International Journal of Clinical Cardiology and Cardiovascular Interventions
OPEN ACCESS | Volume 4 - Issue 1 - 2025
ISSN No: 2836-2837 | Journal DOI: 10.61148/2836-2837/IJCCI


Hammaad Khalid1, Bilal Sait1, Mubashira Fatima2, Abdullah Shehzad3, Azeem S Sheikh1*
1Calderdale & Huddersfield NHS Foundation Trust, Halifax. HX3 0PW. UK.
2Royal Preston Hospital, Preston. PR2 9HT. UK.
3Lahore Grammar School JT, Lahore.
*Corresponding author: Azeem S Sheikh, Consultant Interventional Cardiologist, Calderdale & Huddersfield NHS Foundation Trust Halifax.HX3 0PW, United Kingdom.
Received: May 15, 2026 | Accepted: May 09, 2026 | Published: June 01, 2026
Citation: Khalid H, Sait B, Fatima M, Shehzad A, Azeem S Sheikh., (2026) “Multimodality Imaging in the Diagnosis of Constrictive Pericarditis Mimicking Heart Failure with Preserved Ejection Fraction: A Case Report.” International Journal of Clinical Cardiology and Cardiovascular, 6(1). DOI: 10.61148/2836-2837/IJCCCI/225.
Copyright: © 2026 Azeem S Sheikh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Constrictive pericarditis is an uncommon but important cause of heart failure characterised by pericardial fibrosis and calcification leading to impaired ventricular filling. Clinical presentation is often non-specific and may mimic heart failure with preserved ejection fraction (HFpEF), resulting in delayed diagnosis.
We report the case of an elderly patient presenting with exertional dyspnoea, peripheral oedema, and intermittent chest pain, initially managed as HFpEF. In view of exertional chest pain, invasive coronary angiography was performed to exclude obstructive coronary artery disease and revealed extensive pericardial calcification on fluoroscopy. This prompted further evaluation with cardiac magnetic resonance imaging and computed tomography, which confirmed constrictive physiology.
This case highlights the importance of maintaining clinical suspicion and demonstrates the diagnostic value of multimodality imaging, particularly when incidental findings on invasive imaging alter the diagnostic pathway.
Constrictive pericarditis; HFpEF; cardiac MRI; cardiac CT; septal bounce; pericardial calcification
1. Introduction
Constrictive pericarditis (CP) is a chronic inflammatory condition characterised by progressive pericardial fibrosis, thickening, and often calcification, which results in loss of normal pericardial elasticity and impaired ventricular filling. The resulting ventricular interdependence and dissociation between intrathoracic and intracardiac pressures lead to characteristic haemodynamic abnormalities and predominantly diastolic heart failure. [1]
Despite advances in cardiovascular imaging, CP remains diagnostically challenging because its clinical presentation frequently overlaps with other causes of heart failure with preserved ejection fraction (HFpEF), particularly restrictive cardiomyopathy. [1] Symptoms such as exertional dyspnoea, fatigue, and signs of systemic venous congestion are non-specific and may delay recognition. Early identification is crucial, however, as CP represents a potentially reversible cause of heart failure when treated appropriately, most commonly with pericardiectomy.
2. Case Report
2.1 Clinical Presentation
An 80-year-old man was referred for cardiology evaluation following an episode of exertional chest pain that occurred while walking uphill several weeks prior to presentation. He also reported progressively worsening exertional dyspnoea and increasing peripheral oedema over the preceding two months.
On examination, he appeared dyspnoeic with elevated jugular venous pressure and marked peripheral and sacral oedema. He was clinically in New York Heart Association (NYHA) class II heart failure and was admitted for further evaluation.
His past medical history was notable for atrial fibrillation. He was a lifelong non-smoker, consumed alcohol only occasionally, and remained independent in activities of daily living.
On admission, vital signs included a blood pressure of 128/72 mmHg, heart rate of 56 beats per minute with an irregular rhythm, oxygen saturation of 96% on room air, and he was afebrile. His medications included rate-controlling therapy for atrial fibrillation.
