Clinical Psychology and Mental Health Care
OPEN ACCESS | Volume 7 - Issue 1 - 2025
ISSN No: 2994-0184 | Journal DOI: 10.61148/2994-0184/CPMHC


P. D. Garg 1*, Sandeep Bhola 2, Manmeet Kaur 3, Amarbirpal Singh 4, Aseem Garg 5, Aman Sood 6, Raminder Sidhu 7
1 Professor, Dept. of Psychiatry, Govt. Medical College, Amritsar
2 Consultant Psychiatrist, Civil Hospital, Kapurthala
3 Senior Resident, Dept. of Psychiatry, Govt. Medical College, Amritsar
4 Consultant Psychiatrist, Institute of Mental Health, Amritsar
5 Consultant Psychiatrist, Sankalp Drug De-addiction and Treatment Centre.
6 Assistant Professor, Dept. of Psychiatry, Govt. Medical College Amritsar
7 Clinical Psychologist, Dept. of Psychiatry, Govt. Medical College, Amritsar
*Corresponding Author: Parshotam Dass Garg, Professor, Dept. of Psychiatry, Govt. Medical College, Amritsar
Received: February 18, 2021
Accepted: February 22, 2021
Published: February 26, 2021
Citation: P. D. Garg, Bhola S, Kaur M, Singh A, Garg A. “Experience and Evaluation of Five Day Ooat (Outpatient Opioid Assisted Treatment) Training Programs of Health Care Staff for Establishments of OOAT Clinics in Punjab.’’. Clinical Psychology and Mental Health Care, 2(3); DOI: http;//doi.org/03.2021/1.10017.
Copyright: © 2021 Parshotam Dass Gargi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Background: Punjab has a huge population of opioid dependent patients and they are clearly a major public health concern. To deal with this, it is crucial to strengthen the treatment services for opioid dependent people. Aims: Among the suggested strategies to tackle the problem of opioid dependence in Punjab, substitution therapies are most common. The aim of this study is to assess the impact of training program and change in knowledge among participants receiving five-day training for establishments of OOAT clinics in various districts of Punjab. Materials and methods: For this study “pre-test post-test” design was used. Routine data was collected from staff who underwent five-day training regarding OOAT in 19 different batches and was analyzed. The staff comprises of doctors (224), staff nurses (256), counsellors (91), data entry operator (106), pharmacist (83), lab technicians (17) and other staff (21). In the beginning of training, every Monday of the week pre-test was given and after completion of training program, on Friday of the week post-test (20 questions) was administered. Evaluation sheet was provided to the participants at the end of training to give feedback regarding usefulness of all the sessions and answer comprise out of four options: useful, can’t say, not useful and any remarks. Overall scores were compared using appropriate statistical method. Findings: The difference between the percentage of correct questions answered between pre-test and post-test was significant. Conclusion: The five-day training program was effective to improve the knowledge among health care staff and their attitudes towards opioid dependents.
Introduction
The use of opioids in the state of Punjab has reached in epidemic proportions. Various studies in Punjab show opioid dependence as a major public health concern. Punjab Opioid Dependence Survey (PODS) was conducted by Society for Promotion of Youth and Masses (SPYM) in collaboration with National Drug Dependence and Treatment Centre (NDDTC AIIMS) in collaboration with Department of Health and Family Welfare Government of Punjab. The main aim of survey was to estimate the size of opioid dependent population in the entire state of Punjab. The following findings were presented to Department of Health in Punjab in 2015.
