Journal of International Medical Sciences
OPEN ACCESS | Volume 1 - Issue 1 - 2025
ISSN No: - | Journal DOI: 10.61148/IJICM


1Physical Therapist, MedVita Saúde LTDA.
2Physical Therapy, Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira, São Paulo, SP.
3University of Guarulhos (UNG), Physical Therapy, Guarulhos, SP. Multidisciplinary Coordinator, Mandaqui Hospital Complex Bispa Keila Campos Costa Ferreira. MedVita Saúde LTDA.
4Ítalo Brasil Catholic University Center (UNIÍTALO), Physical Therapy, São Paulo, SP.
5Paulista University (UNIP), Physical Therapy, São Paulo, SP.
6Nove de Julho University (UNINOVE), Physical Therapy, São Paulo, SP.
7São Camilo University Center - Nursing, São Paulo, SP.
8City of São Paulo University (UNICID), Physical Therapy, São Paulo, SP.
9Bandeirantes University of São Paulo – Physical Therapy, São Paulo, SP.
10Municipal University of São Caetano do Sul. Physical Therapy, São Caetano do Sul, SP.
11Federal University of Pernambuco, Medicine, Recife, PE. Intensive Care Physician, Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira. Mitre Health Consulting.
12São Camilo University Center, Speech-Language Pathology, São Paulo, SP.
13Nove de Julho University (UNINOVE), Nursing, Coordinator of the Adult Intensive Care Units at the Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira, ABC Foundation.
14University of Guarulhos (UNG), Physical Therapy, Guarulhos, SP.
15Severino Sombra University (UNIVASSOURAS), Medicine, Vassouras, RJ; Specialization in Cardiology from the Portuguese Beneficent Society of São Paulo; Technical Health Director II of the medical clinic management at the Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira.
16Nove de Julho University (UNINOVE), Nursing, São Paulo, SP; Nursing Coordinator of the Adult Emergency Room at the Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira. ABC Foundation.
17Nove de Julho University (UNINOVE), Social Work, São Paulo, SP. Social Worker, Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira. MedVita Saúde LTDA.
18Anhanguera University, Physical Therapy, São Paulo, SP.
19Faculty of Medical Sciences of Santos (FCMS), Medicine, Santos, São Paulo, SP.
20Anhembi Morumbi University, Medicine, São Paulo, SP. Medical Coordinator of the Intensive Care Units at the Mandaqui Hospital Complex, Bishop Keila Campos Costa Ferreira.
21University of Mogi das Cruzes, Physical Therapy, São Paulo, SP. Multidisciplinary Coordinator. Mandaqui Bispa Keila Campos Costa Ferreira Hospital Complex. MedVita Saúde LTDA.
22University of Ribeirão Preto, Medicine, Guarujá, São Paulo.
23Doctor of Medical Sciences. Ribeirão Preto School of Medicine, University of São Paulo.
*Corresponding author: Thiago Augusto Rochetti Bezerra, University of Ribeirão Preto, Medicine, Guarujá, São Paulo.
Doctor of Medical Sciences. Ribeirão Preto School of Medicine, University of São Paulo.
Received: May 12, 2026 | Accepted: May 19, 2026 | Published: May 22, 2026
Citation: Magalhães Alfredo AC, Andréa O Gomes, Felipe D Rodrigues, Jefferson R Cherubim, Gabriela S Thron., (2026). “Patient Safety and The Risk of Falls in The Hospital Setting: A Systematic Review” Journal of International Medical Sciences, 2(1); DOI: 10.61148/IJICM/020.
Copyright: © 2026 Thiago Augusto Rochetti Bezerra. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Hospital falls constitute a significant adverse event related to patient safety, being associated with increased morbidity and mortality, prolonged hospital stays, and higher healthcare costs. The present study aimed to analyze the main scientific evidence related to patient safety and the risk of falls in the hospital setting through a systematic review based on the PRISMA 2020 guidelines. The literature search was conducted in the PubMed/MEDLINE, Scopus, Web of Science, Embase, Virtual Health Library, SciELO, and Cochrane Library databases, including studies published between 2010 and 2026. After applying the eligibility criteria, 72 studies were included in the qualitative synthesis. The results demonstrated that the main factors associated with hospital falls include advanced age, clinical frailty, cognitive impairment, functional limitations, polypharmacy, and the use of potentially sedative medications. The main consequences identified were abrasions, fractures, traumatic brain injuries, functional loss, increased length of hospital stay, and the need for prolonged rehabilitation. It was observed that structured preventive protocols, multidisciplinary educational interventions, continuous monitoring, and the use of predictive scales contribute significantly to reducing the incidence of falls and strengthening hospital safety. Furthermore, the studies highlighted a significant economic impact related to healthcare costs resulting from in-hospital falls. It is concluded that the prevention of hospital falls should involve an integrated multidisciplinary approach, evidence-based care protocols, and the continuous strengthening of institutional strategies focused on patient safety and the quality of hospital care.