Laboratory investigations, including B-type natriuretic peptide (BNP), were within normal limits. Notably, the absence of elevated natriuretic peptide levels in the presence of clinically apparent right-sided heart failure raised suspicion for an alternative diagnosis to heart failure with preserved ejection fraction.
2.2 Echocardiography
Transthoracic echocardiography was technically challenging due to limited acoustic windows. Left and right ventricular systolic function were preserved. Abnormal interventricular septal motion with early diastolic septal shift suggestive of ventricular interdependence was observed (Figure 1).
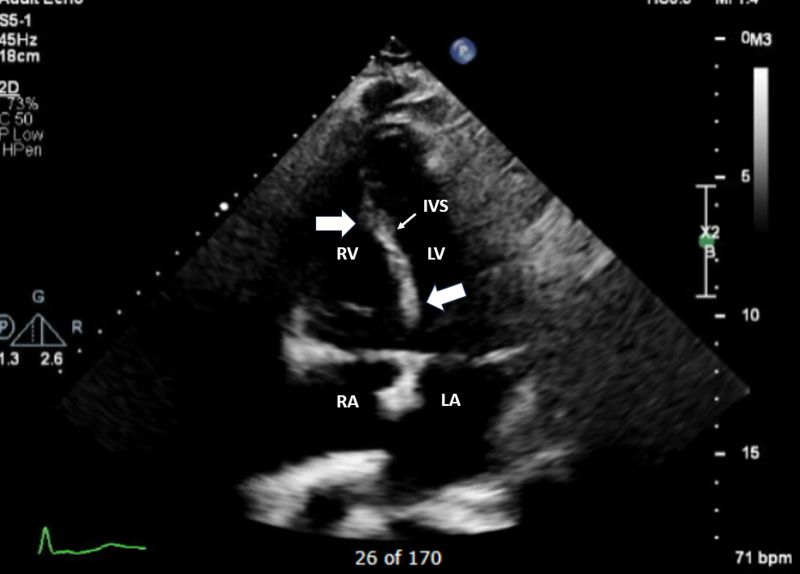
Figure 1: Transthoracic echocardiography demonstrating early diastolic septal bounce (thick white arrows) consistent with ventricular interdependence. LV left ventricle, RV right ventricle, LA left atrium, RA right atrium, IVS interventricular septum.
The inferior vena cava was dilated with reduced respiratory variation, consistent with elevated right atrial pressure. No significant valvular abnormalities were identified.
A provisional diagnosis of heart failure with preserved ejection fraction was considered, and diuretic therapy was initiated. Electrocardiography demonstrated atrial fibrillation with a slow ventricular response (56 beats per minute) and no evidence of acute ischaemic changes.
2.3 Coronary Angiography
In view of the patient’s history of exertional chest pain and advanced age, invasive coronary angiography was performed to exclude obstructive coronary artery disease as a potentially reversible cause of symptoms.
Although non-invasive imaging such as CT coronary angiography may be considered in selected patients, invasive angiography was chosen in this case because of the patient’s presenting symptoms, the need for definitive anatomical assessment, and local clinical practice.
Coronary angiography demonstrated unobstructed epicardial coronary arteries. However, fluoroscopic imaging revealed extensive curvilinear calcification outlining the cardiac silhouette [Figure 2]. This finding raised strong suspicion of chronic calcific pericardial disease and prompted further dedicated imaging.
