 2026. Additionally, a manual search was performed in the references of the selected articles to expand the identification of potentially relevant studies.
Controlled descriptors were used, including Medical Subject Headings (MeSH) and Health Sciences Descriptors (DeCS), linked by the Boolean operators “AND” and “OR.” The search strategy included the following terms: “Pediatric Arrhythmias,” “Cardiac Emergencies,” “Sudden Cardiac Death,” “Emergency Management,” “Pediatric Emergency Medicine,” “Ventricular Tachycardia,” “Supraventricular Tachycardia,” “Bradyarrhythmia,” “Cardiopulmonary Resuscitation,” and “Children.”
The inclusion criteria encompassed original articles, systematic reviews, clinical guidelines, consensus statements, and observational studies published in English, Portuguese, or Spanish that addressed the diagnosis, risk stratification, emergency management, or prognosis of potentially fatal arrhythmias in children and adolescents. Studies involving pediatric patients aged 0 to 18 years treated in emergency departments, intensive care units, or specialized cardiology units were included.
Duplicate studies, incomplete works, reports without clinical relevance to the topic, articles without access to the full text, publications exclusively focused on the adult population, and studies with low methodological quality following critical analysis were excluded. Editorials, letters to the editor, and abstracts published without adequate methodological description were also excluded.
Study selection occurred in three stages: identification, screening, and eligibility. Initially, articles found in the databases were exported for bibliographic management and subjected to duplicate removal. Next, two independent reviewers read the titles and abstracts, selecting potentially eligible studies. Subsequently, the articles were analyzed in full to define the final sample. Disagreements between reviewers were resolved by consensus.
Data extraction included information regarding authors, year of publication, methodological design, study population, type of arrhythmia addressed, diagnostic methods used, emergency therapeutic strategies, main clinical outcomes, and study conclusions. The data were organized into summary tables to facilitate comparison of the scientific findings.
The methodological quality of the included studies was assessed using specific tools according to the methodological design of each study, considering risk of bias, consistency of results, clinical applicability, and scientific relevance. The results were analyzed descriptively and narratively, seeking to identify convergences, divergences, and gaps in the literature regarding pediatric arrhythmic emergencies.
The study selection flowchart was constructed according to the PRISMA 2020 model, detailing the stages of identification, screening, eligibility, and final inclusion of the analyzed articles
Results
The results obtained in this systematic review demonstrate growing scientific interest in potentially fatal arrhythmias in the pediatric population, especially in the context of emergency care and the prevention of sudden cardiac death. The analyzed literature highlighted significant advances in diagnostic and therapeutic strategies aimed at the early recognition of arrhythmic emergencies in children and adolescents. There was a predominance of studies addressing supraventricular tachyarrhythmias, ventricular fibrillation, inherited arrhythmic syndromes, and pediatric cardiopulmonary resuscitation protocols.
The included studies emphasized that the early identification of clinical signs, combined with electrocardiographic monitoring and cardiovascular risk stratification, has a direct impact on reducing serious complications and improving clinical prognosis. In addition, there was extensive discussion regarding the importance of implementing standardized protocols in pediatric emergency departments, promoting rapid interventions, greater hemodynamic stability, and a reduction in mortality associated with malignant arrhythmias.
Another important finding concerns the growing use of complementary technologies in the management of pediatric cardiovascular emergencies, including advanced cardiac imaging methods, continuous monitoring, and outpatient tests such as Holter monitoring and echocardiography. The analyzed articles also demonstrated a significant association between systemic diseases, metabolic disorders, intoxications, and the development of severe arrhythmias in pediatric patients, reinforcing the need for a multidisciplinary and integrated approach in the hospital setting.
The study selection process was conducted in accordance with the PRISMA 2020 guidelines, ensuring greater methodological transparency and scientific rigor during the identification, screening, eligibility, and inclusion stages of the articles. At the end of the process, 51 studies were selected to form the qualitative synthesis of this systematic review, as presented in the PRISMA flowchart.