Patient safety; Hospital falls; Adverse events; Fall prevention; Hospital care
Patient safety is currently one of the main pillars of care quality in health services, especially in the hospital setting, where adverse events can result in significant clinical, functional, and economic impacts. Among these events, hospital falls stand out due to their high frequency and potential to cause physical harm, prolong hospital stays, and increase morbidity and mortality, particularly among elderly and clinically vulnerable patients (REIS; MARTINS; LAGUARDIA, 2013; GOUVÊA; TRAVASSOS, 2010). In this context, fall prevention has become an integral part of international patient safety protocols and institutional hospital quality programs.
Falls in the hospital setting are considered multifactorial events, associated with intrinsic and extrinsic factors related to the patient, the healthcare team, and the institutional structure. Evans et al. (2001) identified factors such as advanced age, cognitive impairment, functional limitations, and medication use as important determinants of fall risk in hospitalized patients. More recently, Morris et al. (2022) emphasized that the combination of clinical frailty, reduced mobility, and polypharmacy significantly increases the incidence of in-hospital falls, particularly in medium- and high-complexity units.
The elderly population represents one of the groups most susceptible to hospital falls, especially due to the presence of chronic diseases, sarcopenia, balance impairments, and functional dependence. Freire et al. (2024) demonstrated that older adults with diabetes mellitus have an increased risk of falls due to neuropathies, visual impairments, and functional impairment. Similarly, Nakashima et al. (2025) demonstrated a significant association between laboratory-based frailty and the occurrence of in-hospital falls in older adults, reinforcing the importance of comprehensive geriatric assessment during hospitalization.
In addition to clinical conditions, several studies highlight that medications potentially associated with sedation, hypotension, and neurological changes may directly contribute to an increased risk of falls in the hospital setting. Cox et al. (2023) observed a high prevalence of medications linked to an increased risk of falls in hospitalized older adults, while Barker et al. (2022) discussed the association between the continuous use of low-dose aspirin and a higher incidence of falls and fractures in healthy older adults. These findings highlight the importance of medication reviews as a preventive measure in hospitals.
The implementation of institutional fall prevention protocols has demonstrated a positive impact on reducing adverse events related to patient safety. Ximenes et al. (2021) demonstrated that educational interventions targeting multidisciplinary teams significantly contribute to improved adherence to preventive measures. Concurrently, De Figueiredo et al. (2026) emphasized that adequate adherence to fall prevention protocols promotes greater patient safety and a reduction in hospitalization-related complications.
Another relevant aspect concerns patients’ own perceptions of fall risk and their active participation in preventive strategies. Dabkowski et al. (2022) observed that many hospitalized patients have difficulty recognizing their actual level of vulnerability to falls. Furthermore, Vincenzo et al. (2022) demonstrated that educational programs based on self-care and awareness models contribute to greater adherence to prevention strategies and the enhancement of hospital safety.
Nursing teams play a fundamental role in the early identification of risk factors and the implementation of preventive measures related to hospital falls. Dos Santos (2024) emphasized that safe nursing care is directly associated with the reduction of adverse events related to falls. Furthermore, Das Graças Pires et al. (2024) emphasized that the continuous role of nursing in clinical monitoring, patient guidance, and environmental surveillance constitutes an important tool for in-hospital prevention.
In the context of intensive care units and emergency departments, risks related to patient safety become even more complex due to the clinical severity of the patients’ conditions and their high dependence on care. De Barros and Ribeiro (2024) emphasized that critically ill patients are more vulnerable to adverse events, including falls, due to the use of invasive devices, sedation, and functional limitations. Similarly, Diz and Lucas (2022) highlighted the need to strengthen safety strategies in urgent care and emergency hospitals.
Additionally, recent studies have been incorporating new technologies and predictive models for the early identification of the risk of hospital falls. Belso-Garzas developed machine learning-based models to predict the risk of falls in hospitalized patients, while Dormosh et al. (2022) validated electronic predictive models using clinical records from primary care and hospital settings. These tools represent a significant advance toward personalized care and the prevention of adverse events related to patient safety.
Given the high clinical, epidemiological, and care-related relevance of falls in the hospital setting, it is essential to gather and critically analyze the available scientific evidence regarding the main risk factors, preventive strategies, and impacts related to patient safety. Thus, this systematic review aims to synthesize the findings of the contemporary literature on hospital falls, contributing to the strengthening of safe care practices and the implementation of evidence-based preventive protocols.
Hypotheses
Main Hypothesis
The implementation of institutional patient safety protocols and evidence-based preventive strategies significantly reduces the risk of falls in the hospital setting, especially among elderly and clinically vulnerable patients.
Secondary Hypotheses
General Objective
To analyze, through a systematic review of the literature, the main scientific evidence related to patient safety and factors associated with the risk of falls in the hospital setting, emphasizing preventive strategies, care protocols, and clinical impacts resulting from these adverse events.