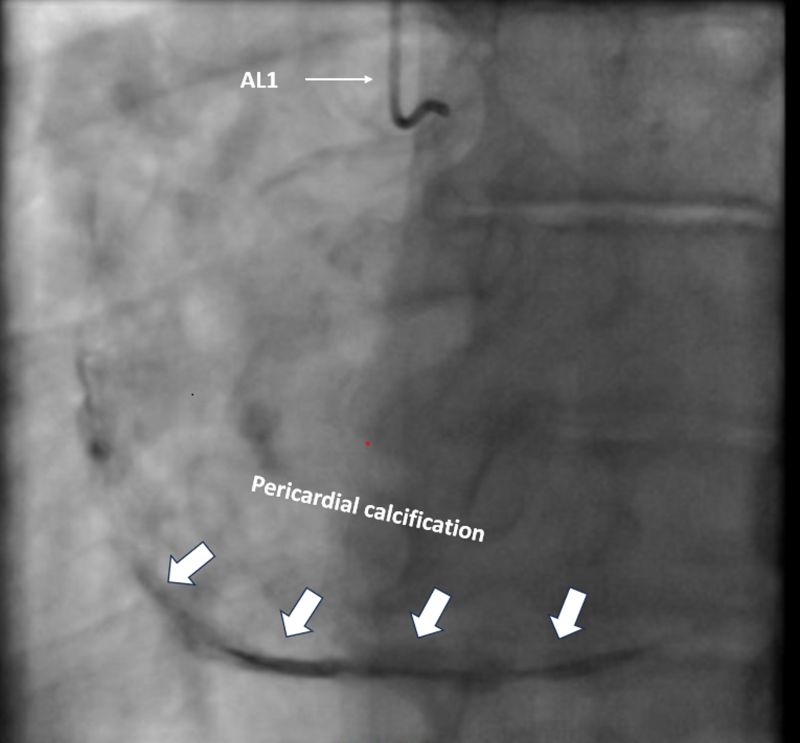
Figure 2: Fluoroscopic image during coronary angiography demonstrating extensive curvilinear pericardial calcification outlining the cardiac silhouette (thick white arrows). AL1 Amplatz left 1 diagnostic catheter.
2.4 Cardiac Magnetic Resonance Imaging
Cardiac magnetic resonance (CMR) imaging demonstrated preserved biventricular systolic function. Steady-state free precession cine sequences showed early diastolic septal bounce (Figure 3, Video 1) and exaggerated ventricular interdependence. Pericardial thickening was also noted.
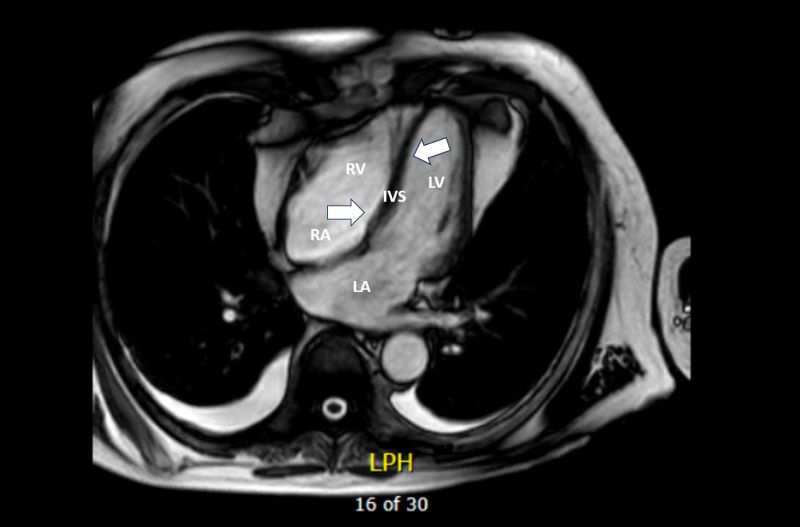
Figure 3: Cardiac magnetic resonance cine imaging (SSFP sequence) demonstrating early diastolic septal bounce (thick white arrows), a hallmark of constrictive physiology with preserved biventricular systolic function. (Dynamic cine clips have been submitted as supplementary material to illustrate ventricular interdependence.)
LV left ventricle, RV right ventricle, LA left atrium, RA right atrium, IVS interventricular septum.
Late gadolinium enhancement imaging revealed a focal inferolateral non-ischaemic myocardial scar consistent with prior myocarditis, without evidence of active myocardial inflammation.
2.5 Computed Tomography
Computed tomography of the thorax demonstrated diffuse circumferential pericardial thickening with dense calcification encasing the cardiac chambers. The maximum pericardial thickness was measured at 7.0 mm [Figure 4], consistent with significant chronic pericardial disease.