1. Most common opioid drug: Heroin (53%)
2.Injecting drug user: 33%
3. Most common reason for starting opioid use: peer influence (75%)
4. Ever tried to quit: 80%
5. Ever received any help for quitting: 33%
6. 2.3 lakh opioid dependent individuals
7. Probable 8.6 lakh opioid users
8.Young males disproportionately affected
9. Estimated annual expenditure on opioid drugs by dependent individuals: Rs. 75,75 crores.[1]
Second study was conducted by PGIMER Chandigarh in 2016-2017 entitled “Epidemiology of Substance Abuse and Dependence in the state of Punjab.” The findings of survey were
Agonist maintenance treatment with opioids (commonly referred to as opioid substitution therapy OST in India) has displayed better outcomes compared with other existing treatment strategies. OST helps in retaining the patient in treatment, reducing the use of illicit opioids and other substances and in improving the individual’s productivity and his/her quality of life.[3] Current number of OST centres in state of Punjab is 29. These OST centres are functional through the support of NACO (National AIDS control organization) and Punjab State Aids Control Society (PSACS) give harm reduction services only for injecting drug users for HIV prevention.[4] The prevalence of unsafe injecting remains high despite the increase in availability of needle/syringe programs, and there is urgent need for countries to expand the implementation of evidence based drug treatment interventions and make full use of all therapeutic options for managing drug dependence and reducing harms from injecting.[5] So Punjab Government and anti-drug Special Task Force (STF) launched a pilot project to start OOAT (Outpatient Opioid Assisted Treatment) centres for injecting and non-injecting opioid dependent persons in the state which requires adequately trained human resources.
Human resources are often limited in drug treatment agencies and ideal staffing are seldom achieved. Efficient staffing profiles should reflect the diversity of the patient population and treatment setting and make effective use of each member of the treatment team. Trained nursing staff or doctor’s assistants can attend to the screening of patients for injection-related injuries, blood-borne virus infections and STIs. They can also assist with substitution treatment dosing. Social workers and other allied health staff are a very useful component of a treatment team and can provide counselling and other psychosocial interventions. Peer educators and peer counsellors can provide an important bridge between health professionals and patients. Patients often listen to their peer than to clinicians and so health professionals need to also develop good relationship with peer workers.[5]
AIIMS study of evaluation of a five-day training program on opioid substitution therapy in India showed that a period of five days is sufficient to improve the knowledge and attitude of participants immediately after training. All the cadres in this study showed improvement in post test scores, demonstrating that it is possible to train different cadres together even on the specialized topic of OST. This study also shows that doctors may benefits more as compared to other cadres. The study demonstrated improvement in the participant’s knowledge as well attitude towards Intravenous Drug Users (IDUs).[6]
Outpatient Opioid Assisted Treatment(OOAT) is safe, efficacious and cost effective dual model approach for the management of opioid dependent patients. It combines positive of two models: harm reduction approach and abstinence based approach. Harm reduction approach includes the use of buprenorphine-naloxone combination to retain the patients. Abstinence based approach involve counselling and peer support aimed at whole person recovery. OOAT clinics are located within/ linked to public health setting. Five stages of treatment under OOAT clinic include induction phase, stabilization phase, maintenance phase, termination and follow up phase. It is based on concept of OST centres but different in some perspectives like in OOAT clinic both injecting as well as non-injecting opioid dependent persons will be treated, there is a provision of urine testing in OOAT clinics and in OOAT clinics buprenorphine-naloxone combination is given instead of plain buprenorphine given in OST centres which reduces the diversion rates in OOAT centres. Staff in OOAT centres will comprise of medical officer, staff nurse, counsellor, data entry operator, peer support group and support staff.[7]
The responsibility to train the staff for implementation of OOAT program was entrusted to Psychiatry Department Medical College Amritsar. The financial resources were provided by government of Punjab. The human resources were three master trainers of NACO including the author and technical support unit of Punjab State Aids Control Society. The aim of the study is to assess the impact of five-day OOAT training program on knowledge and attitude of staff participating. Additionally, evaluation sheet was provided to the participants at the end of training to give feedback on the entire training program.
Materials and methods
The study followed a “pre-test post-test” design, evaluation sheet and used routine data collected as part of carrying out the OOAT training program.