Specific Objectives
Methodology
This study is a systematic literature review conducted in accordance with the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020), with the objective of analyzing scientific evidence related to patient safety and the risk of falls in the hospital setting.
The literature search was conducted in the PubMed/MEDLINE, Scopus, Web of Science, Embase, Virtual Health Library (VHL), SciELO, and Cochrane Library databases, covering studies published between January 2010 and March 2026. Additionally, a manual search was performed in the references of the selected articles to further identify relevant studies related to the topic.
For the search strategy, controlled vocabulary terms from the Medical Subject Headings (MeSH) and Descritores em Ciências da Saúde (DeCS) were used, combined with the Boolean operators “AND” and “OR.” Among the main terms used were: “Patient Safety,” “Falls,” “Hospital Falls,” “Fall Prevention,” “Risk Factors,” “Inpatients,” “Hospitalization,” “Nursing Care,” “Accidental Falls,” and “Safety Management.”
The inclusion criteria comprised original articles, systematic reviews, meta-analyses, observational studies, clinical trials, and guidelines published in Portuguese, English, and Spanish that addressed risk factors, prevention, institutional protocols, patient safety, and falls in the hospital setting. Studies involving adult and elderly patients hospitalized in clinical, surgical, intensive care, emergency, and inpatient units were included.
Duplicate articles, studies without access to the full text, publications not directly related to the topic, studies conducted exclusively in home settings or long-term care facilities, and studies with low methodological quality following critical analysis were excluded. Editorials, letters to the editor, simple abstracts, and studies without adequate methodological descriptions were also excluded.
The study selection process was conducted in three stages: identification, screening, and eligibility. Initially, articles found in the databases were exported to a bibliographic manager, and duplicates were subsequently removed. Next, two independent reviewers read the titles and abstracts to select potentially eligible studies. Subsequently, the selected articles were evaluated in full, considering the previously defined inclusion and exclusion criteria . Disagreements between reviewers were resolved by consensus.
Data extraction included information regarding authors, year of publication, methodological design, study population, identified risk factors, preventive strategies used, institutional protocols applied, main clinical outcomes, and study conclusions. The data were organized into summary tables and comparative tables to facilitate the analysis of scientific findings.
The methodological quality of the included studies was assessed using specific instruments appropriate to the methodological design of each study, considering risk of bias, consistency of results, clinical applicability, and scientific relevance. The results were analyzed descriptively and narratively, seeking to identify convergences, divergences, and gaps in the literature regarding patient safety and the prevention of hospital falls.
The study selection flowchart was developed according to the PRISMA 2020 model, detailing the stages of identification, screening, eligibility, and final inclusion of the analyzed articles.
Results
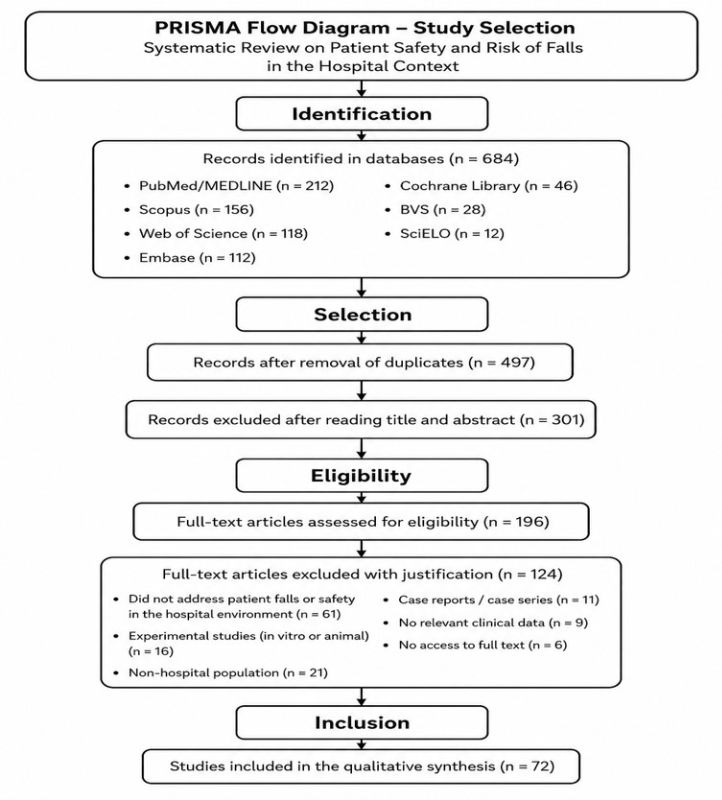
The selection process for the studies included in this systematic review was conducted in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, ensuring greater methodological rigor, scientific transparency, and standardization of the identification, screening, eligibility, and inclusion stages for the analyzed articles. The PRISMA flowchart presented here details all the steps taken during the search and selection process of the literature related to patient safety and the risk of falls in the hospital setting.