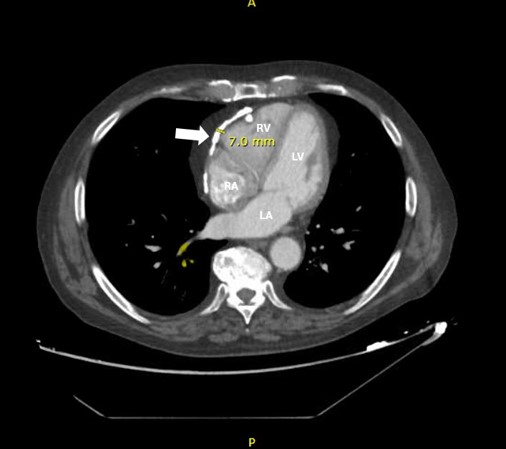
Figure 4: Cardiac CT (axial view) demonstrating diffuse circumferential pericardial thickening with dense calcification (thick white arrow), confirming chronic constrictive pericardial disease. LV left ventricle, RV right ventricle, LA left atrium, RA right atrium.
Based on the clinical presentation and multimodality imaging findings, a diagnosis of constrictive pericarditis was established. No clear underlying aetiology was identified.
Following multidisciplinary team discussion, treatment options—including surgical pericardiectomy and conservative management—were considered. Given the patient’s advanced age and estimated surgical risk, he opted for conservative medical management. Invasive haemodynamic assessment with right heart catheterisation was therefore not pursued.
The patient was discharged on bumetanide 3 mg daily and spironolactone 37.5 mg daily. At six-week follow-up, his dyspnoea had improved, although peripheral oedema persisted. Metolazone 2.5 mg on alternate days was subsequently initiated to optimise diuretic therapy.
3. Discussion
Constrictive pericarditis (CP) is an uncommon but important cause of heart failure in developed countries, accounting for fewer than 0.5% of cases of heart failure presentations. The aetiology is heterogeneous and includes idiopathic disease, prior cardiac surgery, mediastinal radiation therapy, and infectious causes, particularly tuberculosis in endemic regions. [2,5] Despite advances in imaging and clinical recognition, CP remains diagnostically challenging because its clinical manifestations frequently overlap with other forms of heart failure, particularly heart failure with preserved ejection fraction (HFpEF).
The fundamental pathophysiological feature of CP is the presence of a rigid, non-compliant pericardium that restricts normal diastolic expansion of the cardiac chambers. This leads to impaired ventricular filling, dissociation between intrathoracic and intracardiac pressures, and exaggerated ventricular interdependence. Consequently, ventricular filling becomes limited and cardiac output may be reduced, while systemic venous congestion results in clinical features predominantly related to right-sided heart failure, including peripheral oedema, ascites, and elevated jugular venous pressure. [6]
Accurate diagnosis requires careful integration of clinical findings with multimodality imaging. [4,7,8] Transthoracic echocardiography is usually the initial imaging modality and may demonstrate characteristic findings such as abnormal interventricular septal motion (“septal bounce”), respiratory variation in transvalvular flow velocities, and features suggesting elevated right atrial pressure. [6,9] However, echocardiography alone may not always provide definitive diagnostic information, particularly in patients with limited acoustic windows or atypical haemodynamic features. [7,8]
Advanced imaging modalities therefore play a central role in the evaluation of suspected constrictive physiology. Cardiac magnetic resonance (CMR) provides detailed assessment of pericardial morphology and ventricular interaction, enabling visualisation of septal bounce, respiratory variation in ventricular filling, and ventricular interdependence. In addition, CMR allows assessment of myocardial tissue characteristics and can identify concomitant myocardial disease, which is important in differentiating constrictive pericarditis from restrictive cardiomyopathy. [10,11] As highlighted in recent reviews of pericardial imaging, CMR has emerged as a powerful non-invasive tool for characterising pericardial disease and evaluating associated myocardial pathology. [3,6]
Computed tomography (CT) provides excellent spatial resolution for anatomical assessment of the pericardium and is particularly sensitive for detecting pericardial thickening and calcification. CT is therefore especially valuable in chronic calcific pericarditis, where dense circumferential calcification may be readily demonstrated. Contemporary multimodality imaging strategies integrating echocardiography, CMR, and CT have significantly improved the diagnostic accuracy of CP while reducing the need for invasive haemodynamic assessment in many patients. [3]
Distinguishing constrictive pericarditis from heart failure with preserved ejection fraction (HFpEF) remains a common clinical challenge because both conditions may present with similar symptoms of exertional dyspnoea and systemic venous congestion. However, certain clinical and biochemical features may aid differentiation. In patients with CP, natriuretic peptide levels are often normal or only mildly elevated despite significant clinical congestion, reflecting the relatively preserved myocardial wall stress compared with myocardial causes of heart failure. In contrast, HFpEF is typically associated with elevated natriuretic peptide concentrations. Imaging findings such as septal bounce, exaggerated ventricular interdependence, and dissociation between intrathoracic and intracardiac pressures are characteristic of constrictive physiology and help distinguish CP from myocardial disease. [3,12]