Details of OOAT training
The OOAT training was conducted in batches of 30- 70 participants who belong to various government health centres of different districts of Punjab and includes medical officers, staff nurses, counsellors and other staff who are trained together in a residential program of five days. First batch was trained from 17 July 2017 to 21 July 2017. Five-day training program included four and half day classroom training in Government Drug Rehabilitation Centre Amritsar and half day visit to OST center and Swami Vivekananda De-addiction and Treatment Centre. The various sessions in classroom training were according to training manual prepared for this purpose. The various sessions includes overview of drugs and drug use disorders, drug related problems and harms, local drug abuse scenario, general principles of drug treatment and harm reduction, overview of drug treatment and rehabilitation program in Punjab, opioid substitution therapy-an overview, assessment and diagnosis, assessment and diagnosis- role play and case demonstration, buprenorphine- pharmacology, implementation of OOAT with buprenorphine- induction, stabilization and discontinuation, special clinical situations- adolescents; women; HIV; other medical conditions, dual diagnosis, scheme for implementing OOAT at government centres: overview, exposure visit to OST centre and drug de-addiction centre, psychosocial interventions, role play/demonstration of psychosocial interventions, program management-record maintenance, program management- record maintenance and reporting, program management-supply chain mechanism, program management- referral and networking and program management- minimum standards of care and monitoring and Evaluation. A team of three master trainers in NACO and psychiatrists in Department of Psychiatry, Government Medical College and technical support unit staff of PSACS gave training to the participants. The training pedagogy involved presentations, role play and group discussions to improve the knowledge and skills of participants related to OOAT.
A 22-item questionnaire was administrated at the beginning and 20 item questionnaires at the end of training program to each of the individual participants. The questions were in multiple choice questions form in the questionnaire. The questionnaire includes various questions regarding different drugs of abuse and their effects, criteria for drug dependence, substance use related disorders, model de-addiction centres in Punjab, buprenorphine pharmacology and psychosocial interventions. The standard questionnaire was developed to assess the change in knowledge of participants with training. An evaluation sheet was given at the end to give honest and critical feedback regarding the entire training program and regarding the usefulness of various sessions in understanding the problem of opioid dependence and in the management of opioid dependent persons.
Data for the current study
Data for the current study was taken from nineteen batches of OOAT training program conducted from 17 July 2017 to 27 July 2018. A total of 798 staff participated in OOAT training programs which include medical officers, staff nurses, counsellors, data entry operators and other staff including outreach workers, pharmacists, lab technicians from various government health centres in different districts of Punjab. The participant responses in pre and post-test and feedback given in evaluation sheet was analyzed.