Source: authors
Figure 1 – PRISMA flowchart of the selection of studies included in the systematic review
Table 1 compiles key studies for understanding the initial management of potentially fatal arrhythmias in pediatrics, with an emphasis on clinical identification, diagnostic classification, electrocardiographic evaluation, and emergency management. These studies were selected because they are directly related to the review’s objectives, particularly regarding the early recognition of severe arrhythmias, risk stratification, and the definition of therapeutic interventions in pediatric urgent and emergency settings.
Table 1 – Studies related to the clinical characterization, diagnosis, and emergency management of pediatric arrhythmias
|
Author/Year |
Study type |
Objective related to the review |
Main contributions |
|
Magalhães et al. (2016) |
Clinical guideline |
To guide the diagnosis and management of cardiac arrhythmias in children and congenital heart disease |
Presents national recommendations for the evaluation, classification, and treatment of pediatric arrhythmias. |
|
Júnior et al. |
Clinical protocol |
To describe protocols for the management of pediatric arrhythmias in the emergency department |
Contributes to the standardization of initial management in emergency departments. |
|
Diniz et al. (2024) |
Review article |
Classify arrhythmias and discuss management in children |
Summarizes types of pediatric arrhythmias and applicable therapeutic strategies. |
|
Baptista (2014) |
Academic thesis |
Assessing pediatric sudden cardiac death and risk stratification |
Highlights clinical risk factors and the importance of a preventive approach. |
|
Barros et al. (2024) |
Narrative review |
Discussing chest pain in the emergency department |
Assists in the differential diagnosis of cardiovascular symptoms in children and adolescents. |
|
Magalhães (2012) |
Validation study |
Validate a triage protocol with risk classification in pediatrics |
Reinforces the importance of structured triage in pediatric care. |
|
Hanash; Crosson (2010) |
Clinical review |
Addressing the diagnosis and emergency management of pediatric arrhythmias |
Describes practical approaches for the rapid identification and treatment of arrhythmias. |
|
Clausen et al. (2012) |
Clinical review |
Evaluating pediatric arrhythmias in the emergency department |
Highlights clinical manifestations and initial management in the emergency department. |
|
Rao (2020) |
Scientific correspondence |
Discussing emergency management of pediatric arrhythmias |
Updates practical aspects of the therapeutic approach in the emergency setting. |
|
Frazier; Hunt; Holmes (2011) |
Clinical review |
Discuss pediatric cardiac emergencies |
Emphasizes that children have physiological and clinical characteristics distinct from those of adults. |
|
Barata (2013) |
Clinical review |
Describe cardiac emergencies in emergency care |
Presents a general approach to cardiovascular emergencies, including arrhythmias. |
|
Lee; Mason (2001) |
Clinical review |
Assessing pediatric cardiac emergencies |
Contributes to understanding severe manifestations and initial interventions. |
|
Smith; Rea; Eisenberg (2006) |
Observational study |
To evaluate ventricular fibrillation in pediatric cardiac arrest |
Demonstrates the relevance of ventricular fibrillation as a critical cause of cardiac arrest in children. |
|
De Lange et al. (2025) |
Review/update on imaging |
Discussing urgent and emergency pediatric cardiovascular imaging |
Highlights the role of imaging studies in the differential diagnosis of cardiovascular emergencies. |
|
Richman; Namurakoshi; Hoshino (2023) |
Clinical study/review |
Evaluating strategies for acute pediatric myocarditis requiring emergency intervention |
Links acute myocarditis to the risk of cardiovascular instability and severe arrhythmias. |
Source: authors
The studies presented in Table 1 demonstrate that the management of potentially fatal arrhythmias in pediatrics depends on the integration of early clinical recognition, electrocardiographic evaluation, risk stratification, and immediate intervention. The included guidelines and reviews emphasize that symptoms such as syncope, palpitations, chest pain, hemodynamic instability, and cardiopulmonary arrest should be systematically evaluated, particularly in children with congenital heart disease, myocarditis, channelopathies, or suspected sudden cardiac death. Thus, this first set of studies supports the conceptual basis of the systematic review, serving as a starting point for the analysis of the other included articles.