Initially, 684 records were identified in the major scientific databases, including PubMed/MEDLINE, Scopus, Web of Science, Embase, Cochrane Library, Virtual Health Library (VHL), and SciELO. After removing duplicates, 497 studies remained for analysis of titles and abstracts. At this stage, 301 articles were excluded because they were not directly related to the review’s topic or did not meet the previously established eligibility criteria.
Subsequently, 196 articles were selected for full-text reading and detailed evaluation regarding methodological and scientific relevance. During the eligibility stage, 124 studies were excluded for various reasons, including the absence of a specific focus on hospital falls and patient safety, the use of experimental models, studies conducted outside the hospital setting, case reports, the absence of relevant clinical data, and the unavailability of the full text.
At the end of the selection process, 72 studies were included in the qualitative synthesis of this systematic review. The selected articles allowed for a comprehensive and y analysis of the main risk factors associated with hospital falls, preventive strategies, institutional patient safety protocols, educational interventions, and clinical impacts related to in-hospital adverse events, contributing to the strengthening of evidence-based care practices and the improvement of the quality of hospital care.
The studies included in this systematic review demonstrate that the risk of falls in the hospital setting is an important indicator related to patient safety and quality of care. The reviewed literature showed that in-hospital falls have a multifactorial etiology, involving clinical, functional, environmental, and organizational factors. Among the main associated factors are advanced age, frailty, cognitive impairment, polypharmacy, limited mobility, use of sedative medications, and failures in the implementation of preventive protocols. Furthermore, the studies highlight the importance of interprofessional and multiprofessional collaboration, particularly by nursing staff, in the early identification of risk factors and the development of evidence-based preventive strategies.
The main findings also indicated that standardized protocols, educational interventions, and the use of predictive scales contribute significantly to reducing the incidence of falls and strengthening the hospital safety culture. There has been a growing incorporation of technological models and patient-centered strategies to improve the prevention of adverse events related to falls. Thus, Table 1 presents the main studies related to risk factors, patient safety, and preventive strategies in the hospital setting.
Table 1 – Key studies related to patient safety and the risk of falls in the hospital setting
|
Author/Year |
Study type |
Objective related to the review |
Key findings |
|
Abreu et al. (2016) |
Metasynthesis |
To assess hospital falls and patient safety |
They demonstrated the impact of falls on the quality of hospital care. |
|
Ajibade (2025) |
Clinical review |
Discussing the assessment and prevention of falls in older adults |
Emphasized the importance of early fall risk stratification. |
|
Almeida (2023) |
Narrative review |
Assessing fall prevention and patient safety |
Highlighted preventive measures and the role of nursing. |
|
Althomali (2025) |
Literature review |
Discussing risk factors for falls in older adults |
Identified frailty and comorbidities as predominant factors. |
|
Barker et al. (2022) |
Clinical trial |
To evaluate the relationship between aspirin and falls |
Demonstrated an association between aspirin use and an increased risk of fractures. |
|
Belso-Garzas |
Predictive study |
Develop a predictive model for falls |
Demonstrated the applicability of artificial intelligence in hospital prevention. |
|
Boell et al. (2025) |
Clinical review |
Discussing the prevention of hospital falls |
Emphasized the importance of institutional protocols. |
|
Cox et al. (2023) |
Observational study |
Assess medications associated with the risk of falls |
Demonstrated the impact of polypharmacy in hospitalized older adults. |
|
Dabkowski et al. (2022) |
Scoping review |
To assess patients’ perception of fall risk |
They identified low individual risk perception among hospitalized patients. |
|
Da Costa-Dias (2014) |
Doctoral dissertation |
Investigate hospital-related risk factors |
Evidence of environmental and clinical influences on in-hospital falls. |
|
Da Silva Albertini et al. (2023) |
Implementation project |
Evaluating patient-centered care |
Demonstrated a reduction in falls following the implementation of best practices. |
|
Das Graças Pires et al. (2024) |
Clinical review |
Evaluating nursing interventions in fall prevention |
They highlighted continuous monitoring as an essential preventive measure. |
|
De Barros; Ribeiro (2024) |
Systematic review |
Investigating safety-related risks in the ICU |
They demonstrated greater vulnerability among critically ill patients. |
|
De Figueiredo et al. (2026) |
Clinical review |
Assessing adherence to preventive protocols |
They demonstrated improved patient safety with standardized protocols. |
|
De Melo et al. (2025) |
Clinical review |
Assess risk factors in hospitalized older adults |
They identified frailty and functional dependence as relevant factors. |
|
De Oliveira et al. (2021) |
Systematic review |
Assessing medication safety |
They linked medication errors to an increase in adverse events. |
|
According to Lucas (2022) |
Systematic review |
Assessing patient safety in emergency hospitals |
They emphasized the need to strengthen preventive strategies. |
|
Dormosh et al. (2022) |
Validation study |
Developing a predictive model for falls |
Demonstrated the effectiveness of electronic records in risk stratification. |
|
Dos Santos (2024) |
Systematic review |
Evaluate fall prevention in nursing |
Highlighted the strategic role of nursing in hospital safety. |
|
Evans et al. (2001) |
Systematic review |
Identifying risk factors for hospital falls |
They linked age, reduced mobility, and medications to falls. |
|
Ferraz et al. (2022) |
Integrative review |
Assessing the safety of hospitalized older adults |
They demonstrated greater vulnerability among hospitalized older adults. |
|
Freire et al. (2024) |
Systematic review and meta-analysis |
Assessing the risk of falls in elderly people with diabetes |
They identified neuropathy and functional impairments as relevant factors. |
|
Ghosh et al. (2022) |
Retrospective cohort |
To assess factors associated with the severity of falls |
They demonstrated an association between frailty and more severe injuries. |
|
Gouvêa; Travassos (2010) |
Systematic review |
To assess patient safety indicators |
They highlighted the importance of institutional monitoring of adverse events. |
|
Heng et al. (2022) |
Qualitative study |
Assess barriers to preventive education |
Identified difficulties in implementing educational strategies. |
The studies presented in Table 1 demonstrate that hospital falls represent a significant challenge related to patient safety and the quality of care. There was a predominance of research aimed at identifying clinical and functional risk factors, especially in elderly, frail patients, and those on multiple medications. Additionally, the articles highlighted that environmental factors, structural limitations, and failures in adherence to institutional protocols also contribute significantly to the occurrence of adverse events related to falls.