Statistical analysis
The maximum possible score that could be obtained in the pre-test was 22 and post-test was 20. Because of difference in the maximum possible score that could be obtained in pre-test and post-test, the amount of change in knowledge before training and after training was compared using percentage of correct questions answered in the pre-tests and post-tests. The net training effect was calculated by difference in average percentage of correct questions answered between pre-test and post-test which comes out to be 32.29%.
The response of participants who are satisfied or not regarding the usefulness of sessions were calculated by simple percentage method.
Results: Distribution of different cadres of health staff was as following
|
S. no. |
Designation |
Total no. of participants |
|
1. |
Medical officer |
224 |
|
2. |
Staff nurse |
256 |
|
3. |
Counsellor |
91 |
|
4. |
Data Entry Operator |
106 |
|
5. |
Pharmacist |
83 |
|
6. |
Lab technician |
17 |
|
7. |
Other health care staff |
21 |
|
|
Total staff |
798 |
|
Batch no. |
District |
Total batch strength |
Pre-test average(%) |
Post-test average(%) |
|
1. |
Amritsar,Tarntaran,Kapurthala,SBS nagar |
40 |
32.27 |
66.99 |
|
2. |
Faridkot, Sangrur,Barnala,Fazilka |
40 |
38.39 |
67.24 |
|
3. |
Amritsar |
33 |
30.82 |
62.87 |
|
4. |
Tarntaran |
25 |
34.78 |
69.99 |
|
5. |
Kapurthala,Ferozpur,Faridkot,Ludhiana |
22 |
34.84 |
67.26 |
|
6. |
Moga,Ferozepur |
38 |
33.51 |
63.28 |
|
7. |
Tarntaran,Amritsar,Ludhiana,Fatehgarh sahib |
63 |
31.96 |
55.01 |
|
8. |
Jalandhar,Faridkot,Fazilka |
36 |
30.11 |
62.63 |
|
9. |
Patiala,Sangrur |
86 |
38.21 |
70.11 |
|
10. |
Hoshiarpur,Pathankot,Gurdaspur |
55 |
38.40 |
77.45 |
|
11. |
SAS nagar,Roopnagar,Fatehgarh sahib |
42 |
35.58 |
64.39 |
|
12. |
Ludhiana,Jalandhar,Mansa |
55 |
28.90 |
67.87 |
|
13. |
Muktsar,Mansa,Barnala,Bathinda |
57 |
30.63 |
64.91 |
|
14. |
Moga,Tarntaran,Amritsar, |
34 |
40.50 |
63.08 |
|
15. |
Barnala,Kapurthala,Bathinda,Muktsar |
45 |
39.27 |
65.54 |
|
16. |
Jalandhar,Fazilka,Faridkot,Ludhiana |
23 |
32.1 |
86.73 |
|
17. |
Roopnagar,Fatehgarh sahib,SAS nagar |
38 |
35.06 |
66.70 |
|
18. |
Barnala,Ludhiana |
45 |
36.04 |
56.77 |
|
19. |
Ferozepur, Bathinda,Faridkot |
21 |
28.07 |
64.24 |
|
|
|
798 |
34.18 |
66.47 |
ove table shows participants from various districts in 19 different batches of OOAT training program. The training program was conducted in phases starting with
So each batch consists of participants from different districts.
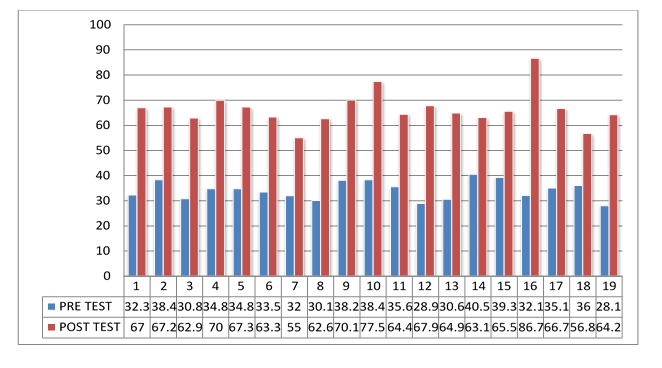
Graph 1: Comparison Between Pre Test And Post Test Percentage Of Correct Questions In Different OOAT Training Batches
The graph 1 compares the pre-test and post-test percentage of correct questions answered for the 19 different batches of OOAT training program showing that percentage was improved in post-test compared to pre-test for each of OOAT batch. The highest improvement was seen in sixteenth batch as compared to other batches.
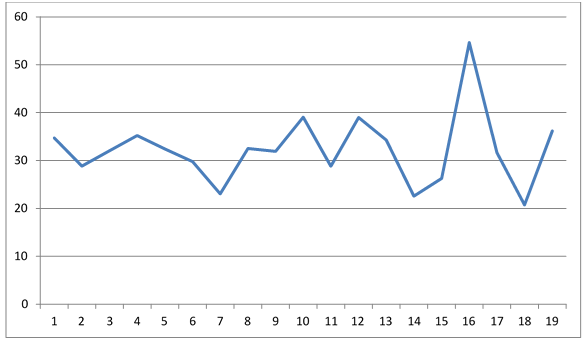
Graph 2: Improvement in Sequential Batches Of Ooat Training Program
The above graph shows the improvement in sequential batches of OOAT training program with peak in the graph showing the highest improvement in that OOAT training batch.
