International Journal of Medical Case Reports and Medical Research
OPEN ACCESS | Volume 5 - Issue 1 - 2026
ISSN No: 2994-6905 | Journal DOI: 10.61148/2994-6905/IJMCRMR


Jayasekara Sandeep1*, Senarathna Loshan1, Weerawansa Lakshitha1 and Jayasuriya Nadeena2
1Teaching Hospital Peradeniya.
2Faculty of Dental Sciences, University of Peradeniya.
*Corresponding Author: Jayasekara Sandeep, Teaching Hospital Peradeniya.
Received Date: June 16, 2024
Accepted Date: June 25, 2024
Published Date: July 29, 2024
Citation: Jayasekara Sandeep, Senarathna Loshan, Weerawansa Lakshitha and Jayasuriya Nadeena. (2024) “End-to-End Anastomosis with Internal Jugular Vein as A Last Resort in Salvaging Venous Compromise of Fibular Free Flap.”, International Journal of Medical Case Reports and Medical Research, 3(2); DOI: 10.61148/2994-6905/IJMCRMR/049.
Copyright: © 2024. Jayasekara Sandeep. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In majority of cases, a free flap is used in conjunction with an end-to-side anastomosis to a preserved vein in head and neck reconstruction. However, selecting the recipient vein after a neck dissection with only a ligated internal jugular vein/external jugular vein (IJV/EJV) is frequently problematic. If all previous methods have failed, end-to-end anastomosis with the IJV may be the last remaining choice. This paper emphasizes the value of maintaining a variety of options while discussing the success story of that uncommon option.
Introduction:
Fibular free flap is the gold standard among mandibular reconstruction methods due to the adequate length of bone (up to 26cm), consistent anatomy of blood supply, shape and quality of bone, and ability of oral rehabilitation in a later stage.[1]. A problem arises from the pedicle's relatively short length, which is made up of the peroneal artery and its venae comitantes, unless the pedicle is cut off from the fibula more proximally and combined with the distal bone for reconstruction. Anastomosis becomes challenging due to the inability to preserve multiple veins for anastomosis, when the necessity of performing neck dissection is arisen in the presence of oral cancer. Usually end-to-side anastomosis with the internal jugular vein (IJV) has shown superior results in the literature. Thus it has been recognized as the first choice for venous anastomosis in free flaps [2]. Vessel size discrepancy, wide capacity and respiratory venous pump effect are known to be main reasons for its superiority in relation to end-to-side anastomosis [3].
Evidence of end-to-end anastomosis with the IJV when other options are failing cannot be seen in the literature, although it could be an alternative or perhaps the last resort depending on the situation. This paper discusses the success story of that rare option while emphasizing the importance of keeping multiple options.
Case report:
A 58-year-old lady with a bony hard swelling in anterior mandible was diagnosed with clear cell odontogenic carcinoma. In ultrasonography of neck showed bilateral enlarged lymph nodes in relation to neck levels IA,IB and II. Patient underwent segmental mandibulectomy, bilateral selective neck dissection and reconstruction of the defect with fibular free flap. 14cm sized fibular free flap was harvested from left side lower limb and it was immediately oriented in such a way that 5cm fibular segments representing the either side of the mandible and 4cm for the middle anterior region. ( 5cm+ 4cm+ 5cm = 14cm )Initially arterial and venous anastomosis were done with right side superior thyroid artery and end-to-side with internal jugular vein respectively. But following the failure due to venous thrombosis, length of the peroneal veins was compromised and secondly anastomosis was carried out with the help of vein graft taken from one of two peroneal veins. Eventually when it was failed, there was a short of 3cm distance to the closest site of internal jugular vein. Exploring the left side neck for seeking a site for anastomosis was not attempted due to the fact that most of the veins could be compromised in the presence of neck dissection. Besides the idea of harvesting a vein graft from a different site was not executed as it had already been set out. Ultimately end to end anastomosis with internal jugular vein became successful and venous drainage was well-established giving the solution for previous ill-fated anastomosis attempts.
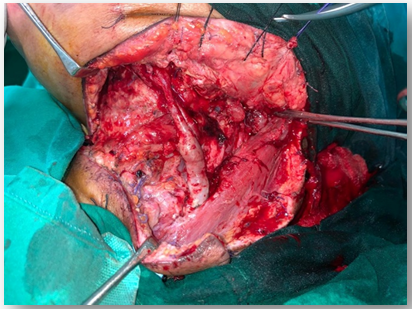
Figure 1: After end-to-end anastomosis with IJV.
Discussion:
Fibular free flap is essentially a better choice for reconstruction in oral and maxillofacial cancer surgery. Maintaining a good blood supply and uninterrupted venous drainage would count for the success of free flap survival. Failure of free flaps are caused mainly due to venous thrombosis rather than arterial thrombosis [3].
Majority of cases, Surgeon finds it difficult to spare multiple veins for the anastomosis purpose, as they could be sacrificed during neck dissection and tumour extirpation following extensive head and neck cancer surgery. That is applicable specially in a case like this, where bilateral neck dissection had to be performed. If the pedicle of fibular flap could be harvested with the sufficient length, end-to-side anastomosis with IJV has been recognized as the best choice. As the literature shows, there is less chance of venous thrombus propagation along with IJV. Length of the pedicle can be increased if the fibular flap is harvested more proximally. But in accordance with the defect to be reconstructed, harvesting the fibular flap with sufficient lengthened pedicle that matches the defect would be an issue. In such situations, keeping multiple choices would solve the problem. But in an instance when end –to-side anastomosis and vein graft have been unsuccessful resulting shortage of distance, end to end anastomosis with IJV would be irrevocable. The vessel diameter discrepancy is a main factor which should be taken into the consideration when it comes to end-to-end anastomosis. If the vessel diameter mismatch is less than 3:1, success rate of the anastomosis is increased [5]. The diameter of IJV more distally is more or less similar to the diameter of peroneal vessels and as a consequence it does not readily produce issues related to caliber mismatch. Therefore end to end anastomosis with IJV could be the last resort in salvaging venous compromised free flaps especially as it will also demonstrably bring out the pedicle length problem.
Conflicts of interest:
All authors declare that they have no conflicts of interest to disclose.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org