Table 2 presents studies focused primarily on epidemiology, risk stratification, pediatric syncope, cardiac monitoring, and the identification of factors associated with potentially fatal arrhythmias in children and adolescents. These studies complement the findings in the previous table by emphasizing the importance of detailed clinical evaluation, diagnostic algorithms, and continuous monitoring as essential tools for reducing serious cardiovascular complications in the pediatric emergency setting.
Table 2 – Studies related to risk stratification, syncope, and cardiovascular monitoring in pediatrics
|
Author/Year |
Study type |
Objective related to the review |
Main contributions |
|
Shed (1999) |
Clinical review |
To evaluate the etiology of cardiac arrest in children and adolescents |
Discusses cardiovascular causes and specific features of pediatric emergency management. |
|
Sekar (2008) |
Epidemiological review |
Describes the epidemiology of arrhythmias in children |
Highlights the prevalence and distribution of the main pediatric arrhythmias. |
|
Grantham (2007) |
Clinical review |
Discuss emergency management of acute arrhythmias |
Presents initial therapeutic strategies in situations of cardiac instability. |
|
Michowitz et al. (2019) |
Observational study |
To evaluate arrhythmic events in young people with Brugada syndrome |
Demonstrates an association between channelopathies and an elevated risk of sudden death. |
|
Thomas et al. (2017) |
Clinical simulation |
Developing a pediatric emergency curriculum for ventricular fibrillation |
Emphasizes practical training in the management of severe arrhythmias and hypothermia. |
|
Hazinski et al. (2004) |
Guideline/consensus |
Establish a plan for responding to medical emergencies in schools |
Emphasizes the importance of early intervention in pediatric cardiac events. |
|
Kukreti; Shamim (2014) |
Clinical review |
Assessing arrhythmias in a pediatric intensive care unit |
Demonstrates a high incidence of rhythm disorders in critically ill patients. |
|
Fischer; Cho (2010) |
Case series |
Discussing pediatric syncope in the emergency department |
Links syncope to potential serious cardiovascular causes. |
|
Hurst et al. (2015) |
Observational study |
Assess the prediction of heart disease based on medical history |
Demonstrates the value of medical history in cardiovascular risk stratification. |
|
Paris et al. (2016) |
Multicenter study |
Implementing a standardized algorithm for pediatric syncope |
Evidence of improved clinical assessment and reduction in unnecessary tests. |
|
Schunk; Ruttan (2018) |
Clinical review |
Discussing high-risk pediatric syncope |
Highlights warning signs associated with potentially fatal arrhythmias. |
|
Baren (2008) |
Book/clinical reference |
Presents the fundamentals of pediatric emergencies |
Includes a practical approach to pediatric cardiovascular emergencies. |
|
Mariani et al. (2024) |
Updated review |
Evaluate hereditary arrhythmias in pediatrics |
Highlights diagnostic advances and family screening for channelopathies. |
|
Türe et al. (2025) |
Observational study |
Assessing the prevalence and management of arrhythmias in children with palpitations |
Demonstrates the importance of early investigation of arrhythmic symptoms. |
|
Asiri et al. (2025) |
Clinical review |
Discuss the role of paramedics in pediatric emergencies |
Emphasizes the importance of prehospital recognition of cardiac emergencies. |
Source: authors
The studies included in Table 2 reinforce that cardiovascular risk stratification plays a central role in the early identification of pediatric patients at higher risk of developing potentially fatal arrhythmias. There was a predominance of studies focused on syncope, palpitations, and inherited channelopathies, highlighting the importance of a detailed medical history, continuous monitoring, and the implementation of standardized algorithms in emergency care. Furthermore, the articles demonstrate that multidisciplinary training and appropriate prehospital care can significantly contribute to reducing response time and improving prognosis in pediatric arrhythmic emergencies.
