Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Logan Wiedemann, Esmeralda Menjivar, Robert Villejo, Helena Heshmatipour, Nafiseh Hashemi MD*
Hashemi Eye Care, 16542 Ventura Blvd, Encino, CA 91436.
*Corresponding author: Nafiseh Hashemi MD, Hashemi Eye Care, 16542 Ventura Blvd, Encino, CA 91436.
Received: June 15, 2026 | Accepted: June 22, 2026 | Published: June 25, 2026
Citation: Wiedemann L, Menjivar E, Villejo R, Heshmatipour H, Hashemi N. (2026) “The Critical Role of Early Multidrug Antibiotic Treatment in Preventing Optic Atrophy in Cat Scratch Disease Neuroretinitis” Clinical Case Reports and Clinical Study, 13(3); DOI: 10.61148/2766-8614/JCCRCS/243.
Copyright: © 2026 Nafiseh Hashemi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
B. henselae is the most common cause of neuroretinitis. Even with its sudden and extreme changes to the optic nerve and macula that lead to frightening ocular symptoms, neuroretinitis from this bacterial source often has a promising prognosis. The 49 year old male with bilateral neuroretinitis that we focus on in this paper did not have such a favorable outcome, as his vision did not return to baseline even following double antibiotic therapy. This can be attributed to initial attempts with antibacterial monotherapy and then IV steroids pending bloodwork. This unfortunate case sets a precedent which advocates for quick initiation of antibacterial multitherapy for neuroretinitis.
ocular symptoms, neuroretinitis
Neuroretinitis is defined as the presentation of macular edema secondary to optic disc edema [1]. Although neuroretinitis has inflammatory and idiopathic causes, the most common is infectious [1], including varicella zoster, lyme disease, tuberculosis, and syphilis [2]. The most prevalent cause of neuroretinitis, though, is the bacterium B. henselae, causing an infection named Cat Scratch Disease (CSD) [3] as it is most commonly passed via scratches, bites, or licks from a feline infected with the bacterium. Due to this, determining the epidemiology of the neuroretinitis often first involves obtaining B. henselae titer regardless if there has been recent exposure to a feline [2]. If negative, a range of other titers to determine if there are other infectious causes, as well as MRI to rule out retrobulbar optic neuritis and demyelinating diseases, are completed while waiting to repeat B. henselae titer [2]. Those with neuroretinitis from B. henselae often have diminished visual acuity (VA), a relative afferent pupillary defect (rAPD), and central or cecocentral visual field (VF) defects, all of which may be unilateral or bilateral during the duration of inflammation. After recovery, the aforementioned symptoms typically return to- or near-baseline after treatment [2]. Although various studies have shown that greater than 80% of those who are treated with a variety of antibiotic therapies demonstrate visual acuity (VA) better than 20/200, there remains support for steroid usage in such cases.
An extensive previous case series highlights ocular manifestations secondary to cat scratch disease from 86 patients and 107 eyes details multiple important considerations in treatment plans of CSD. Neuroretinitis was seen to have developed in 74 (79%) of eyes considered in the series, with only 9 patients developing bilateral neuroretinitis.
Further, when compared to only systemic antibiotics used as a therapy course, a combination of antibiotics and steroids had the most statistically significant improvement of vision, with significant VA improvement (defined as VA improvement of at least 3 Snellen lines) seen in 87.5% of eyes [6]. Further, a smaller case series of 7 patients found that a double therapy of antibiotics rifampin and doxycycline seemed to quicken visual recovery and shorten the course of CSD [7]. While single-therapy antibiotic treatment plans were seen with moderate recovery in the extensive retroactive case review by Habot-Wilner et al., [6], it remains important for clinicians treating CSD to consider strong, multicourse antibiotic interventions.
This report discusses a middle aged male who manifested the typical symptoms and anatomy of CSD yet obtained bilateral optic atrophy due to delay of antibiotic multitherapy that was only given after receiving a positive B. henselae titer. While treatment plans for the disease are still ill-defined, this case underscores the importance of treating patients with presumed CSD with at least a double antibiotic therapy in a timely manner.
