International Journal of Interventional Radiology and Imaging
OPEN ACCESS | Volume 4 - Issue 1 - 2026
ISSN No: 3065-6702 | Journal DOI: 10.61148/3065-6702/IJIRI


Sabareesh Suresh Kumar1, Adithya Mani2, R Rajarajan3*, TCR Ramakrishnan4, Raja Vel Shantharam5, Sailesh I S Kumar6
1Interventional Neuro and vascular Radiologist Kg Hospital, Coimbatore.
2Department of Internal Medicine, Coimbatore medical college, Coimbatore.
3Consultant Radiologist KG Hospital, Coimbatore.
4Consultant Neurologist, KG Hospital, Coimbatore.
5Department of Community Medicine, Sri Lalithambigai Medical College and Hospital, Chennai, TN, India.
6Institute of Internal Medicine, Madras Medical College, Chennai, India.
*Corresponding author: Dr. Raja Vel Shantharam, Assistant Professor, Department of Community Medicine, Sri Lalithambigai Medical College and Hospital, Chennai, TN, India.
Received: June 22, 2026 | Accepted: June 29, 2026 | Published: July 01, 2026
Citation: Sabareesh S Kumar, Mani A, R Rajarajan, TCR Ramakrishnan, Raja V Shantharam, Sailesh I S Kumar. (2026) “Carotid Artery Stenting for Carotid Artery Stenosis Under Local Anesthesia: A Case Series”, International Journal of Interventional Radiology and Imaging, 4(1); DOI: 10.61148/ 3065-6702/ IJIRI/049.
Copyright: © 2026. Raja Vel Shantharam. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Carotid artery stenosis is a major cause of ischemic stroke and transient ischemic attack. Carotid endarterectomy remains the standard treatment for symptomatic stenosis ≥50% and asymptomatic stenosis ≥60%; however, carotid artery stenting (CAS) has emerged as a minimally invasive alternative in appropriately selected patients. Limited real-world evidence from Indian tertiary care centers highlights the need for reporting institutional experiences. This case series describes eight consecutive patients (age 45–70 years; 60% female) who underwent CAS at KG Hospital Center, Coimbatore. Clinical presentations included transient ischemic attack (n=2), stroke (n=4), giddiness (n=1), and incidental detection (n=1). Symptomatic patients had ipsilateral carotid stenosis ≥50%, while asymptomatic patients had stenosis ≥80%, diagnosed using NASCET angiographic criteria. Patients were enrolled based on conventional inclusion and exclusion criteria. Procedural success was achieved in 100% of cases, with no procedural complications. The 30-day major adverse cardiac or cerebrovascular events rate was 0%. New ipsilateral ischemic lesions at 48 hours were observed in 37% of patients, with an average lesion volume of 0.039 ± 0.08 cm³.This series demonstrates the feasibility and short-term safety of CAS as an alternative revascularisation strategy in selected patients within a real-world tertiary care setting.
Carotid artery stenosis, Carotid artery stenting (CAS), Ischemic stroke, Transient ischemic attack (TIA), Revascularisation
1. Introduction
Carotid artery stenosis is an important and preventable cause of ischemic stroke and transient ischemic attack [1]. Timely carotid revascularisation plays a key role in reducing the risk of recurrent neurologic events in both symptomatic and selected high-grade asymptomatic patients [2]. Carotid endarterectomy has traditionally been the standard treatment; however, carotid artery stenting has emerged as a minimally invasive alternative, particularly in patients who are poor surgical candidates or have high operative risk [3]. With advances in endovascular techniques, CAS is increasingly being performed worldwide, yet real-world data from Indian tertiary care centers remain limited [4]. Institutional experiences are valuable in assessing procedural feasibility, safety, and early clinical outcomes.
This case series was undertaken to report the clinical presentation and short-term results of carotid artery stenting in patients treated at a tertiary care hospital in South India.
2.1 Aim
To evaluate the feasibility, safety, and short-term clinical outcomes of carotid artery stenting in patients with symptomatic and asymptomatic carotid artery stenosis treated at a tertiary care center.
2.2 Objectives
To describe the clinical profile and presenting symptoms of patients undergoing carotid artery stenting.
3. Materials and methods
3.1 Study Design And Patient Selection
This single-center case series included eight consecutive patients who underwent carotid artery stenting (CAS) between 2021 and 2023 at KG Hospital Center, Coimbatore. Patients aged ≥18 years with de novo atherosclerotic carotid artery stenosis were eligible. Symptomatic patients had experienced transient ischemic attack or ischemic stroke within the preceding six months with ipsilateral carotid stenosis ≥50% [5]. It was assessed by angiography using NASCET criteria. Asymptomatic patients had carotid stenosis ≥80% deemed suitable for revascularisation by a vascular specialist and an independent neurologist[6].Patients with stage III renal insufficiency, acute stroke within 30 days, recent myocardial infarction (within 72 hours), atrial fibrillation, non-carotid causes of stroke, total carotid occlusion, severe circumferential calcification, lesion length >30 mm, or prior stent extension into the aortic arch were excluded.