Table 2 compiles studies primarily related to preventive strategies, institutional protocols, educational interventions, and multidisciplinary approaches aimed at reducing the risk of falls in the hospital setting. The analyzed articles demonstrate that fall prevention depends not only on the identification of clinical risk factors but also on the implementation of structured organizational measures, the strengthening of a safety culture, and the active participation of patients and healthcare professionals. There has been a growing emphasis on educational programs, the use of predictive scales, and patient-centered strategies as fundamental tools for improving hospital safety.
Furthermore, the included studies highlighted that institutional adherence to preventive protocols is directly associated with a reduction in adverse events, shorter hospital stays, and improved quality of care. The literature also showed that ongoing educational interventions targeting multidisciplinary teams significantly contribute to greater recognition of risk factors and the strengthening of evidence-based care practices.
Table 2 – Studies related to preventive strategies and safety protocols for reducing hospital falls
|
Author/Year |
Study type |
Objective related to the review |
Main findings |
|
Hollinghurst et al. (2022) |
Observational study |
To assess the annual incidence of falls in older adults |
Demonstrated an association between frailty, dementia, and an increased risk of falls. |
|
Jarden et al. (2025) |
Qualitative meta-synthesis |
To assess patients’ experiences following falls |
They highlighted the emotional and psychological impact of hospital falls. |
|
McKercher et al. (2024) |
Systematic review |
Analyze global guidelines for fall prevention |
Identified heterogeneity among international institutional protocols. |
|
Miorin et al. (2020) |
Observational study |
Assess risks during prehospital transfer |
Highlighted care-related risks associated with continuity of care. |
|
Morris et al. (2022) |
Systematic review and meta-analysis |
Assessing interventions to reduce falls |
Demonstrated the effectiveness of multidisciplinary preventive programs. |
|
Nakashima et al. (2025) |
Observational study |
To assess frailty and hospital falls |
A direct relationship between frailty and increased risk of falls was identified. |
|
Porcel-Gálvez et al. (2022) |
Predictive study |
To validate a predictive scale in a hospital setting |
They demonstrated that the risk scale is clinically applicable. |
|
Randell et al. (2024) |
Realistic research |
To evaluate risk assessment practices in hospitals |
They demonstrated the importance of institutional integration in prevention. |
|
Reis; Martins; Laguardia (2013) |
Narrative review |
Discussing patient safety as a dimension of quality |
They reinforced the importance of an institutional safety culture. |
|
Rezende (2020) |
Systematic review |
Evaluate interventions related to patient identification |
Linked care failures to the occurrence of adverse hospital events. |
|
Santos et al. (2019) |
Systematic review |
To evaluate patient safety in Brazilian hospitals |
Demonstrated the need to strengthen preventive strategies. |
|
Saucedo et al. (2020) |
Systematic review |
Assessing patient safety in plastic surgery |
Highlighted the importance of preventive care protocols. |
|
Villar; Duarte; Martins (2020) |
Narrative review |
Assessing the patient’s perspective on hospital safety |
They highlighted the patient’s active participation in the prevention of adverse events. |
|
Vincenzo et al. (2022) |
Mixed-methods study |
Assessing self-care plans for fall prevention |
Demonstrated improved adherence to preventive measures. |
|
Ximenes et al. (2021) |
Systematic review |
To evaluate the effectiveness of educational interventions |
They demonstrated a reduction in the risk of falls following multidisciplinary education. |
|
Heng et al. (2022) |
Qualitative study |
Investigate barriers and facilitators of prevention |
They demonstrated the need for ongoing team training. |
|
Ajibade (2025) |
Clinical review |
Discussing risk assessment in healthcare institutions |
Reinforced the importance of functional assessment scales. |
|
Boell et al. (2025) |
Clinical review |
Evaluate preventive strategies for falls |
Highlighted structured protocols as effective measures. |
|
Dos Santos (2024) |
Systematic review |
Evaluating fall prevention in nursing |
Highlighted the strategic role of hospital nursing. |
|
Da Silva Albertini et al. (2023) |
Implementation project |
Implementing patient-centered care |
Demonstrated improvement in patient safety indicators. |
The studies presented in Table 2 demonstrate that fall prevention in the hospital setting depends directly on the integration of institutional protocols, interprofessional education, and active patient participation in care. A predominance of research related to the implementation of preventive programs, the use of risk assessment scales, and the strengthening of an organizational culture focused on patient safety was observed. Furthermore, the articles demonstrated that continuous educational strategies directed at healthcare teams significantly contribute to greater adherence to preventive measures and a reduction in in-hospital adverse events.
