Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Suman Ahuja, Jawad Hassan*
Department of Haematology, Liaquat National Hospital, Karachi.
*Corresponding author: Jawad Hassan, Department of Haematology, Liaquat National Hospital, Karachi, Pakistan.
Received: April 28, 2026 | Accepted: May 06, 2026 | Published: May 12, 2026
Citation: Ahuja S, Hassan J. (2026) “Pediatric B- Lymphoblastic Leukemia Presenting with Granulomatous inflammation: Diagnostic and Pathological Considerations” Clinical Case Reports and Clinical Study, 13(2); DOI: 10.61148/2766-8614/JCCRCS/237.
Copyright: © 2026 Jawad Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Bone marrow granulomas and fibrosis in trephine biopsies are a rare findings in pediatric acute lymphoblastic leukemia (ALL). Possible causes include infectious (especially tuberculous, but also many other bacterial, viral, fungal and parasitic agents) and non-infectious causes (especially medications, autoimmune disease, sarcoidosis, hematological and non-hematological malignancy). Their coexistence at initial presentation can create significant diagnostic difficulty by masking leukemic infiltration and is unusual and sparsely reported. We had a case of 11 years old female child presented with pallor and cervical lymphadenopathy and history of transfusions, diagnosed as B-lymphoblastic leukemia on bone marrow biopsy with incidental finding of non-caseating granulomas.
B- lymphoblastic leukemia, Granuloma, Bone marrow biopsy, Fibrosis
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy, with B-cell lineage accounting for the majority of cases. B-acute lymphoblastic leukemia (B-ALL) is a malignant neoplasm of lymphoid progenitor cells characterized by uncontrolled proliferation of immature B-cell precursors in the bone marrow, peripheral blood, and extramedullary sites. The disease typically presents with bone marrow failure, circulating blasts, and systemic symptoms such as fever, pallor, and bleeding tendencies. Bone marrow examination remains central to diagnosis, risk stratification, and treatment monitoring in pediatric ALL.
Granulomatous inflammation represents a distinctive pattern of chronic inflammation characterized by a cell-mediated immune response against an offending agent. 1 Although granulomas are infrequently encountered in bone marrow biopsies, their identification is clinically significant and is rarely been reported in association with hematological malignancies1.
The coexistence of granulomatous inflammation with B-ALL is uncommon and may pose a diagnostic challenge. Herein, we report a case of a 11-years old female child, who presented with pallor and neck swelling was diagnosed as a case of B-ALL with granuloma and fibrosis on trephine biopsy.
Case presentation:
An 11 years old female patient; referred to our setup due to low hemoglobin (Hb) since 4 months. On examination there is pallor and left sided cervical lymphadenopathy. Laboratory investigations done (Table 1). She was transfused with one packed RBC and two units of platelets. Bone marrow biopsy done due to persistence of cytopenias that revealed paucispicular and hypocellular aspirate with neutrophils, lymphocytes and blast cells seen. Differential count performed on touch imprints (Figure 1) exhibiting Blasts 49%, Lymphocytes 23%, Erythroid Precursors 20%, and Plasma cells 08%. Morphology assessment showed blast cells characterized by small to medium size, high nuclear to cytoplasm ratio, fine chromatin, indistinct nucleoli and scant amount of cytoplasm. No megakaryocytes seen. Bone marrow trephine biopsy showed cellularity around 95-99% and diffuse infiltration by blast cells with background fibrosis and multiple focal collections of epitheloid macrophages forming non-caseating granulomas(Figure 2). Residual hematopoiesis is markedly suppressed. Cytochemical Myeloperoxidase stain was negative in blast cells. Bone marrow Immunohistochemistry showed diffuse positivity of TdT, CD34, CD79a, CD19 and CD10. CD68 (PGM1) was positive in epitheloid macrophage aggregates(Figure 3). Reticulin Stain highlighted Grade 2 fibrosis. Infective workup such as Ziehl Neelson Stain and Modified Ziehl Neelson Stain were negative for typical and atypical Mycobacterium and Grocott Methamine Silver was negative for fungal hyphae.Thus the diagnosis of B- cell Lymphoblastic Leukemia was made on the basis of bone marrow morphology and immunohistochemistry. Multiple non-caseating Granulomas seen in trephine core. Possible causes of granuloma are due to infections / sarcoid reaction due to underlying disorder, (Acute Lymphoblastic Leukemia) / drug reactions / inflammatory conditions, foreign body reactions etc.
Table 1:
|
Hb |
6.7 gm/dl |
|
MCV |
82.1fl |
|
WBC |
3.04x109/L |
|
Neutrophils |
26% |
|
Lymphocytes |
70% |
|
Monocytes |
04% |
|
Platelets |
36x109/L |
|
Recticulocyte Count |
2.46%. |
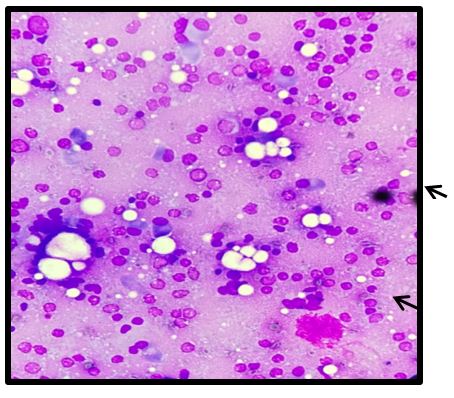
Figure 1: Moderately cellular aspirate showing predominant population ofblast cells (pointed by arrows).