|
Sessions |
Useful (%) |
Can’t say(%) |
Not useful(%) |
|
Overview of drugs and drug use disorders |
98.65 |
.85 |
.50 |
|
Drug related problems and harms |
98.14 |
.85 |
1.01 |
|
Local drug abuse scenario |
93.6 |
5.40 |
1.0 |
|
General principles of drug treatment and harm reduction |
97.80 |
2.03 |
.17 |
|
Overview of drug treatment and rehabilitation program in Punjab |
97.63 |
2.2 |
.17 |
|
Opioid substitution therapy-overview |
98.14 |
1.52 |
.34 |
|
Assessment and diagnosis |
98.48 |
1.52 |
0 |
|
Assessment and diagnosis-role play and case demonstration |
94 |
4.7 |
1.3 |
|
Buprenorphine pharmacology |
96.62 |
3.21 |
.17 |
|
Implementation of OOAT with buprenorphine-induction, stabilization and discontinuation |
96.8 |
3.04 |
.16 |
|
Special clinical situations -adolescents; women; HIV; other medical conditions, dual diagnosis |
95.78 |
4.05 |
.17 |
|
Scheme for implementing OOAT at government Centre’s: overview |
93.41 |
6.25 |
.34 |
|
Exposure visit to OST Centre and drug de addiction Centre |
93.6 |
4.4 |
2 |
|
Psychosocial interventions |
96 |
4.0 |
0 |
|
Role play/demonstration of psychosocial interventions |
91.54 |
7.26 |
1.2 |
|
Program management-record maintenance |
95.95 |
3.54 |
.51 |
|
Program management-record maintenance and reporting |
95.93 |
3.9 |
.17 |
|
Program management-supply chain mechanism |
88 |
11.15 |
.85 |
|
Program management -referral and networking |
94 |
5.40 |
.6 |
|
Program management –minimum standards of care and monitoring & evaluation |
92.2 |
7.3 |
.5 |
Feedback regarding sessions in training program:
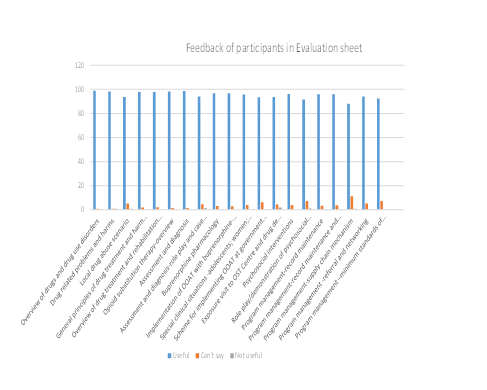
Graph 3: The graph 3 shows the feedback given by participants in evaluation sheet on different lectures and role play activities. Maximum response of participants was the lectures were useful.
Discussion
There are total 151 CHCs in Punjab. They are served by medical officers. These centres represent community based first level for the management of opioid dependent persons.
The training of the health care staff working in these health centres is crucial for effective implementation of OOAT program. OOAT is based on concept of OST which is currently available in 77 countries; of these, most countries use methadone as the OST medicine, followed by buprenorphine started being used in some government hospitals as well as in some NGO settings.[9] Opioid substitution therapy programs are effective in substantially reducing illicit opiate use, HIV risk behaviours, death from overdose and criminal activity, and financial and other stresses on drug users and their families. These programs also improve adherence to antiretroviral therapy and physical and mental health of injecting drug users. India is a good example of a developing country that is gradually integrating the provision of opioid substitution therapy into public health policies and programs.[10]
Unfortunately, the time allotted to the training on diagnosis and management of substance use disorder in undergraduate medical or other courses is very limited. Hence adequate duration of training program is required for its effectiveness. This study shows that a duration of five-days was sufficient to improve the knowledge of the participants. Overall improvement in post test scores show that it is possible to train all cadres of health care staff together. The significant improvement in knowledge of health care staff is necessary for providing services under OOAT program. The questions in pre-test and post- test were different so training demonstrates improvement in knowledge of participants.
A major point of the study was in administering pre-test, post-test and evaluation sheet, anonymity of participants was maintained. So study does not reveal about improvement in knowledge in different cadres of participants but there was improvement in overall batch. Limitation in the study was the improvement in knowledge was assessed immediately at the end of training. Future studies are required to assess the impact of training over a long period or when staff is actually working in the field. Finally, test-retest design was used which is an inferior study design as compared to other study designs.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org