Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Ahmed Hijazi¹*, Mandira Chakraborty1, Honey Philip1
Bankstown-Lidcombe Hospital, Southwestern Sydney Local Health District, NSW, Australia.
*Corresponding author: Ahmed Hijazi, Bankstown-Lidcombe Hospital South Western Sydney Local Health District NSW, Australia.
Received: April 28, 2026 | Accepted: May 06, 2026 | Published: June 17, 2026
Citation: Hijazi A, Chakraborty M, Philip H. (2026) “Resuscitation Planning Prior to In-Hospital Cardiac Arrest: A Three-Year Retrospective Observational Study in a Metropolitan Australian Hospital” Clinical Case Reports and Clinical Study, 13(2); DOI: 10.61148/2766-8614/JCCRCS/238.
Copyright: © 2026 Ahmed Hijazi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
In-hospital cardiac arrest (IHCA) is associated with high mortality and significant healthcare resource utilisation. Early goals-of-care discussions and formalised resuscitation planning are recommended to ensure that cardiopulmonary resuscitation (CPR) aligns with patient preferences and clinical appropriateness. However, real-world adherence to resuscitation planning prior to IHCA remains unclear.
Aim: To evaluate the prevalence of documented resuscitation plans prior to IHCA and identify missed opportunities for advance care planning in ward-based patients.
Methods
A retrospective observational study was conducted at a 433-bed metropolitan hospital in Sydney, Australia. Adult patients who experienced ward-based IHCA between January 2022 and December 2024 were included. Arrests occurring in ICU, emergency department, operating theatres, or procedural areas were excluded. Electronic medical records were reviewed to extract demographic data, admitting specialty, timing of arrest, resuscitation plan status, prior documentation of goals-of-care discussions, prior Medical Emergency Team (MET) calls, ICU step-down status, and outcomes. Descriptive statistics were performed.
Results
Sixty-four patients met inclusion criteria. Median age was 78 years (range 45–97), and 64% were male. Only 3 patients (4.7%) had a completed resuscitation plan at the time of IHCA. Thirteen patients (20%) had documented evidence on the EMR of discussions regarding resuscitation status during admission; however, only 2 of 8 patients identified as not for CPR during these discussions had formalised orders. Ten patients (15.6%) had a prior MET call, and 8 patients had been stepped down from ICU; formalised resuscitation planning occurred in only one ICU step-down case. Survival to discharge was 17.2%, with an overall in-hospital mortality of 82.8%.
Conclusion
Formal resuscitation planning prior to IHCA was uncommon despite identifiable high-risk features and documented discussions in a subset of patients. Failure to convert goals-of-care discussions into formal documentation represents a significant systems gap. Structured triggers for resuscitation planning, particularly following clinical deterioration and ICU transition, may improve patient-centred care and reduce potentially non-beneficial resuscitation.