Management of CP should be individualised according to symptom severity, comorbidities, and operative risk. In patients with mild symptoms or significant comorbid conditions that increase surgical risk, conservative treatment with diuretics may provide symptomatic relief by reducing systemic congestion. [12] However, medical therapy does not address the underlying mechanical constraint imposed by the diseased pericardium. For patients with advanced symptoms and acceptable surgical risk, pericardiectomy remains the definitive treatment and can lead to substantial haemodynamic and symptomatic improvement. [13]
The present case highlights the clinical challenges encountered when managing elderly patients with CP. In this instance, the patient elected conservative therapy because of advanced age and perceived operative risk. Although medical therapy improved symptoms, the underlying constrictive physiology remained untreated, and careful clinical follow-up was required.
An additional noteworthy aspect of this case is the incidental identification of extensive pericardial calcification during invasive coronary angiography performed to evaluate suspected coronary artery disease. Fluoroscopic recognition of extra-coronary findings, such as curvilinear pericardial calcification outlining the cardiac silhouette, can provide an important diagnostic clue. In this patient, the angiographic observation prompted further targeted multimodality imaging that ultimately established the diagnosis of CP. This emphasises the importance of maintaining diagnostic vigilance and recognising extracardiac and extra-coronary findings during invasive procedures
Overall, this case highlights the growing importance of multimodality imaging in the evaluation of suspected constrictive pericarditis. Integrating echocardiography, CMR, and CT allows comprehensive non-invasive assessment of both pericardial anatomy and cardiac physiology, facilitating accurate diagnosis even in complex or atypical presentations. [3,4,6]
4. Conclusions
Constrictive pericarditis is an uncommon but clinically important and potentially treatable cause of heart failure that may mimic HFpEF. Accurate diagnosis requires a high index of suspicion and careful integration of clinical findings with multimodality imaging. Echocardiography, cardiac magnetic resonance, and computed tomography provide complementary information regarding pericardial structure and constrictive physiology.
Although diuretic therapy may provide symptomatic relief in selected patients, surgical pericardiectomy remains the only definitive treatment. Patients managed conservatively require careful follow-up due to the persistent underlying constrictive pathology.
5. Key Learning Points
6. Abbreviations:
AL1: Amplatz Left 1
CMR: Cardiac Magnetic Resonance Imaging
CP: Constrictive pericarditis
CT: Computed tomography
HFpEF: Heart Failure with preserved Ejection Fraction
IVS: Interventricular septum.
LA: Left atrium,
LV: Left ventricle
NYHA: New York Heart Association
RA: Right atrium,
RV: Right ventricle
SSFP: Steady-state free precession
7. Declarations
Authors’ contributions
ASS, HK, BS: Conceptualization, Writing—original draft, Writing—review & editing. ASS, HK, BS: Writing—original draft, Writing—review & editing. ASS, HK, BS, MF, AS: Writing—review & editing. All authors read and approved the submitted version.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Ethical approval
The study was conducted in accordance with institutional guidelines and the principles of the Declaration of Helsinki. A formal ethical approval was not required for this retrospective case report.
Consent to participate
Informed consent to participate in the study was obtained from the patient.
Consent to publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding Statement
This research work did not receive any external funding.
Availability of Data and Materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of generative AI and AI-assisted technologies in the writing process
The authors declare that ChatGPT was used solely to assist with language editing and improving clarity of expression. The tool was not used to generate scientific content, analyse data, or develop conclusions. All intellectual contributions are entirely those of the authors. The manuscript was carefully reviewed and revised by the authors, who take full responsibility for its content and integrity.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org