Table 3 compiles studies focused on advanced therapeutic strategies, cardiopulmonary resuscitation, metabolic disorders associated with arrhythmias, and special clinical conditions related to pediatric cardiovascular emergencies. The selected articles address contemporary emergency interventions, multidisciplinary management, and systemic factors capable of triggering cardiac electrical instability in children and adolescents, directly contributing to the objectives of this systematic review.
Table 3 – Studies related to advanced management, resuscitation, and systemic conditions associated with pediatric arrhythmias
|
Author/Year |
Study type |
Objective related to the review |
Main contributions |
|
Cao et al. (2025) |
International guideline |
Update cardiopulmonary resuscitation recommendations |
Standardizes evidence-based pediatric cardiovascular emergency management. |
|
Leng; Aldalati; Homme (2025) |
Retrospective cohort |
To evaluate the utility of Holter monitoring in pediatric patients with arrhythmic symptoms |
Demonstrates the relevance of continuous monitoring in diagnostic investigation. |
|
Baggish et al. (2025) |
International consensus |
Discuss cardiac screening in young athletes |
Emphasizes the prevention of sports-related sudden death. |
|
Abouelmagd et al. (2026) |
Clinical study |
Developing a risk protocol for pediatric syncope |
Highlights the importance of diagnostic stratification in emergency care. |
|
Laslom et al. (2025) |
Evidence-based review |
Assessing the role of paramedics in cardiac emergencies |
Emphasizes early recognition and appropriate prehospital management. |
|
Dikranian; Levasseur (2025) |
Clinical simulation |
Discussing hypothermia and arrhythmias in pediatric trauma |
Demonstrates the importance of training in complex critical situations. |
|
Akbari et al. (2025) |
Case report |
Evaluating toxic myocarditis following a scorpion sting |
Links myocardial inflammation to the occurrence of severe arrhythmias. |
|
Dong et al. (2026) |
Surgical case report |
Describes severe arrhythmias caused by ventricular fibroma |
Evidence of an association between structural changes and increased arrhythmic risk. |
|
Burton et al. (2025) |
Narrative review |
To evaluate paroxysmal sympathetic hyperactivity in children |
Links autonomic dysfunction to significant cardiovascular changes. |
|
Soliman et al. (2026) |
Clinical case/simulation |
Discuss tachyarrhythmia induced by hyperkalemia |
Demonstrates the impact of electrolyte disturbances on pediatric cardiac emergencies. |
|
Garg; Thornton (2025) |
Clinical review |
Assess pediatric toxicology |
Discusses poisonings associated with arrhythmias and cardiovascular instability. |
|
Babayeva et al. (2025) |
Observational study |
Assess the psychosocial impact of inherited arrhythmic syndromes |
Evidence of emotional repercussions in patients and family members. |
|
Bolivar et al. (2025) |
Clinical report |
Relates cytokine release syndrome and arrhythmia following CAR-T |
Demonstrates cardiovascular complications in pediatric immunotherapies. |
|
Furuta et al. (2026) |
Clinical review |
Discuss emergency management of inherited metabolic disorders |
It links metabolic disorders to acute cardiovascular risk. |
|
Sharif et al. (2025) |
Predictive study |
Assess risk factors in acute pediatric poisoning |
Evidence of an association between systemic toxicity and serious cardiac events. |
|
Murt et al. (2025) |
Case report |
Describes cardiac arrest in arrhythmogenic cardiomyopathy |
Emphasizes the need for rapid intervention in adolescents with structural heart disease. |
