International Journal of Clinical Cardiology and Cardiovascular Interventions
OPEN ACCESS | Volume 4 - Issue 1 - 2025
ISSN No: 2836-2837 | Journal DOI: 10.61148/2836-2837/IJCCI


Ben Khemis A*., Mesrati M., Daoued Z., Ziadi J., Ben Mrad M., Denguir R
Department of Cardiovascular Surgery, La Rabta Hospital, Tunis, Tunisia.
*Corresponding author: Asma Ben Khemis, Department of Cardiovascular Surgery, La Rabta Hospital, Tunis, Tunisia.
Received: February 01, 2026 | Accepted: February 09, 2026 | Published: February 12, 2026
Citation: Ben Khemis A., Mesrati M., Daoued Z., Ziadi J., Ben Mrad M., Denguir R., (2026) “Surgical Repair of Abdominal Aortic Aneurysm Associated with a Congenital Pelvic Kidney: A Challenging Case Report.” International Journal of Clinical Cardiology and Cardiovascular, 5(1). DOI: 10.61148/2836-2837/IJCCCI/223.
Copyright: © 2026 Asma Ben Khemis. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: The coexistence of an abdominal aortic aneurysm (AAA) and an ectopic pelvic kidney is an extremely rare and surgically challenging condition, due to the aberrant renal vascular anatomy and the risk of renal ischemia during aortic clamping.
Case Presentation: We report the case of a 73-year-old male with a symptomatic infrarenal AAA (89 mm) extending to the iliac arteries, associated with a right ectopic pelvic kidney perfused by the internal iliac artery. Open repair with a bifurcated Dacron graft was performed, including reimplantation of the right renal artery and inferior mesenteric artery. Renal protection was achieved using Custodiol® cold perfusion. The postoperative course was uneventful, and the patient was discharged on postoperative day 5 with preserved renal function.
Conclusion: AAA repair in the setting of an ectopic pelvic kidney requires careful preoperative planning and intraoperative renal protection strategies. Open and endovascular approaches have both been described, but the choice depends on anatomical feasibility and institutional expertise.
abdominal aortic aneurysm; ectopic pelvic kidney; Congenital Pelvic Kidney
Congenital pelvic kidney represents the rarest form of renal ectopia, resulting from a failure of renal ascent during embryogenesis beyond the fourth gestational week. Its incidence is estimated at approximately 1 in 2,200 to 1 in 3,000 autopsies. Aberrant renal vasculature is common, with arteries arising from the distal aorta, iliac bifurcation, or iliac arteries. The association with abdominal aortic aneurysm (AAA) is exceedingly rare and poses a surgical challenge, as renal perfusion must be preserved during aneurysm repair.
Case Report
A 73-year-old man with a history of nephrolithiasis presented with abdominal pain. Computed tomography angiography (CTA) demonstrated an 89 mm infrarenal AAA extending to the iliac arteries, with the left iliac artery measuring 32 mm and the right iliac artery 27 mm. An ectopic right pelvic kidney was identified, perfused by the right internal iliac artery. Baseline renal function was preserved, with creatinine clearance at 54.7 ml/min/1.73m².
An open surgical repair was planned. Through a midline laparotomy, the proximal infrarenal aortic neck, inferior mesenteric artery, right renal artery, and bilateral iliac arteries were isolated.
Aortic and iliac cross-clamping was performed, with renal protection achieved by selective perfusion of the right renal artery using Custodiol® solution. A bifurcated Dacron graft (18-9-9) was implanted from the proximal infrarenal aorta to the common iliac arteries. An endarterectomy of the right renal artery ostium was performed before reimplantation into the graft, followed by reimplantation of the inferior mesenteric artery and ligation of the aneurysmal internal iliac arteries. The postoperative course was uneventful. The patient was discharged on day 5 with normal renal function, and a one-month follow-up CTA demonstrated satisfactory graft patency.