Case Presentation
A 49-year-old male presented to a neuro-ophthalmology clinic and reported that he began losing vision in the left eye (OS) upon waking one morning. Throughout the day, his vision progressively worsened and he was subsequently taken to the emergency room. He was informed by medical staff at the ER that he was hypertensive where he was placed on 5mg of amlodipine. The following day, he developed a similar pattern of vision loss in his right eye (OD), prompting him to see a retina specialist who noted severe edema in both the maculae and optic nerves of both eyes (OU). He was immediately started on Bactrim and referred for a neuro-ophthalmic opinion. MRI Brain and Orbit with and without intravenous contrast was also performing, revealing no mass effects, demyelinating lesions, or infarcts. Further, the MRIs revealed bilateral optic nerve head elevation without increased signal intensity; the imaging was otherwise unremarkable. Bloodwork was also performed and showed elevated inflammatory markers for ESR and CRP, at 39 and 18.9, respectively. This initial bloodwork at the hospital was completed pending the results for the B. Henselae antibody titer.
At the neuro-ophthalmologist’s office, central VA was count fingers (CF) 1ft OU and the patient’s color vision was 0/11 OU. Visual field examination showed a cecocentral defect OU. Optical coherence tomography (OCT) images of the macula showed severe macular edema and OCT retinal nerve fiber layer (RNFL) images showed extensive optic disc edema OU with an RNFL thickness of 171 microns OD and 172 microns OS. Dilated fundus exam revealed extensive disc edema and hemorrhaging with macular edema secondary to severe optic nerve inflammation OU, as well as a macular star present in both maculae. A 1+ rAPD OD was observed in the office prior to patient dilation.
Additional blood work was ordered to rule-out more specific infectious and inflammatory pathologies, including myelin oligodendrocyte glycoprotein (MOG), neuromyelitis optica (NMO), syphilis, post-infectious optic neuritis, optic neuritis secondary to meningitis, sarcoidosis, and other autoimmune disorders.
In the meantime, the patient was admitted to the hospital to undergo further diagnostic testing, including a lumbar puncture. Due to the patient’s severe and rapid vision loss, as well as his unresponsiveness to bactrim, a high dose of high dose IV methylprednisolone under the assumption of autoimmune optic neuropathy. After receiving the high dose steroid infusion for five days, the patient began a course of oral prednisone, beginning with 60 mg daily and tapering the medication by 10 mg every week until completing the therapy. The lumbar puncture he underwent came back inconclusive, but the laboratory evaluating blood work sent from the neuro-ophthalmology clinic reported a high titer of B. henselae.
In conjunction with a self-reported illness roughly two weeks prior to the onset of vision loss and being scratched by a kitten at home, this positive blood work result for B. heneslae confirmed that the neuroretinitis was secondary to CSD. Double therapy of Rifampin and doxycycline was initiated for six weeks immediately. However, his vision did not improve significantly and the patient subsequently developed bilateral optic atrophy.


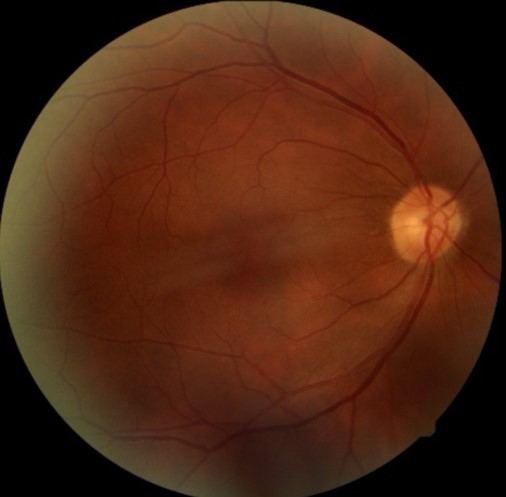
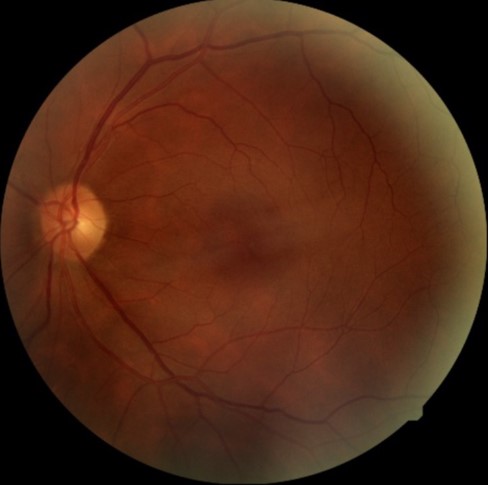
Figure 1: Moving left to right from top to bottom, panels 1 and 2 display aforementioned macular star observed on dilated slit-lamp exam on initial encounter at the neuro-ophthalmology clinic OD and OS, respectively; panels 3 and 4 display the absence of a macular star 14 months after initial visit OD and OS, respectively.