In-hospital cardiac arrest; Advance care planning; Resuscitation planning; End-of-life care; Medical emergency team; Goals of care
In-hospital cardiac arrest (IHCA) remains a major cause of morbidity and mortality in acute care hospitals. Recent international literature suggests that survival to discharge after IHCA has increased in the last two decades, however remains between 15% to 25%, depending also upon patient population and arrest characteristics and rhythm.¹-³ Australian data demonstrates similar outcomes, with mortality exceeding 74%, again dependent upon patient and hospital demographics and arrest characteristics.⁴ Despite technological and systems improvements in rapid response and resuscitation science, outcomes remain particularly poor among elderly patients and those with significant comorbidity.³,⁵
Advance care planning (ACP) and formal resuscitation planning are critical components of high-quality, patient-centered care. The Australian Commission on Safety and Quality in Health Care emphasises that goals-of-care discussions should occur early and be clearly documented to guide clinical decision-making during deterioration.6,7 Similarly, NSW Health Policy Directive PD2014_030 outlines that resuscitation plans should be discussed and formalised for patients at risk of clinical deterioration or where CPR may be inappropriate.8 Patients with progressive advanced life limiting illnesses or poor 6-12 month survivability prognosis should have resuscitation planning discussion and formalisation during their hospital admission. 8
Despite these policy frameworks, resuscitation decision-making in acute hospitals frequently remains reactive rather than anticipatory. Goals-of-care discussions are often deferred until significant clinical deterioration occurs, including during rapid response activation or at the time of cardiac arrest itself.9–11 Decision-making under such crisis conditions may limit meaningful patient participation, increase emotional burden on families, and reduce the likelihood that care aligns with previously expressed values.12 Furthermore, in the absence of clearly documented resuscitation plans, patients who may have been clinically inappropriate candidates for CPR can undergo invasive and potentially non-beneficial interventions, including chest compressions, endotracheal intubation, and escalation to intensive care. Beyond the risk of patient harm, inappropriate or unwanted resuscitation attempts may contribute to moral distress among healthcare professionals, conflict with families, and utilisation of substantial healthcare resources in circumstances where the probability of meaningful recovery is extremely low.13, 14
Evaluating the prevalence of formalised resuscitation planning prior to IHCA provides an important measure of whether advance care planning processes are functioning as intended. If patients experiencing cardiac arrest lack documented resuscitation plans despite identifiable high-risk features during admission, this may reflect missed opportunities for earlier goals-of-care discussions and formalisation. Accordingly, this study aimed to evaluate the prevalence of documented resuscitation plans prior to ward-based IHCA in a metropolitan Australian hospital and to identify potential systems gaps in advance care planning.
Methods
Study Design and Setting
A retrospective observational study was conducted at a 433-bed metropolitan referral hospital in Sydney, Australia, serving a culturally and linguistically diverse population.
Inclusion Criteria
Exclusion Criteria
Data Collection
Electronic medical records were reviewed. Extracted variables included:
Statistical Analysis
A standardized date collection tool was developed in Microsoft Excel to ensure consistent extraction of data using the above extracted variables. A separate independent investigator extracted data for all in-hospital deaths from 2022 to 2024. The medical record number (MRN) of each patient who was included in the retrospective study was searched in both data sets to ensure accuracy of collected data.
The data underwent descriptive analysis, with descriptive statistics calculated including frequencies, percentages, means, medians, and ranges.
Subgroup analyses were performed to compare rates of resuscitation plan formalisation amongst patients who had previously required a medical emergency team (MET) call during their admission, or those who had been stepped down from ICU compared to those who had not.
Additionally, comparisons were made between the rates of documentation of discussions between medical teams and patients regarding resuscitation planning and the formalisation of plans.
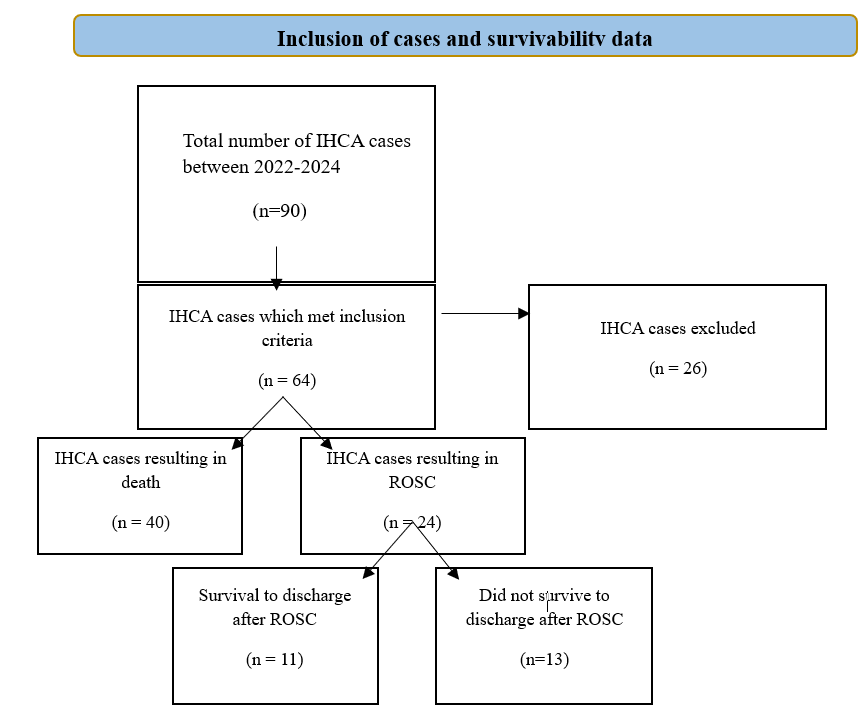
Figure 1: Inclusion of cases and survivability data
Results
Patient Characteristics
A total of 64 patients were included in the analysis. The cohort was predominantly male, comprising 64% (n = 41) of patients, with females accounting for 36% (n = 23).