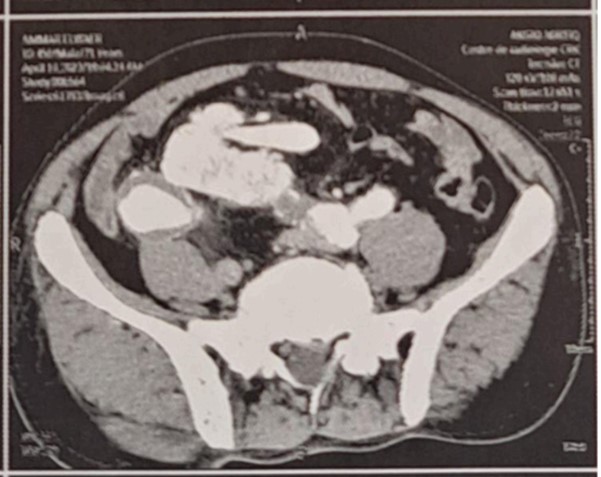
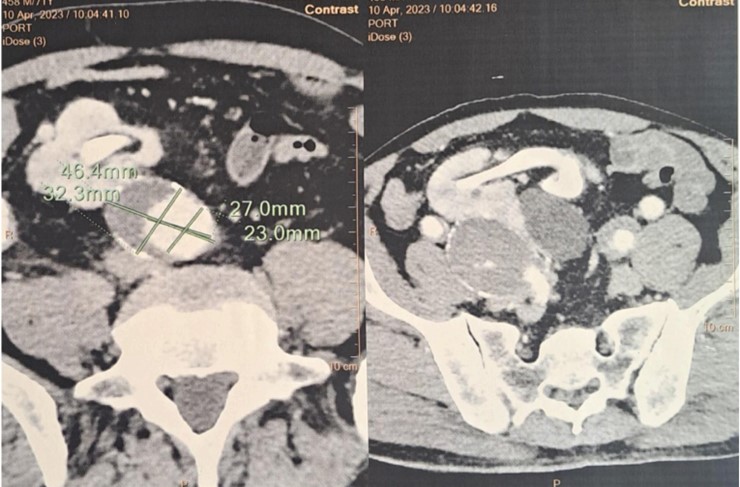
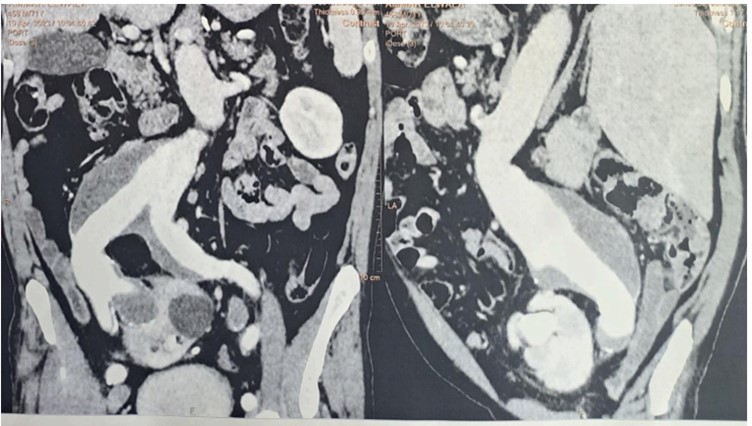
Figure: Computed tomography angiography (CTA) demonstrated an 89 mm infrarenal AAA extending to the iliac arteries, with the left iliac artery measuring 32 mm and the right iliac artery 27 mm. An ectopic right pelvic kidney was identified, perfused by the right internal iliac artery.
Discussion
Pelvic kidney is a rare congenital anomaly resulting from a failure of normal renal ascent during embryogenesis, typically occurring after the fourth gestational week [1]. Its prevalence is estimated at 1 in 2,200 to 3,000 live births, with most cases being asymptomatic and discovered incidentally during imaging for unrelated conditions [2]. The anomaly is often associated with a shorter ureter, which increases the risk of urinary tract infections, hydronephrosis, and lithiasis [1,2]. Aberrant vascularization is characteristic of pelvic kidneys, with renal arteries originating from the distal aorta, the aortic bifurcation, or the iliac arteries, and frequently multiple arteries supply a single kidney [1,2]. Such anatomic variations have significant surgical implications, particularly in the context of abdominal aortic aneurysm (AAA) repair.