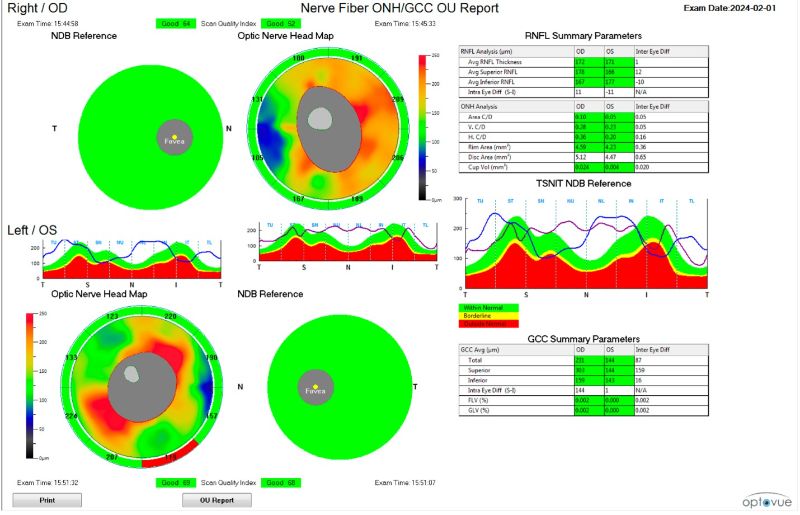
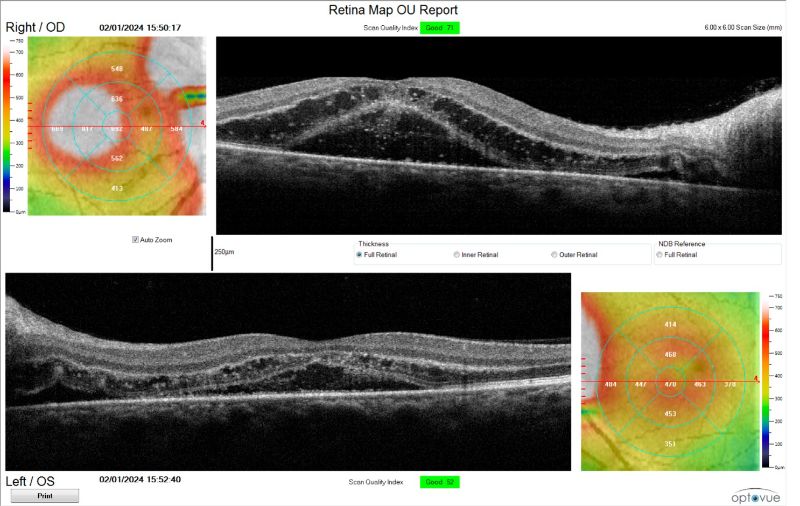
Figure 2: The above images show initial presentation to the clinic with OCT RNFL and OCT Macula images, indicating bilateral optic disc & macular edema OU, respectively.
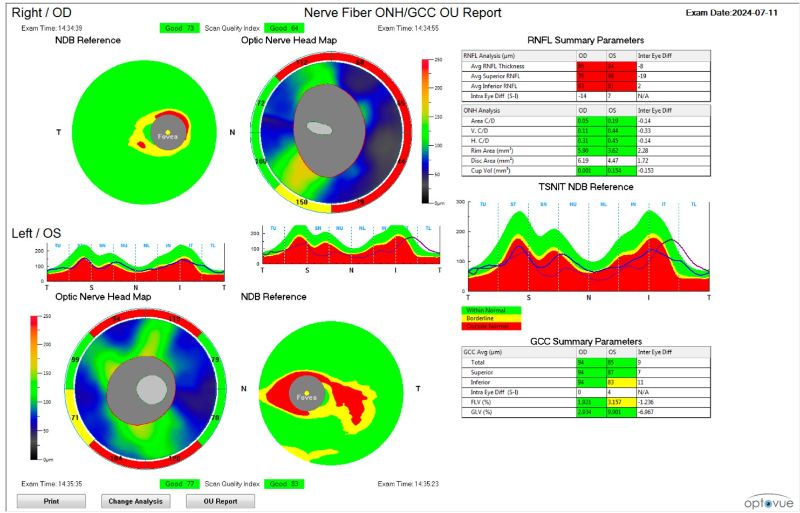
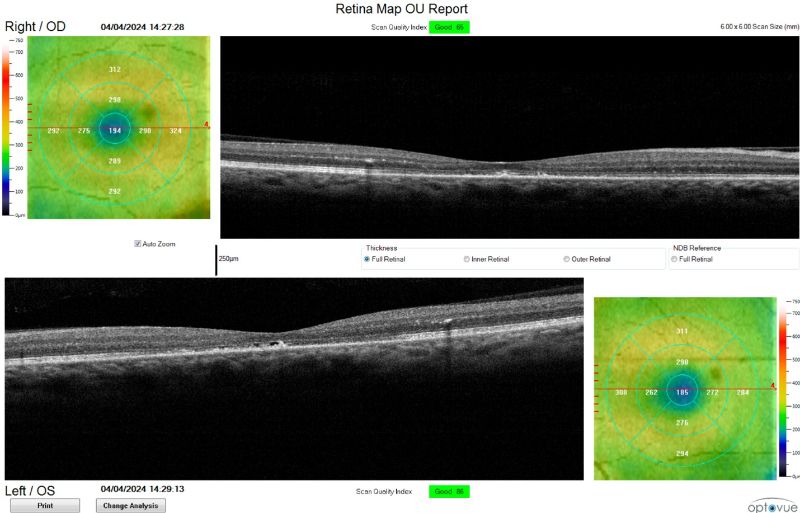
Figure 3: Above images show quieted optic disc and macular edema OU, respectively, three months after initial visit to neuro-ophthalmology clinic.
Discussion
This case illustrates how a short diagnostic delay in fulminant, bilateral Bartonella henselae neuro-retinitis can convert what is usually a self-limited, good-prognosis disease into one that leaves permanent visual sequelae. Several features conspired against a prompt, targeted therapy.
1. Atypical initial presentation.
• Simultaneous, profound visual loss in both eyes is distinctly uncommon in cat-scratch disease (CSD); most series report bilateral neuro-retinitis in <10 % of cases [6].
• The resulting diagnostic uncertainty—coupled with the absence of an obvious cat exposure in the history initially—lowered clinical suspicion and postponed empiric Bartonella-directed therapy.
2. Monotherapy and waiting for serology.
Trimethoprim-sulfamethoxazole was begun empirically, but B. henselae is intrinsically less susceptible to this agent. Evidence from small series and in-vitro studies favors doxycycline, azithromycin, rifampin or a combination thereof for rapid bactericidal activity [4,6,7]. Relying on a single agent with marginal Bartonella coverage likely allowed the infection to progress while serology was pending (turn-around 7-10 days in our laboratory).
3. Isolated high-dose corticosteroid use.