3.2 Procedure Technique
All procedures were performed under standard protocol with embolic protection device (EPD) placement [7]. Temporary pacemaker insertion was routinely performed. Predilatation using a 2.5–3 mm balloon was performed when indicated, with atropine available for bradycardia. Self-expanding nitinol or Elgiloy stents were deployed to fully cover the lesion, extending from the common carotid artery to the internal carotid artery when necessary. Post-dilatation was performed selectively if residual stenosis resulted in a luminal diameter <5 mm. Following stent deployment, the EPD was removed and completion angiography was performed to assess residual stenosis and intracranial flow.
3.3 Outcome Measures
Primary outcomes included procedural success and peri-procedural complications [8]. Secondary outcomes included 30-day major adverse cardiac or cerebrovascular events and the incidence of new ipsilateral ischemic lesions detected at 48 hours.
4.1 Baseline Characteristics And Clinical Presentation
A total of eight patients underwent carotid artery stenting between 2021 and 2023. The mean age was approximately 61 years (range: 48–68 years). There were five females (62.5%) and three males (37.5%). Six patients (75%) were symptomatic at presentation with either stroke or transient ischemic attack. Stroke was the most common presentation, observed in four patients (50%), while two patients (25%) presented with recurrent or recent transient ischemic attacks. One patient presented with isolated upper limb weakness without documented infarct at presentation. Two patients (25%) presented with non-focal symptoms, including giddiness and headache.Comorbid conditions were common. Type 2 diabetes mellitus was present in three patients (37.5%), hypertension in two patients (25%), dyslipidemia in one patient (12.5%), and hypothyroidism in one patient (12.5%). Two patients had a prior history of cerebrovascular accident.Digital subtraction angiography demonstrated high-grade carotid stenosis in all cases, ranging from 70% to 99%. The right internal carotid artery involved five patients (62.5%), while left-sided lesions were noted in three patients (37.5%).
4.2 Case Summaries
Table 1: Clinical Characteristics and Outcomes of the Reported Case(s)

Figure 1: Case 1 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 90% stenosis of left ICA. right: Post-stenting angiogram showing good flow across the stent.
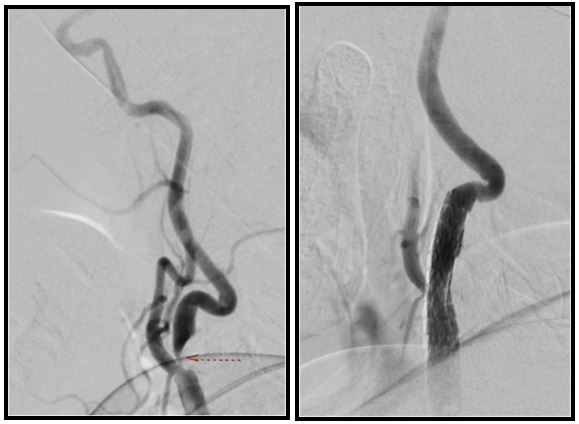
Figure 2: Case 2 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 99% stenosis of left ICA. right: Post-stenting angiogram showing good flow across the stent.
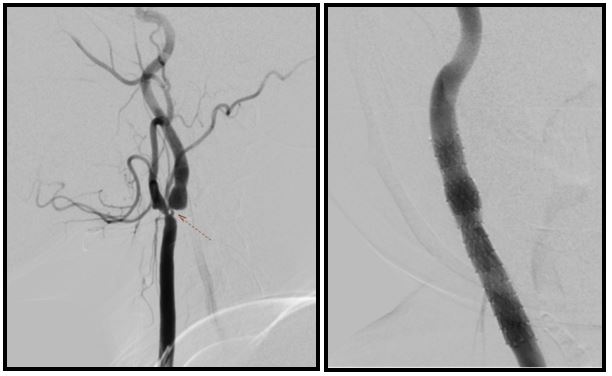
Figure 3: Case 3 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 90% stenosis of right ICA. right: Post-stenting angiogram showing restoration of flow.