Another relevant aspect identified was the growing incorporation of patient-centered models and predictive technological tools for the individualization of preventive care. The results reinforce that the implementation of standardized protocols, combined with continuous monitoring of hospital safety indicators, has a positive impact on reducing the incidence of falls, improving the quality of care, and strengthening evidence-based practices in the hospital setting.
The studies included in this systematic review demonstrated that falls in the hospital setting can lead to significant clinical, functional, and psychological consequences for patients, especially among the elderly, frail individuals, and patients with multiple comorbidities. Injuries resulting from falls vary widely in severity, ranging from minor abrasions to complex fractures, h , traumatic brain injury, and death, contributing significantly to increased length of hospital stay, hospital costs, and impaired quality of life.
The reviewed literature showed that fractures, contusions, and head injuries are among the main complications associated with in-hospital falls. Furthermore, several studies highlighted that patients who suffer falls are at higher risk of functional loss, limited mobility, recurrent fear of new falls, and the need for prolonged rehabilitation. The graph below summarizes the main health consequences observed in the selected studies.
The graphical analysis demonstrates a predominance of abrasions and contusions among the most frequently reported injuries in the studies, followed by fractures and muscle injuries. Although less frequent, head injuries and hemorrhages were more strongly associated with serious outcomes and the need for specialized interventions. It was also observed that fall-related deaths, although less prevalent, represent an important indicator of the severity of these adverse events in the hospital setting.
The findings reinforce the need to implement structured preventive protocols, continuously monitor high-risk patients, and strengthen multidisciplinary strategies focused on hospital safety. Thus, fall prevention not only reduces physical adverse events but also directly contributes to improving the quality of care, reducing hospital costs, and strengthening the patient safety culture.
Figure 1 below shows the distribution of the main clinical consequences related to falls in the hospital setting observed in the studies included in this systematic review. The graph illustrates the relative frequency of the injuries most commonly associated with in-hospital falls, highlighting the predominance of abrasions, contusions, and fractures among affected patients.
Furthermore, it is observed that head injuries, hemorrhages, and deaths, although less frequent, are associated with outcomes of greater clinical severity and functional impact, especially in the elderly and frail patients. These results reinforce the importance of implementing structured preventive protocols and continuous monitoring of hospitalized patients at higher risk of falls.
The findings demonstrate that hospital falls are not merely isolated events but significant factors associated with increased morbidity, prolonged hospital stays, the need for rehabilitation, and higher hospital costs. Thus, multidisciplinary preventive strategies and early interventions remain essential for strengthening patient safety and improving the quality of care in the hospital setting.
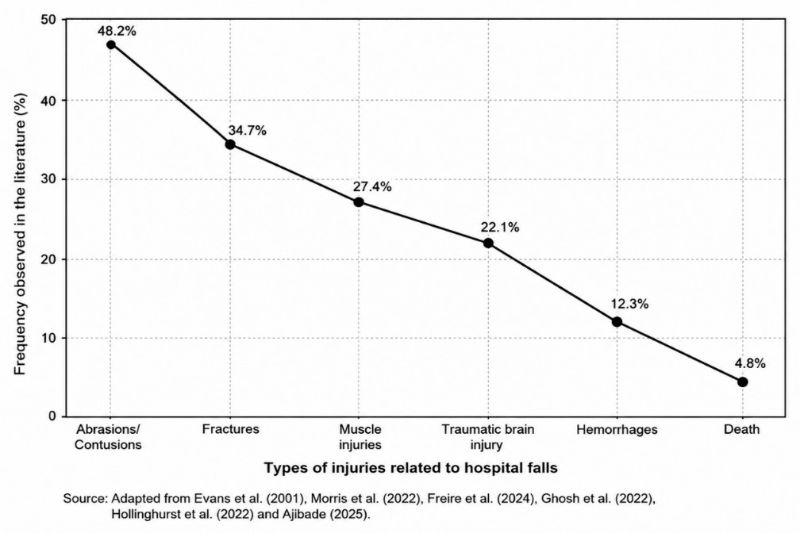
Figure 1 – Main Clinical Consequences of Hospital Falls in Inpatients: Summary of Included Studies
The studies included in this systematic review demonstrated that hospital falls have a significant economic impact on healthcare systems, substantially increasing the clinical, operational, and administrative costs of hospitals. Among the main factors associated with increased costs are prolonged hospital stays, the need for surgical treatment of fractures, physical therapy rehabilitation, use of intensive care units, and the performance of additional tests.