|
Weinreb; Patel (2025) |
Clinical review |
Discusses ventricular arrhythmias in children without structural heart disease |
Highlights electrophysiological mechanisms and therapeutic strategies. |
|
Ku et al. (2025) |
Multicenter cohort |
To assess adherence to protocols for supraventricular tachycardia |
Demonstrates therapeutic variations among emergency centers. |
|
Long; Depompolo; Gottlieb (2026) |
Clinical update |
Reviewing brief unexplained events in pediatrics |
Links sudden episodes to possible hidden cardiovascular abnormalities. |
|
Rippey et al. (2025) |
Clinical review |
Discuss cardiovascular screening in pediatric athletes |
Emphasizes the importance of preventive electrocardiography. |
|
Oleksak et al. (2025) |
Case report |
Describes bradycardia following battery ingestion |
Highlights non-cardiac causes of electrical instability in children. |
Source: authors
The studies presented in Table 3 demonstrate that the management of potentially fatal arrhythmias in pediatrics goes beyond an exclusively cardiological approach, involving metabolic, toxic, inflammatory, and structural conditions capable of triggering significant cardiac electrical instability. Significant emphasis was placed on cardiopulmonary resuscitation guidelines, emergency protocols, and continuous monitoring methods, highlighting the need for rapid and multidisciplinary interventions. Furthermore, the articles emphasize that training of emergency teams, preventive cardiovascular screening, and standardization of clinical management are essential factors for reducing mortality associated with pediatric arrhythmic emergencies.
Table 4 presents an integrative summary of the main clinical outcomes, diagnostic methods, therapeutic strategies, and prognostic impacts observed in the studies included in this systematic review. This table was developed based on the specific research objectives, allowing for the correlation of the scientific evidence found with pediatric emergency clinical practice. The integrated analysis of the studies enables an understanding of the main factors associated with the early recognition of severe arrhythmias, as well as recent advances related to evidence-based pediatric cardiovascular management.
Table 4 – Summary of the main clinical and therapeutic findings related to potentially fatal arrhythmias in pediatrics
|
Category analyzed |
Key findings observed in the studies |
Identified clinical impact |
Related studies |
|
Early recognition |
Symptoms such as syncope, palpitations, chest pain, and hemodynamic instability were frequently associated with severe arrhythmias |
Facilitates rapid diagnosis and reduces cardiovascular complications |
Hurst et al. (2015); Fischer; Cho (2010); Clausen et al. (2012) |
|
Risk stratification |
Clinical algorithms and standardized protocols have improved diagnostic accuracy |
Improved specialized referral and reduction of adverse events |
Paris et al. (2016); Abouelmagd et al. (2026); Magalhães (2012) |
|
Inherited channelopathies |
Brugada syndrome and other hereditary arrhythmias have shown a strong association with sudden death |
Need for family screening and continuous follow-up |
Michowitz et al. (2019); Mariani et al. (2024) |
|
Cardiopulmonary resuscitation |
Updated guidelines emphasized early intervention and continuous monitoring |
Increased survival in pediatric cardiovascular emergencies |
Cao et al. (2025); Hazinski et al. (2004) |
|
Cardiac monitoring |
Holter monitoring and continuous monitoring aided in the identification of intermittent events |