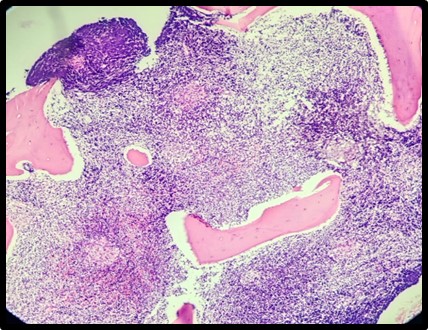
Figure 2 (a): Multiple non-caseating granulomas (pointed by arrows) in the background of blast cells infiltration
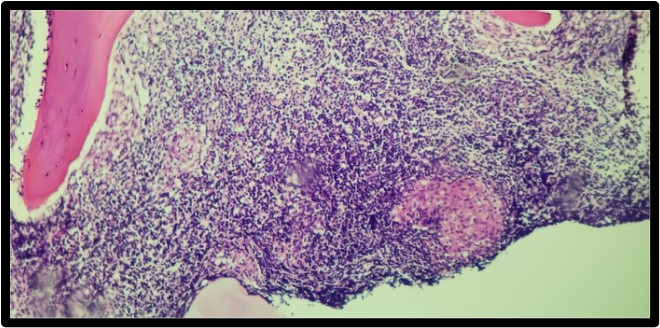
Figure 2 (b): A focal collection of epitheloid macrophages forming non-caseating granuloma.
Discussion:
The coexistence of B-cell acute lymphoblastic leukemia (B-ALL) and non-caseating granulomas in the bone marrow is exceptionally rare and poses significant diagnostic and therapeutic challenges. Acute lymphoblastic leukemia is primarily defined by clonal proliferation of immature lymphoblasts in bone marrow, yet granulomatous inflammation is not a typical histopathologic feature of this disease(2). Granulomas in bone marrow biopsies are described infrequently, with reported incidence ranging from 0.3% to 2.2% of all marrow specimens. While granulomas have been reported in association with Hodgkin lymphoma, non-Hodgkin lymphoma, and multiple myeloma, their occurrence with acute lymphoblastic leukemia is rarely documented. In the American Journal of Clinical Pathology case series, among ten patients with non-Hodgkin’s lymphoproliferative malignancies and marrow granulomas, only one case involved acute lymphoblastic leukemia, underscoring the exceptional nature of this finding(3). Mechanisms behind non-caseating granuloma formation associated with malignancies have been described as sarcoid-like reactions (SLRs). Such reactions are histologically indistinguishable from granulomas seen in systemic sarcoidosis but occur in the setting of neoplastic disease without fulfilling clinical criteria for sarcoidosis. The pathogenesis is believed to involve immune activation by tumor antigens or paraneoplastic immune responses, triggering T-lymphocyte and macrophage aggregation into granulomatous formations(4).The identification of granulomas within a leukemic marrow necessitates a thorough exclusion of infectious etiologies (especially mycobacterial and fungal infections) and true systemic sarcoidosis before attributing the findings to a sarcoid-like reaction. In regions with high tuberculosis prevalence, this distinction is particularly critical. Prior case reports emphasize the need for comprehensive microbiologic investigations, including Ziehl–Neelsen staining, PCR testing, and appropriate cultures, to avoid misdiagnosis and inappropriate therapy(2). In our case,there was no clinical evidence of multisystem involvement, special stains for typical and atypical Mycobacterium and fungal infection (Ziehl Neelson , Modified Ziehl Neelson Stain and Grocott Methamine Silver) were negative , PCR for Mycobacterium infection tuberculosis (MTB by genexpert) was also negative. Based on these, infectious etiology and sarcoidosis were ruled out.
Furthermore, granulomatous reactions can sometimes overshadow or delay the recognition of leukemic infiltrates, especially if blast percentages are low or focal. Close correlation witimmunophenotyping, and cytogenetic analyses is therefore essential to confirm the diagnosis of B-ALL in the presence of granulomatous marrow changes.(2). In summary, non-caseating granulomas within the bone marrow in association with B-ALL, while exceedingly rare, represent a documented phenomenon that can complicate diagnosis and management. Clinicians should maintain a high index of suspicion for underlying hematologic malignancy in patients presenting with unexplained marrow granulomas, particularly after infectious and systemic granulomatous diseases have been excluded. A coordinated diagnostic strategy including morphology, immunophenotyping, microbiologic testing, and clinical correlation is essential to guide appropriate treatment.
Competing Interest: The authors declared no conflict of interest.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org