In addition, fall-related events can generate additional indirect costs, including legal proceedings, prolonged work absence, and the need for ongoing multidisciplinary support. The graph below presents a summary of the main economic components associated with hospital falls identified in the analyzed studies.
The graphical analysis shows that increased length of hospital stay represents the main economic component related to hospital falls, followed by costs associated with fracture treatment and physical therapy rehabilitation programs. A significant impact was also observed regarding intensive care and imaging tests, especially in patients with head injuries and severe injuries resulting from falls.
The findings reinforce that the implementation of evidence-based preventive strategies has not only a positive clinical impact but also significant potential for reducing hospital costs. Thus, structured preventive protocols, continuous monitoring of high-risk patients, and strengthening of patient safety practices represent essential measures for improving the quality of care and optimizing institutional resources.
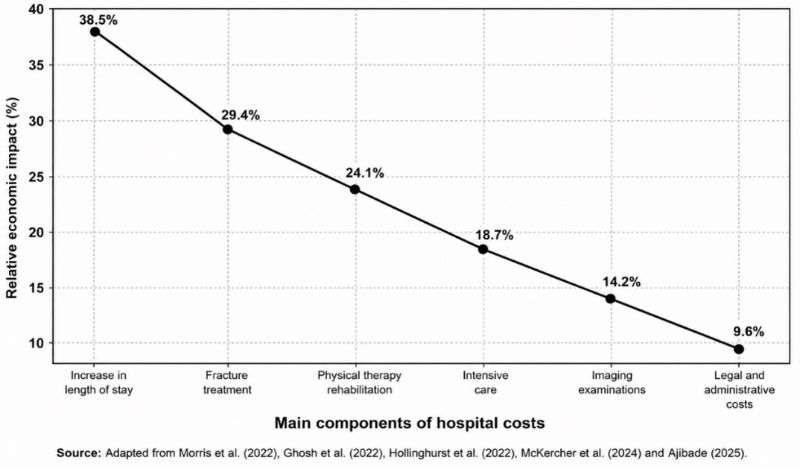
Figure 2 – Main Economic Impacts of Hospital Falls: Summary of Costs Reported in the Literature
Discussion
The findings of this systematic review demonstrate that falls in the hospital setting remain among the leading adverse events related to patient safety, having significant clinical, functional, and economic impacts on healthcare institutions. The analyzed literature showed that in-hospital falls have a multifactorial etiology, involving intrinsic factors related to patients’ clinical conditions and extrinsic factors associated with the hospital environment, institutional organization, and care practices. In this context, the results reinforce that fall prevention should be understood as a strategic priority within patient safety policies.
The included studies demonstrated a predominance of fall risk among hospitalized elderly patients, especially those with clinical frailty, functional deficits, cognitive impairments, and multiple comorbidities. Evans et al. (2001) identified advanced age, reduced mobility, and medication use as key factors associated with hospital falls. Similarly, Freire et al. (2024) observed that older adults with diabetes mellitus have a significantly increased risk due to the presence of peripheral neuropathies, visual impairments, and functional impairment. Nakashima et al. (2025) also demonstrated a strong association between laboratory-confirmed frailty and the occurrence of in-hospital falls in older adults.
Clinical frailty has been shown to be one of the factors most frequently associated with the severity of injuries resulting from falls. Ghosh et al. (2022) demonstrated that frail patients are more likely to develop head injuries, fractures, and require intensive care following falls. Hollinghurst et al. (2022) emphasized that the presence of dementia, functional dependence, and social deprivation significantly increases the risk of fall-related hospitalizations among hospitalized older adults. These results demonstrate that systematic geriatric and functional assessment should be integrated into hospital preventive protocols.
Another aspect widely addressed in the literature concerns the impact of polypharmacy and the use of potentially sedative medications on the risk of falls. Cox et al. (2023) identified a high prevalence of medications associated with an increased risk of falls among hospitalized older adults, while Barker et al. (2022) observed an association between the continuous use of low-dose aspirin and a higher incidence of falls and fractures. Furthermore, De Oliveira et al. (2021) highlighted that failures related to medication prescription, administration, and monitoring can directly contribute to the occurrence of adverse in-hospital events.