The mean age was 76.2 years, with a median age of 78.0 years (range 45–97 years), reflecting an elderly population with a broad age distribution.
Most patients were admitted under medical specialties. Geriatrics was the most common admitting team, accounting for 30% (n = 19) of cases, followed by Cardiology at 22% (n = 14) and Respiratory Medicine at 19% (n = 12). Renal Medicine accounted for 9% (n = 6) of admissions, and General Surgery for 5% (n = 3). Other admitting specialties collectively represented 16% of cases and included Medical Oncology (5%, n = 3), Colorectal Surgery (3%, n = 2), and single cases (2% each) under Neurology, Gastroenterology, Rehabilitation Medicine, Upper Gastrointestinal Surgery, and Ear, Nose and Throat Surgery.
More than half of all in-hospital cardiac arrests occurred on three medical wards: 2G (19%, n = 12), 3F (17%, n = 11), and 3H (16%, n = 10), together accounting for 52% of events. Additional arrests occurred on 2J (11%, n = 7) and 3B (9%, n = 6). The remaining cases were distributed across several other wards, including 3J (8%, n = 5), 3A (5%, n = 3), 2D (5%, n = 3), 2A (2%, n = 1), and 2B (2%, n = 1).
|
Characteristics |
Sub characteristics |
Proportion |
|
Gender |
Male Female |
64% (n=41) 36% (n=23)
|
|
Age
|
Mean Median Range |
76.2 years 78.0 years 45-97 years
|
|
Ward |
2G 3F 3H 2J 3B Other |
12 11 10 7 6 3J (5), 3A (3), 2D (3), 2A (1), 2B (1) |
|
Admitting team |
Geriatrics Cardiology Respiratory Renal General Surgery Other |
19 14 12 6 3 Medical Oncology (3), Colorectal Surgery (2), Neurology (1), Gastroenterology (1), Rehab (1), Upper GI (1), ENT (1) |
Resuscitation Planning Prior to Arrest
Only 3 patients (4.7%) had a completed resuscitation plan at the time of IHCA. One was documented as “for CPR” and two as “not for CPR”.
Thirteen patients (20%) had documentation of goals-of-care discussions during admission. Five Patients were identified as ‘for CPR’. Of the eight patients identified in discussion as not appropriate for CPR, only two had formalised “not for CPR” orders.
Clinical Deterioration Triggers
Ten patients (15.6%) had a prior MET call during admission. Only two had resuscitation planning discussions following MET review. In one case, ICU recommended limitation of resuscitation; however, this was not formalised.
Eight of the sixty-four included patients had been stepped down from ICU prior to arrest. Only one had a completed resuscitation plan at the time of ward transfer.