The coexistence of AAA and a pelvic kidney is exceedingly rare, with fewer than 40 cases reported in the literature [3]. The pelvic location of the kidney, combined with its unusual vascular supply, poses unique technical challenges during aortic surgery. The primary concern is maintaining renal perfusion during cross-clamping of the aorta, as ischemic injury can result in acute kidney injury (AKI) with subsequent long-term functional impairment [2,4]. The rarity of this scenario has precluded the development of standardized surgical guidelines, and management strategies must be individualized based on patient anatomy, aneurysm characteristics, and institutional expertise [3,5].
Open Surgical Repair
Open repair remains the most commonly reported approach for AAA in patients with a pelvic kidney, especially when the aneurysm involves the aortic bifurcation or when the renal arteries are unsuitable for endovascular access [3,6]. Techniques for renal protection are critical during aortic cross-clamping and include:
Selective Cold Perfusion: This involves perfusing the renal artery with cold crystalloid solutions (commonly 4°C Ringer lactate) to reduce metabolic demand and protect renal tissue from ischemia [3,6].
Temporary Shunts: Shunts, typically from the axillary artery or constructed from the body of the graft during distal anastomosis, allow continuous perfusion of the pelvic kidney [2].
Custodiol® Solution: Originally developed for myocardial protection in cardioplegia, Custodiol® has demonstrated superior renal protection compared to cold Ringer lactate in comparative studies. Tshomba et al. reported improved perioperative renal function with Custodiol® during thoracoabdominal aortic aneurysm repair [4].
During open repair, reimplantation of aberrant renal arteries may be necessary to ensure adequate perfusion. The inferior mesenteric artery and internal iliac arteries can also be involved, and careful planning is required to minimize ischemic complications [3,6].
Endovascular Repair
Endovascular repair (EVAR) offers a minimally invasive alternative, but it is technically demanding in the context of pelvic kidneys due to aberrant renal artery anatomy. Fenestrated or branched stent-grafts, chimney EVAR, or hybrid ilio-renal bypass techniques have been described in the literature [5,6,8,9]. Fenestrated EVAR allows precise incorporation of aberrant renal arteries into the stent-graft design, whereas chimney grafts provide parallel perfusion of the pelvic kidney. Hybrid techniques, combining surgical bypass with endovascular exclusion of the aneurysm, have been successfully reported, reducing the need for extensive open dissection [6,9].
Patient selection for EVAR depends on the specific vascular anatomy, aneurysm morphology, and institutional experience. Endovascular strategies can reduce operative time, blood loss, and postoperative complications; however, the long-term durability in the context of aberrant renal arteries remains under investigation [8,9].
The most frequently reported complication is acute kidney injury, reflected by transient elevations in serum creatinine and reduced glomerular filtration rate [3,4]. Other potential complications include graft thrombosis, ischemic colitis, and lower limb ischemia if iliac arteries are ligated [3,6]. Careful intraoperative planning, including selective perfusion and arterial reimplantation, has been shown to mitigate renal injury. Long-term outcomes are generally favorable when renal protection strategies are appropriately applied [2,3].
A review of 37 reported cases of AAA with pelvic kidney highlights that open repair with renal protection remains the most common approach, while endovascular techniques are increasingly utilized in selected patients with suitable anatomy [3,5]. Custodiol® solution has emerged as a preferred renal perfusion solution due to its superior preservation of renal function [4]. No standardized guideline exists, emphasizing the importance of individualized treatment planning, multidisciplinary discussion, and preoperative imaging, including CT angiography and 3D reconstruction, to define renal and aneurysmal anatomy [2,5,8].
Conclusion
The coexistence of AAA and congenital pelvic kidney represents a rare but challenging surgical scenario. Open repair with meticulous renal protection remains the standard in many centers, whereas endovascular approaches are feasible in selected cases with favorable anatomy. Preservation of renal function is the primary surgical goal, and perioperative strategies—including selective cold perfusion, Custodiol® solution, temporary shunts, and careful reimplantation of aberrant arteries—are critical to optimizing outcomes. Future studies and multicenter registries are needed to establish standardized approaches and improve evidence-based recommendations for this complex clinical entity.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org