Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Gyan Chand*, Arushi Yadav, B R Goyal, Archana Mathur, Vineet Marwaha, Manjari Jaiswal
Max Super Speciality Hospital, Patparganj, Delhi 110092, India.
*Corresponding author: Gyan Chand, Max Super Speciality Hospital, Patparganj, Delhi 110092, India.
Received: December 02, 2025 | Accepted: December 15, 2025 | Published: December 19, 2025
Citation: Chand G, Yadav A, B R Goyal, Mathur A, Marwaha V, Jaiswal M. (2025) “Chondrosarcoma of Upper Posterior Ribs Disguised as Back Pain: A Case Report and Review of Literature” Clinical Case Reports and Clinical Study, 12(5); DOI: 10.61148/2766- 8614/JCCRCS/227.
Copyright: © 2025 Gyan Chand. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Chondrosarcomas are cartilaginous neoplasms that represent the third most common primary malignant neoplasm of bone. This case report describes a 36-year-old female who presented with complaints of upper to mid-back pain and left-sided radiculopathy. CECT Chest revealed a lobulated hypodense lesion with irregular nodular calcifications arising from the left 4th rib. Left sided VATS procedure was performed, and excision of the lesion was done. Histopathological examination confirmed the diagnosis of Grade I chondrosarcoma.
Chondrosarcoma is the third most common primary malignant neoplasm of bone, following multiple myeloma and osteosarcoma, accounting for 10% of primary malignant bone tumors.[1] It affects adults between the age group of 40-70 years of age with a slight male predominance. The most common sites for these tumors are the pelvis, proximal femur, and proximal humerus, with ribs being a relatively less common site.[1] We describe a case of chondrosarcoma arising from the posterior end of a rib, contrary to the usual occurrence of the neoplasm from the anterior ribs including costochondral junctions.
Case presentation:
A 36-year-old female presented to our Neurosurgery outpatient department with complaints of upper to mid-back pain and left radiculopathy for the past 6 months. Patient had no obvious soft tissue swelling. No history of trauma, falls, or injuries to the back or spine. No complaints of fever, chills, unexplained weight loss, or night sweats. No weakness or paralysis in extremities. No cardiovascular symptoms (chest pain, shortness of breath). Chest X Ray (Fig. 1) was suggestive of a lobulated radio opaque shadow in the left paratracheal region at the level of T3-T4 vertebra.
CECT scan was performed for better evaluation which showed a well defined lobulated hypodense mass lesion, lying in the left anterior paraspinal region at the level of the posterior end of the fourth rib. The lesion was arising from the posterior end of the left 4th rib. There were irregular nodular calcifications within it, and it measures ~3.1 (CC) x 2.6 (AP) x 2.5 (TR) cm. (Fig 2).

Figure 1. Chest X ray PA view showing a homogenous, lobulated radio opacity seen in the left paratracheal region at the level of T3- T4 vertebrae.
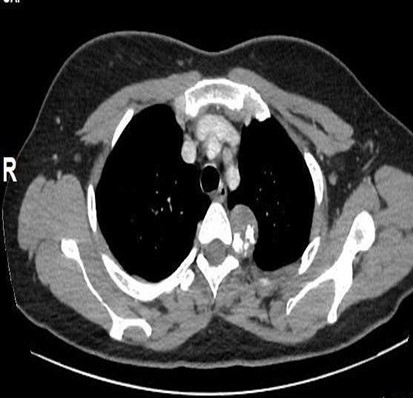
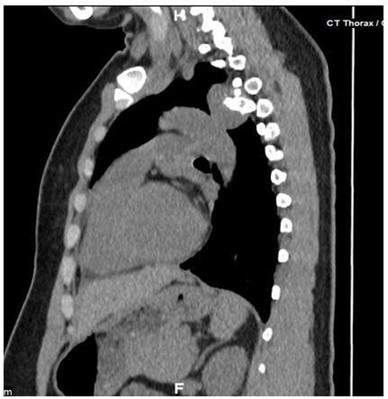
Figure 2. (A) CECT Thorax: Thin axial view showing a hypodense mass lesion arising from the posterior end of the 4th rib on the left side, irregular nodular seen calcifications within it. There is no obvious erosion of T4 vertebra. There is minimal enhancement in the mass lesion.