Outcomes
Return of spontaneous circulation occurred in 37.5% of patients. Survival to discharge was 17.2%. Overall in-hospital mortality was 82.8%
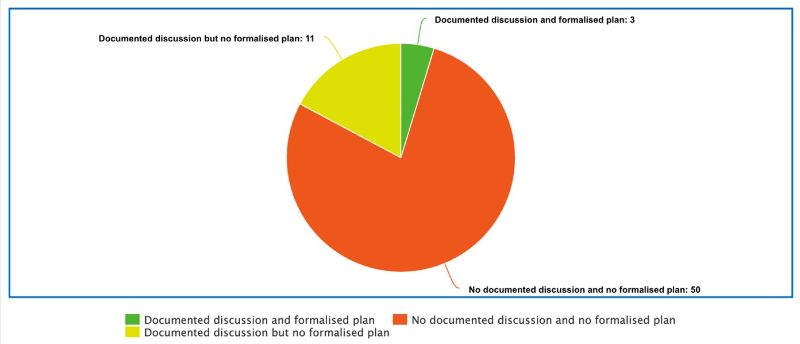
Figure 1: Documentation of goals of care discussions and formalisation of resuscitation plans
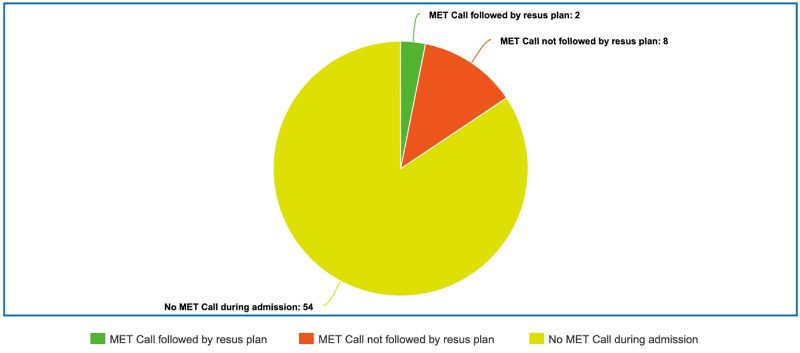
Figure 2: Resuscitation planning following MET Calls
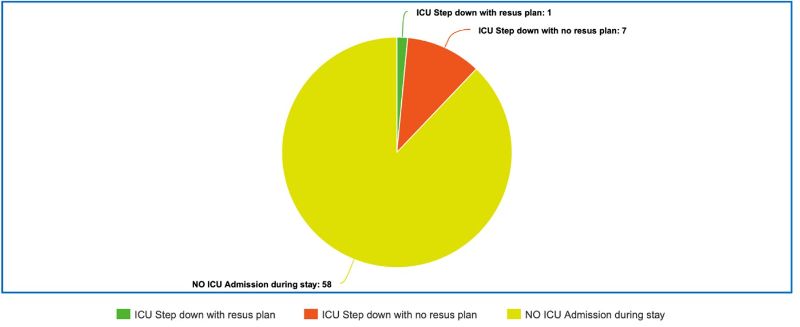
Figure 3: Resuscitation planning for ICU-Stepdown patients
Discussion
This study demonstrates that formalized resuscitation planning prior to IHCA was uncommon, occurring in fewer than 5% of cases. Although one in five patients had documented evidence of goals-of-care discussions between the patient or family and the treating team, formalisation of these discussions into ‘resuscitation plans’ frequently did not follow.
The discrepancy between discussions of goals of care and formalization of resuscitation plans represents a critical systems failure. Documentation is crucial in ensuring clarity across multidisciplinary teams, and in this context is important in preventing unwanted or non-beneficial interventions.5 Failure to formalize clinical decisions may result from a variety of factors, including time constraints, workflow barriers, or often, a lack of certainty amongst junior members of medical teams in completing ‘resuscitation plan’ documents.
The low rate of completion of ‘goals of resuscitation plan’ following MET call activation suggests missed opportunities for resuscitation planning following clinical deterioration. Rapid response activations are important junctures for reassessment of goals of care.9,11 When deterioration sufficient to trigger a MET call occurs, this should prompt consideration of whether escalation aligns with prognosis and patient values.8
Similarly, the transfer of patients from ICU to the wards represents a high-risk transition point. Patients leaving ICU often remain physiologically vulnerable.16 Clear documentation of goals-of-care at transition may prevent crisis-driven decisions should deterioration recur. Systems failures may be at fault here, with differing software being used in the ICU compared to the wards in the hospital included in this study, which does not allow for the transfer of resuscitation plans created on the ICU software, to the ward-based software.