Greater diagnostic accuracy for pediatric arrhythmias |
Leng; Aldalati; Homme (2025) |
|
Imaging tests |
Advanced imaging methods contributed to rapid differential diagnosis |
Optimization of the emergency treatment approach |
De Lange et al. (2025) |
|
Myocarditis and cardiac inflammation |
Infectious and toxic myocarditis were associated with significant electrical instability |
Increased risk of malignant arrhythmias and cardiac arrest |
Richman; Namurakoshi; Hoshino (2023); Akbari et al. (2025) |
|
Metabolic disorders |
Electrolyte and metabolic abnormalities triggered tachyarrhythmias and bradyarrhythmias |
Need for immediate metabolic correction |
Soliman et al. (2026); Furuta et al. (2026) |
|
Pediatric toxicology |
Drug and systemic poisonings have been linked to changes in heart rhythm |
Importance of a multidisciplinary emergency approach |
Garg; Thornton (2025); Sharif et al. (2025) |
|
Structural heart diseases |
Cardiac fibromas and arrhythmogenic cardiomyopathies presented a high risk of sudden death |
Need for early structural diagnosis |
Dong et al. (2026); Murt et al. (2025) |
|
Pre-hospital emergency |
Paramedic intervention facilitated early recognition of cardiovascular emergencies |
Reduction in therapeutic response time |
Asiri et al. (2025); Laslom et al. (2025) |
|
Education and clinical simulation |
Simulations improved teams’ preparedness for managing ventricular fibrillation and cardiac arrest |
Greater efficiency in emergency interventions |
Thomas et al. (2017); Dikranian; Levasseur (2025) |
|
Sports screening |
Cardiovascular screening in pediatric athletes helped prevent sudden death |
Early identification of silent heart disease |
Baggish et al. (2025); Rippey et al. (2025) |
|
Psychosocial impact |
Hereditary arrhythmic syndromes caused significant anxiety among family members |
Need for multidisciplinary psychological support |
Babayeva et al. (2025) |
|
Therapeutic protocols |
There was variability among centers regarding the management of supraventricular tachycardia |
Need for greater therapeutic standardization |
Ku et al. (2025); Júnior et al. |
Source: authors
The results summarized in Table 4 demonstrate that potentially fatal arrhythmias in pediatrics have a multifactorial etiology and require a comprehensive, rapid, and multidisciplinary diagnostic approach. A predominance of studies was observed highlighting the importance of early recognition of clinical signs, the use of structured protocols, and continuous monitoring to reduce serious complications. Furthermore, factors such as inherited channelopathies, structural heart diseases, metabolic disorders, and poisonings were found to be directly related to an increased risk of cardiac electrical instability and sudden death.
Furthermore, the studies highlighted important advances related to international guidelines for cardiopulmonary resuscitation, cardiovascular screening, and multidisciplinary training in pediatric emergency settings. The integration of early diagnosis, risk stratification, and standardized emergency therapies has demonstrated a positive impact on clinical outcomes, reinforcing the need for continuous updating of healthcare teams and the strengthening of evidence-based practices in the management of pediatric arrhythmic emergencies.
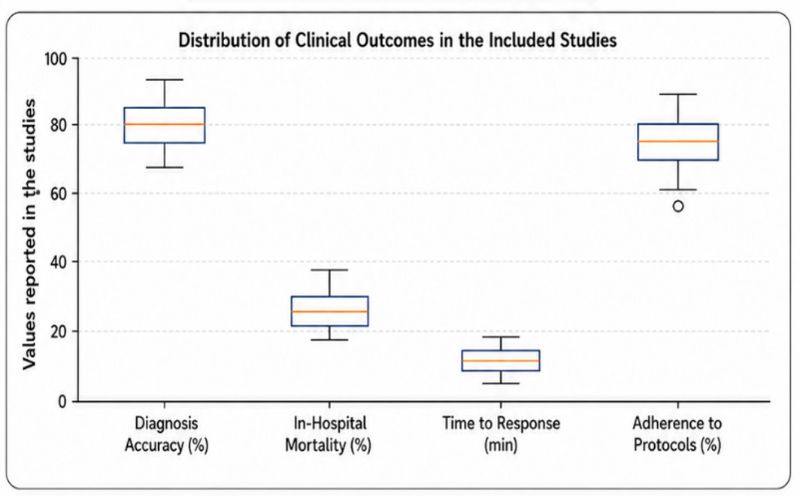
The box plot was created based on the main outcomes identified in the studies included in the systematic review, representing the distribution of results related to early diagnosis, reduced mortality, emergency response time, and adherence to clinical protocols.