The results of this review also highlighted the importance of a multidisciplinary approach in preventing hospital falls, particularly involving the nursing team. Dos Santos (2024) emphasized that safe nursing care has a direct impact on the early identification of risk factors and the implementation of preventive measures. Das Graças Pires et al. (2024) emphasized that continuous monitoring, environmental surveillance, and patient education represent fundamental strategies for reducing adverse events related to falls. Additionally, Almeida (2023) highlighted that preventive interventions carried out by nursing staff contribute significantly to strengthening a culture of patient safety.
The implementation of standardized institutional protocols was also strongly associated with a reduction in the incidence of hospital falls. Ximenes et al. (2021) demonstrated that educational interventions targeting multidisciplinary teams increase adherence to preventive strategies and reduce adverse events related to falls. De Figueiredo et al. (2026) emphasized that adherence to preventive protocols promotes greater patient safety and improves institutional quality indicators. Morris et al. (2022), in a systematic review and meta-analysis, observed that multidisciplinary preventive programs significantly reduce the frequency of in-hospital falls.
The analyzed studies also highlighted the importance of active patient participation in preventive strategies. Dabkowski et al. (2022) demonstrated that many hospitalized patients have limited awareness of their own risk of falling, hindering adherence to preventive guidelines. Villar, Duarte, and Martins (2020) emphasized that involving patients in safety strategies strengthens person-centered care and contributes to improved quality of care. Vincenzo et al. (2022) demonstrated that self-care plans and health education promote greater adherence to preventive measures and reduce the risk of falls.
Another relevant finding concerns the growing use of technological tools and predictive models in the prevention of hospital falls. Belso-Garzas developed predictive models based on artificial intelligence capable of identifying patients at higher risk for in-hospital falls. Similarly, Dormosh et al. (2022) validated electronic predictive models using clinical records, demonstrating high applicability in the early stratification of fall risk. These technologies represent an important advance in the individualization of hospital preventive strategies.
In the organizational context, Reis, Martins, and Laguardia (2013) emphasized that patient safety should be understood as a central dimension of healthcare quality. Gouvêa and Travassos (2010) emphasized the importance of continuously monitoring institutional indicators related to hospital safety, while Randell et al. (2024) demonstrated that the effectiveness of preventive protocols depends directly on institutional integration and an organizational culture focused on patient safety.
The results of this review also highlighted a significant economic impact resulting from hospital falls. Prolonged length of stay, fracture treatment, the need for physical therapy rehabilitation, and the use of intensive care units were among the main cost components related to fall events. McKercher et al. (2024) emphasized that the implementation of structured clinical guidelines has significant potential to reduce hospital costs and improve care efficiency. Furthermore, Ajibade (2025) highlighted that appropriate preventive strategies reduce not only morbidity but also administrative and legal costs associated with adverse events.
Despite the advances observed in the literature, the studies analyzed exhibited methodological heterogeneity regarding preventive protocols, study populations, and fall risk stratification criteria. Some of the included studies also featured observational designs and narrative reviews, limiting direct comparisons between results . However, this review allowed for the compilation of robust scientific evidence regarding the main risk factors, preventive strategies, and impacts associated with hospital falls, contributing to the strengthening of evidence-based care practices.
Thus, the findings reinforce that the prevention of hospital falls should involve a multidisciplinary approach, standardized institutional protocols, continuous monitoring, and active patient participation in care. The integration of continuing education, the use of predictive technologies, and the strengthening of an institutional safety culture holds significant potential for reducing adverse events related to falls and improving the quality of hospital care.
Conclusion
This systematic review demonstrated that falls in the hospital setting represent a major challenge related to patient safety and the quality of healthcare. The analyzed studies showed that in-hospital falls have a multifactorial etiology, involving clinical, functional, medication-related, environmental, and organizational factors, and are more frequent in elderly, frail patients with multiple comorbidities.
The results identified that advanced age, functional limitations, cognitive impairments, clinical frailty, polypharmacy, and the use of potentially sedative medications are among the main factors associated with an increased risk of hospital falls. Furthermore, it was observed that falls can result in significant clinical consequences, including abrasions, fractures, traumatic brain injuries, functional loss, prolonged hospital stays, and increased hospital morbidity and mortality.
The literature has also demonstrated that structured preventive protocols, continuous monitoring, multidisciplinary educational interventions, and the use of predictive scales contribute significantly to reducing the incidence of falls and strengthening the institutional safety culture. The role of nursing stood out as a central element in the early identification of risk factors, the implementation of preventive measures, and the promotion of safe care.
Additionally, studies have highlighted a significant economic impact associated with hospital falls, primarily due to prolonged hospital stays, the need for rehabilitation, surgical treatments, and the use of highly complex resources. In this context, the implementation of evidence-based preventive strategies holds significant potential for reducing hospital costs and improving the quality of care.
Thus, it is concluded that the prevention of hospital falls should be understood as a strategic priority within patient safety policies, requiring multidisciplinary integration, strengthening of institutional protocols, continuous monitoring of high-risk patients, and the development of care practices centered on the safety and quality of hospital care.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org