Clinical Medical Case Reports and Case Series
OPEN ACCESS | Volume 1 - Issue 2 - 2026
ISSN No: 3065-7644 | Journal DOI: 10.61148/3065-7644/CMCRCS


Mesrati M¹*, Corniquet M¹, Topolanski A¹, Alsac JM¹, El Batti S¹
1Department of Vascular Surgery, Hôpital Européen Georges-Pompidou, Paris, France.
*Corresponding author: Mesrati M, Department of Vascular Surgery, Hôpital Européen Georges-Pompidou, Paris, France.
Received: March 04, 2026 | Accepted: March 18, 2026 | Published: March 30, 2026
Citation: Mesrati M, Corniquet M, Topolanski A, Alsac JM, El Batti S. (2026) “Left Renal Artery Compression: A Rare Type of Median Arcuate Ligament Syndrome.”, Clinical Medical Case Reports and Case Series, 3(1); DOI: 10.61148/3065-7644/CMCRCS/059.
Copyright: © 2026. Mesrati M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Median arcuate ligament syndrome (MALS) is caused by compression of the celiac trunk by the median arcuate ligament. Renal artery involvement is extremely rare and can lead to secondary hypertension in young patients. We report the case of a 22-year-old male medical student with newly diagnosed hypertension. Imaging revealed significant stenosis of two right renal arteries and renal asymmetry due to extrinsic compression from a prominent right diaphragmatic crus. Surgical decompression of the ligament was performed; the artery remained fibrotic, so a right aorto-renal bypass with a PTFE graft was performed. Doppler ultrasound and CT confirmed severe proximal stenosis and reduced kidney size (10 cm vs. 13 cm). Surgery restored renal perfusion. At three months follow-up, blood pressure was normalized without antihypertensive therapy, and renal function was preserved. Renal artery compression by the median arcuate ligament is rare, and early recognition and surgical management, sometimes combined with revascularization, are essential.
Extrinsic arterial compression; Median arcuate ligament syndrome; Renal artery stenosis; Secondary hypertension; Aorto-renal bypass
Median arcuate ligament syndrome (MALS) is caused by extrinsic compression of the celiac trunk by the median arcuate ligament. While compression of the celiac trunk is more common, other arteries, including the renal arteries, can be affected. Renal artery entrapment by the arcuate ligament was first described in 1962, and only a few cases have been reported. This condition represents a rare cause of secondary hypertension in young individuals, and early recognition is essential to prevent long-term renal damage.
Case Report
Mr. F.R., a 22-year-old medical student with no past medical history, was diagnosed with hypertension. An abdominopelvic CT scan was performed, complemented by a PET scan at Tenon Hospital to investigate lymphadenopathy; no hypermetabolic activity was observed, but renal asymmetry and right renal artery stenosis were noted. Further imaging at Georges Pompidou Hospital, including renal artery Doppler ultrasonography and CT, confirmed significant stenosis of the right renal artery with intrarenal hemodynamic consequences.
Measured velocities reached 4 m/s, and the right kidney was reduced in size (10 cm vs. 13 cm on the left). Two right renal arteries were present, both thin and collapsed, with subocclusion of the proximal segments, and a prominent right diaphragmatic crus in close contact. No adenopathy was observed.(figure 1).

Figure 1: CT scan demonstrating right renal artery stenosis and renal asymmetry.
The patient underwent surgery under general anesthesia via a right subcostal approach. The right renal artery was dissected retrocavally, revealing the median arcuate ligament(Figure2)

Figure 2: Intraoperative view of left renal artery compression by the median arcuate ligament.
The muscular portion was divided with electrocautery, and the fibrous portion was sectioned with scissors. The artery remained fibrotic, and a right aorto-renal bypass using a PTFE graft (Figure3) was performed. The postoperative course was uneventful. At three months follow-up, the patient had resumed his studies and daily activities, the surgical scar was clean, and blood pressure had normalized, allowing discontinuation of antihypertensive medications.
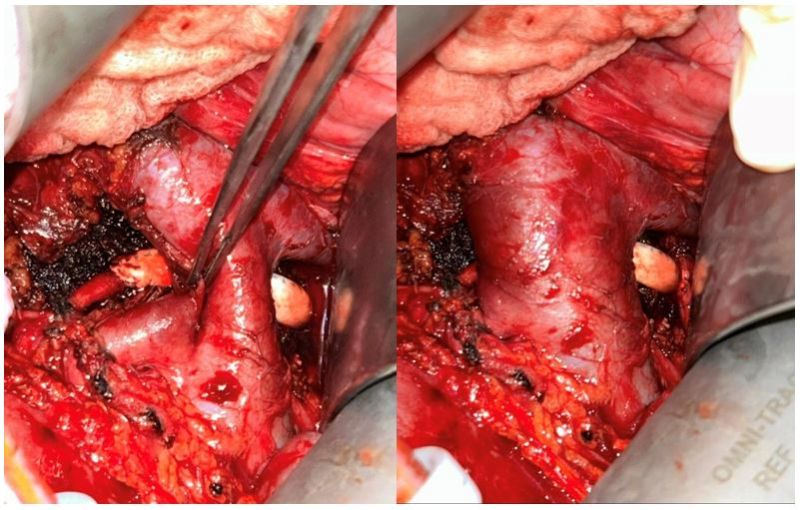
Figure 3: Right aorto-renal bypass with PTFE graft placement following ligament decompression.
Discussion
Median Arcuate Ligament Syndrome (MALS) is a rare condition in which extrinsic compression of the celiac artery, and more rarely the renal arteries, can cause ischemia and secondary hypertension [1]. While the celiac artery is most commonly affected, renal arteries may also be compressed, particularly in young patients without traditional atherosclerotic risk factors [2]. Pathophysiology involves mechanical compression, reducing blood flow and potentially causing hypertension. Diagnosis requires high clinical suspicion and multimodal imaging, including Doppler ultrasonography, CT angiography (CTA), and magnetic resonance angiography (MRA) [5,6]. CTA may show the “hooked” appearance of the artery and post-stenotic dilatation, while Doppler allows dynamic assessment of flow variations during respiration [5,6]. Management depends on severity; surgical decompression is the gold standard. When fibrosis is present, vascular reconstruction via bypass or stenting may be necessary [2,4,7]. Prognosis is favorable when intervention is timely. Multidisciplinary management involving vascular surgeons, radiologists, and nephrologists is recommended [2,4,6].
Conclusion
Renal artery stenosis accounts for approximately 1% of hypertensive patients, rising to 30% in refractory hypertension. Extrinsic compression by the arcuate ligament is extremely rare. Diagnosis relies on multiple imaging modalities, including conventional angiography, CT, MRI, Doppler ultrasound, and intravascular ultrasound. Treatment typically involves resection of the diaphragmatic crus and, when the artery is fibrotic, vascular reconstruction. Early recognition and intervention are critical to normalize blood pressure and preserve renal function.
Patient Perspective
The patient reports full return to daily activities and studies, with normalization of blood pressure and no residual symptoms.
Informed Consent
Written informed consent was obtained from the patient for publication of this case and images.
Funding and Conflicts of Interest
No external funding was received, and the authors declare no conflicts of interest.


Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org