Because the patient’s vision continued to worsen and extensive imaging/CSF studies were unrevealing, 1 g/day IV methyl-prednisolone was administered for five days. Although several retrospective series suggest that steroids added to antibiotics can blunt inflammation and speed visual recovery [6], glucocorticoids given before antimicrobial control of the organism may increase bacterial replication and optic-nerve axonal loss. In hindsight, the temporal association between steroid initiation and precipitous decline in acuity supports this concern.
4. Delayed initiation of combination therapy.
Once B. henselae IgG serology returned positive, rifampin + doxycycline was started and disc oedema resolved within four weeks; nevertheless, the macular star and outer-retinal disruption persisted for three months and permanent optic-atrophy developed. This reinforces experimental data indicating that optic-nerve head axons suffered irreversible damage within days of unchecked inflammation.
Conclusion
Bartonella neuroretinitis usually carries an excellent visual prognosis, yet our patient’s outcome—optic atrophy and permanent acuity loss—highlights the narrow therapeutic window during which axonal integrity can be preserved. In fulminant, bilateral cases we should initiate empiric combination antibiotics immediately and add corticosteroids only after—or concurrent with—effective antimicrobial coverage; and pursue serological confirmation without delaying therapy. Early, aggressive treatment is the best safeguard against irreversible optic-nerve damage and should be considered the standard of care until prospective data become available.
Credit authorship contribution statement
Logan Wiedemann: Writing – review & editing, Writing – original draft . Esmeralda Menjivar: Writing – review & editing, Writing – original draft. Robert Villejo and Helena Heshmatipour: Writing – review & editing. Nafiseh Hashemi, MD: Conceptualization, Analysis & Interpretation, Investigation, Writing – review & editing.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org