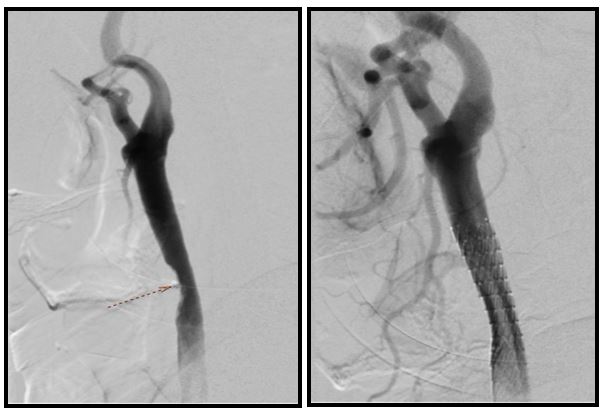
Figure 4: Case 4 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 70% stenosis of left CCA. right: Post-stenting angiogram showing good luminal patency.

Figure 5: Case 5 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 70–80% stenosis of right ICA. right: Post-stenting angiogram showing satisfactory flow.
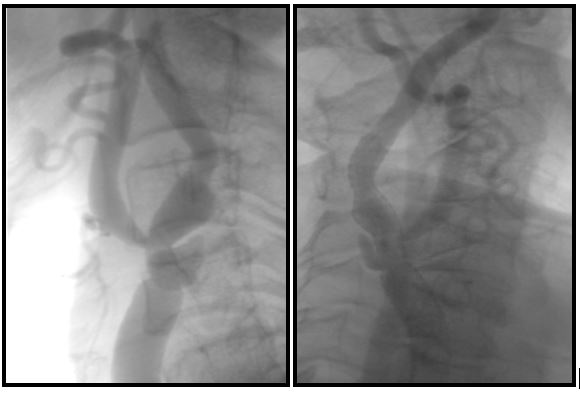
Figure 6: Case 6 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 80% stenosis of right ICA. right: Post-stenting angiogram showing good distal perfusion.
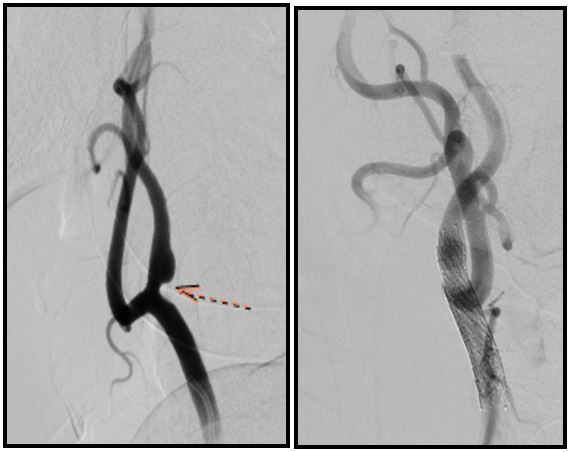
Figure 7: Case 7 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 70% stenosis of right ICA. right: Post-stenting angiogram showing adequate revascularisation.

Figure 8: Case 8 – Pre- and Post-Stenting Images left: Pre-stenting DSA showing 70–80% stenosis of right CCA/ICA. right: Post-stenting angiogram showing good flow across the stent.
5. Discussion
Stroke remains a major global health burden and is a leading cause of long-term disability. Significant carotid artery stenosis contributes to nearly 20–25% of ischemic strokes, making timely revascularisation crucial in selected patients. Carotid endarterectomy (CEA) has long been regarded as the standard of care for symptomatic stenosis >50% and asymptomatic stenosis >60%[9]. However, over the past two decades, carotid artery stenting (CAS) has evolved considerably as a less invasive alternative to carotid endarterectomy and medical management [10].
Early trials evaluating CAS, including the Wallstent study (2001) and CAVATAS (2001), reported relatively higher 30-day stroke and death rates. Subsequent landmark trials such as SPACE (2006), EVA-3S (2006), ICSS (2009), and CREST (2010) demonstrated progressive improvement in outcomes, with 30-day combined stroke and death rates declining to approximately 6–9% in symptomatic and average-risk patients. Notably, CREST also included asymptomatic patients and showed comparable long-term outcomes between CAS and CEA [11]. This trend reflects advances in stent design, embolic protection devices, operator experience, and improved patient selection.
In our case series, procedural success was achieved in all patients, with no peri-procedural complications and a 0% 30-day major adverse cardiac or cerebrovascular event rate. Although new ipsilateral ischemic lesions were detected on early imaging in a subset of patients, these were small in volume and clinically silent. These findings are consistent with contemporary data suggesting improved safety profiles of CAS in experienced centers [12].
6. Conclusion
Carotid artery stenting demonstrated high procedural success and excellent short-term safety in our case series.No major peri-procedural or 30-day adverse cerebrovascular events were observed.These findings are consistent with improving outcomes reported in contemporary literature.In appropriately selected patients, CAS represents a safe and effective revascularisation strategy.It may serve as a viable alternative to carotid endarterectomy in experienced centers.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org