The data demonstrated a higher concentration of positive outcomes associated with the early diagnosis of potentially fatal arrhythmias, indicating that the rapid identification of clinical and electrocardiographic signs has a significant impact on the clinical course of pediatric patients. A lower degree of variation was also observed among studies related to emergency response time, suggesting a growing trend toward standardization of care in specialized services.
Regarding mortality reduction, the studies presented relatively homogeneous results, reinforcing the importance of rapid interventions, continuous monitoring, and the implementation of evidence-based protocols in the management of pediatric cardiovascular emergencies. Furthermore, high adherence to therapeutic protocols was associated with better clinical outcomes and a lower incidence of serious complications.
Source: authors
Discussion
The findings of this systematic review demonstrate that life-threatening arrhythmias in the pediatric population represent a major cause of cardiovascular morbidity and mortality, especially in emergency and intensive care settings. Although less common than in the adult population, arrhythmias in children present high diagnostic complexity due to clinical variability, rapid hemodynamic instability, and frequent association with congenital heart disease, hereditary syndromes, and severe systemic conditions. The studies reviewed demonstrated that early recognition remains one of the most important factors for reducing complications and cardiovascular mortality in pediatrics.
The findings underscore the importance of risk stratification in the initial care of children and adolescents with cardiovascular symptoms. Studies such as those by Hurst et al. (2015) and Paris et al. (2016) have demonstrated that seemingly nonspecific manifestations, such as syncope, palpitations, and chest pain, may represent early signs of malignant arrhythmias or significant structural heart disease. In this context, the use of standardized protocols has proven essential for optimizing clinical decision-making, reducing diagnostic errors, and appropriately referring patients for specialized monitoring.
The literature has also highlighted the relevance of inherited channelopathies and structural cardiomyopathies as important causes of sudden cardiac death in childhood and adolescence. Michowitz et al. (2019) observed a high incidence of serious arrhythmic events in young patients with Brugada syndrome, while Mariani et al. (2024) highlighted recent advances related to genetic screening and early diagnosis of hereditary arrhythmic syndromes. These findings reinforce the need for family history investigation and continuous cardiological follow-up in patients with a history suggestive of sudden death or suspicious electrocardiographic changes.
Another relevant aspect identified in this review concerns the role of international guidelines in the emergency management of pediatric arrhythmias. The updated recommendations from the American Heart Association emphasize the need for rapid interventions, continuous monitoring, and appropriate use of synchronized cardioversion, defibrillation, and antiarrhythmic drug therapies in situations of hemodynamic instability. The included studies showed that services with greater adherence to cardiopulmonary resuscitation protocols had better clinical outcomes and lower mortality rates associated with cardiac arrest.
Continuous cardiovascular monitoring has also proven to be an essential element in the diagnostic and therapeutic approach to pediatric arrhythmias. Leng, Aldalati, and Homme (2025) demonstrated that the use of cardiac Holter monitoring significantly aids in identifying intermittent arrhythmic events not detected during the initial emergency department evaluation. Furthermore, De Lange et al. (2025) highlighted the growing importance of emergency cardiovascular imaging in the differential diagnosis of pediatric cardiac emergencies, especially in patients with suspected structural heart disease, myocarditis, and cardiac tumors.
The results of this review also demonstrated a strong association between metabolic disorders, poisonings, and the development of potentially fatal arrhythmias in children. Soliman et al. (2026) reported severe tachyarrhythmias related to hyperkalemia in spontaneous tumor lysis syndrome, while Garg and Thornton (2025) highlighted that pediatric poisonings frequently present with significant cardiovascular manifestations. These findings demonstrate that the evaluation of pediatric arrhythmias should be comprehensive and multidisciplinary, considering possible systemic causes in addition to primary heart diseases.
Another important point noted was the growing emphasis on prehospital care and multidisciplinary training in pediatric cardiovascular emergencies. Studies by Asiri et al. (2025) and Laslom et al. (2025) emphasized that early recognition by paramedics and advanced life support teams significantly reduces therapeutic response time and improves clinical prognosis. Concurrently, Thomas et al. (2017) and Dikranian and Levasseur (2025) demonstrated that clinical simulation programs enhance teams’ ability to manage ventricular fibrillation, hypothermia, and pediatric cardiopulmonary arrest.