Survival to discharge in this cohort (17.2%) aligns with international IHCA data.1-3 Notably, mortality was highest among elderly patients admitted under medical specialties, consistent with prior literature demonstrating poor outcomes among frail and chronically ill populations.17
Overall, our finding suggest that resuscitation planning unfortunately in some instances remains reactive rather than proactive. Early identification of high risk patients, for example those being stepped down from ICU or those requiring rapid response calls, and early formalization of resuscitation plans may help limit futile resuscitative efforts.
Structured interventions could include:
These system-level strategies align with national safety standards emphasising comprehensive care and recognition of clinical deterioration.6
Strengths
This study has several strengths. Firstly, it includes a three-year cohort, which provides a comprehensive insight into resuscitation planning performance in this center. Detailed extraction of data allowed for comprehensive subgroup analysis. Additionally, benchmarking against local policy for resuscitation planning and international literature for outcomes following IHCA enabled identification of gaps and alignment with best possible standards.
Limitations
This study has several limitations worth noting. Firstly, it has a single-center design, which does not allow generalizability. The retrospective methodology, although useful for data analysis, relies heavily on interpretation of documentation in medical records. Some MET calls, goals of care discussions and resuscitation planning may not have been reported, and this was deemed random and did not result in selection bias. Finally, we did not capture qualitative data regarding clinician or family perspectives. Future prospective studies incorporating these elements would provide deeper insights.
Future Study
Future research should extend beyond descriptive audit data to evaluate interventions aimed at improving timely resuscitation plan completion. A prospective quality improvement study assessing the impact of targeted strategies, such as electronic medical record alerts, junior doctor education, and consultant-led goals-of-care discussions would be valuable. Additionally, qualitative studies exploring clinician and system-level barriers to early resuscitation planning may help identify modifiable factors contributing to low compliance. Multicentre studies across other NSW hospitals would improve generalisability and allow benchmarking of adherence to NSW Health PD2014_030 guidelines. Finally, examining patient-centred outcomes such as rates of non-beneficial resuscitation attempts, ICU utilisation, length of stay, and family satisfaction would help qualitatively clarify whether better resuscitation planning translates into meaningful clinical impact.
Conclusion
In this three-year retrospective study of ward-based in-hospital cardiac arrest at a metropolitan Australian hospital, formal resuscitation planning prior to arrest was uncommon, occurring in fewer than 5% of cases. Although documented goals-of-care discussions occurred in a subset of patients, these conversations frequently did not translate into formalised resuscitation orders. This gap between discussion and documentation represents a significant systems-level vulnerability, particularly in elderly patients with high mortality risk and identifiable triggers for deterioration such as prior MET activation or ICU step-down.
The findings suggest that resuscitation decision-making in this setting remains largely reactive rather than anticipatory. Missed opportunities for formalisation following clinical deterioration or at transition points of care may contribute to crisis-driven decision-making and potentially non-beneficial resuscitation attempts. Structured system-level interventions including electronic prompts, clearer transition processes between ICU and ward platforms, and targeted education for junior medical staff may improve adherence to established policy frameworks and better align care with patient prognosis and preferences.
Improving the consistency and timeliness of resuscitation planning is not merely a documentation exercise; it is fundamental to delivering patient-centred, ethically aligned, and resource-conscious healthcare. Strengthening systems that support early and proactive goals-of-care discussions may reduce avoidable harm and ensure that resuscitative efforts are consistent with both clinical appropriateness and patient values.
Acknowledgements
The authors thank the MET team members and ICU staff at Bankstown-Lidcombe Hospital for their ongoing dedication to quality improvement practices and patient care. We acknowledge the support of Southwestern Sydney Local Health District in facilitating this research.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of Interest
The authors declare no conflict of interest
Data availability
The datasets generated and analysed during this current study are not currently available to the public due to patient privacy requirements but are available from the corresponding author on reasonable request and with appropriate ethics approval.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org