(B) Sagittal image showing the hypodense exophytic mass lesion in the posterior mediastinum.
Therapeutic Intervention
After thorough preoperative planning, the patient underwent Video Assisted Thoracoscopic Surgery (VATS) procedure with excision of the mass lesion.
Follow-Up And Outcomes
Histopathological examination showed chondroid tissue with a lobular pattern. There was a mild increase in cellularity with occasional binucleate nuclei and foci of mild nuclear atypia. Occasional mitosis and foci of myxoid change noted (Fig. 3).
These features were consistent with chondroid neoplasm, morphology favouring atypical cartilaginous tumour/chondrosarcoma grade I.
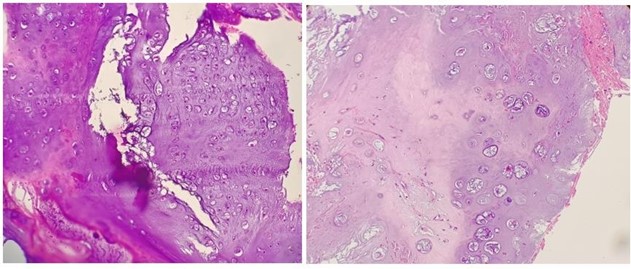
Figure 3: (A) Histopathology H&E stained slide (hematoxylin and eosin stain) at 200x magnification which demonstrates the chondroid matrix with lobular pattern. (B) H&E stained slide at 400x magnification showing increased cellularity, binucleate nuclei and nuclear atypia.
Discussion And Literature Review:
Chondrosarcoma of the rib are rare and most of the patients present with enlarging anterior chest wall tumour. We present an unusual case of chondrosarcoma arising from the posterior ribs.
CT imaging provides the most definitive diagnostic information, revealing characteristic "flocculent" or "punctate" calcifications within the chondroid matrix that create the pathognomonic "ring and arc" or "popcorn-like" appearance.[1]
Multiplanar CT reconstructions clearly delineate the tumor's relationship to adjacent structures, particularly vital mediastinal and pleural anatomy, while precisely mapping areas of matrix mineralization that may be overlooked on plain radiography. The differential diagnosis includes enchondroma, fibrous dysplasia, and metastatic disease.
Treatment involves wide surgical excision, as these tumors demonstrate relative resistance to conventional radiation and chemotherapy. Inadequate surgical margins are associated with local recurrence rates exceeding 30%. Sangma et al. presented a case report of a 29-years old female with a painless tumor on the left anterior chest wall [2]. CT showed a lobulated heterogeneous mass with peripheral calcifications in the anterior aspect of the 8th rib. Biopsy revealed Chondrosarcoma, and radical resection procedure was performed. Their study emphasized CT scanning as the preferred imaging modality and emphasized that surgical resection with wide margins remains the cornerstone of treatment with routine lifelong surveillance. This approach was mirrored in our 36-year-old patient presenting with back pain, where a prompt VATS procedure following CT diagnosis facilitated wide tumor resection.
Milants et al. analyzed a case of chondrosarcoma presenting as a lower abdominal mass and demonstrated that while MRI provides superior delineation of tumor extent and marrow involvement, CT more effectively visualizes matrix mineralization and cortical destruction.[3]
Gao et al. described an incidentally discovered mediastinal mass.[4] CT revealed a lobulated mass containing diffuse stippled calcifications adjacent to the right side of T4/5 vertebra, demonstrating classic features of cortical scalloping of the rib with marginal sclerosis. Surgical resection of portions of the fourth and fifth ribs, with subsequent histopathological examination confirming the diagnosis of periosteal chondroma.
Chondrosarcoma of the rib in our case aligns with the literature findings regarding presentation, diagnostic approach, and management strategies. The prompt identification and wide surgical excision through the VATS procedure follow current best practices for treating this challenging malignancy.
Conclusion
Chondrosarcoma of the ribs is a rare neoplasm and commonly involves the anterior ribs, however posterior rib involvement is less common. The reviewed literature highlights that chondrosarcoma management requires a multidisciplinary approach with careful radiological and histopathological correlation. Surgical resection with adequate margins remains the mainstay of treatment. Imaging plays a critical role in diagnosis, staging, and surgical planning. Future research should focus on identifying molecular markers for better prognostication and developing targeted therapies for patients with unresectable or metastatic disease.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org