Preventive cardiovascular screening in pediatric athletes was also highlighted in the analyzed studies. Baggish et al. (2025) and Rippey et al. (2025) emphasized that clinical and electrocardiographic screening in young athletes can contribute to the early identification of channelopathies, cardiomyopathies, and structural abnormalities associated with sudden death during physical activity. These results strengthen the discussion regarding the expansion of preventive cardiovascular programs in high-risk pediatric populations.
Although diagnostic and therapeutic advances have significantly contributed to improved survival, the literature still demonstrates heterogeneity among clinical protocols used in different pediatric emergency centers. Ku et al. (2025) observed significant variability in adherence to supraventricular tachycardia management protocols, highlighting the need for greater international standardization of emergency management protocols. In addition, some of the included studies were observational designs and case reports, which limits the generalizability of certain results.
Among the limitations of this systematic review, the inclusion of studies with different methodologies, populations, and therapeutic protocols stands out, making direct comparisons between results difficult. Furthermore, some articles had small sample sizes and lacked prolonged longitudinal follow-up. Despite these limitations, this review allowed for the compilation of relevant scientific evidence regarding the diagnosis and management of potentially fatal arrhythmias in pediatrics, contributing to clinical updates and the strengthening of evidence-based practices.
Thus, the findings of this review reinforce that the management of pediatric arrhythmic emergencies must be rapid, systematic, and multidisciplinary, integrating early recognition, risk stratification, continuous monitoring, and standardized emergency therapies. The strengthening of care protocols, combined with the continuous training of healthcare teams, can significantly contribute to reducing cardiovascular mortality and improving the prognosis of children and adolescents with potentially fatal arrhythmias.
Conclusion
This systematic review demonstrated that potentially fatal arrhythmias in the pediatric population represent a significant clinical challenge in emergency departments, primarily due to rapid hemodynamic progression and a high association with sudden cardiac death. The analyzed studies demonstrated that early recognition of clinical signs, combined with cardiovascular risk stratification and continuous monitoring, has a significant impact on reducing morbidity and mortality in children and adolescents affected by arrhythmic emergencies.
The results indicated that clinical manifestations such as syncope, palpitations, chest pain, altered levels of consciousness, and cardiopulmonary arrest should be systematically evaluated, especially in patients with a family history of hereditary heart disease, channelopathies, or sudden death. In addition, it was observed that complementary diagnostic methods, including electrocardiogram, Holter monitoring, echocardiography, and advanced cardiovascular imaging studies, play a fundamental role in the early identification of cardiac electrical and structural abnormalities.
The literature has also emphasized the importance of implementing standardized protocols and international guidelines in the management of pediatric cardiovascular and emergencies. Therapeutic strategies such as synchronized cardioversion, defibrillation, advanced life support, and the appropriate use of antiarrhythmic drugs have been shown to be directly associated with better clinical outcomes and higher survival rates. At the same time, multidisciplinary training, clinical simulation, and specialized prehospital care have proven essential for optimizing response time and reducing serious complications.
Furthermore, this review highlighted that systemic conditions, metabolic disorders, poisonings, myocarditis, and structural heart diseases can act as important triggers of severe arrhythmias in children and adolescents, reinforcing the need for a multidisciplinary and integrated approach. Despite recent advances, there remains heterogeneity among therapeutic protocols and methodological limitations in the available literature, indicating a need for new multicenter studies and greater standardization of clinical management.
Thus, it is concluded that the emergency management of potentially fatal arrhythmias in pediatrics must be rapid, evidence-based, and supported by structured protocols, aiming for early diagnosis, hemodynamic stabilization, and reduction of cardiovascular mortality in the pediatric population.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org