Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Hanane El ghouat
Professor Qualified, Regional Center for Education and Training Professions, Rabat/ Morocco.
*Corresponding author: Hanane El ghouat, Professor Qualified, Regional Center for Education and Training Professions, Rabat/ Morocco.
Received: March 05, 2026 | Accepted: March 11, 2026 | Published: March 18, 2026
Citation: Hanane El ghouat. (2026) “Mentalizing Therapy for Anxious Children: A Systematic Review” Clinical Case Reports and Clinical Study, 13(2); DOI: 10.61148/2766-8614/JCCRCS/235.
Copyright: © 2026 Hanane El ghouat. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Childhood and adolescent anxiety disorders are one of the most prevalent forms of internalizing psychopathology globally, and are associated with a multitude of challenges including difficulties with affect regulation, social challenges, as well as cognitive and academic challenges that can exacerbate developmental delays. Although Cognitive Behavioral Therapy (CBT) remains the leading evidence based treatment for pediatric anxiety disorders, there is a growing need for alternative or complementary interventions as not all youth benefit from initial treatments. Recent literature has begun to explore adaptations of Mentalization-Based Therapy (MBT) for use with children and adolescents; however, there has been no empirical research examining the effectiveness of MBT when treating pediatric anxiety disorders.
Methods: This systematic review was conducted in accordance with the PRISMA 2020 statement. We searched PubMed, Scopus, Web of Science and PsycINFO for studies published between 1997 and 2025. The criteria were: (1) adolescents aged 5–17 years who received MBT; (2) diagnoses of anxiety disorders; and/or (3) clinically significant internalizing symptoms. Fifteen studies met our criteria, including six randomized controlled trials (RCTs) and nine quasi-experimental studies/pilot studies. We assessed the risk of bias using the Cochrane RoB 2 tool. Due to the large degree of heterogeneity, we were only able to perform a partial quantitative synthesis.
Results: Internalising and anxiety symptoms were reduced following MBT in all study designs. MBT was also associated with improvements in emotional regulation and reflective functioning in both children and parents. Most RCTs showed moderate to large effects of MBT compared with control conditions, although there was a considerable degree of heterogeneity between studies.
Conclusion: MBT shows emerging promise as a developmentally informed intervention for pediatric anxiety, warranting further large-scale, anxiety-specific randomized trials.
Mentalization-Based Therapy (MBT); MBT-C; MBT-A; Pediatric Anxiety; Internalizing Disorders; Reflective Functioning; Emotional Regulation; Attachment Theory; PRISMA; Systematic Review
1. Introduction
1.1 Childhood Anxiety and Its Developmental Impact
Anxiety disorders are amongst the most common mental health disorders in children and adolescents. A systematic review and meta-analysis of epidemiological studies revealed that the pooled prevalence for any anxiety disorder was 6-7% at any given time (Polanczyk et al., 2015). Anxiety disorders can create a large amount of suffering and can cause significant interference with the functioning of a child. They can cause social as well as academic difficulties and can negatively affect the functioning of the family.
Several developmental issues have been identified that are associated with the diagnosis of child and adolescent anxiety disorders. These include difficulties with emotional management, poor social skill acquisition, and poor adaptation to a range of situations. A 2021 systematic review of psychological interventions for the treatment of paediatric anxiety disorders was published in Clinical Child and Family Psychology Review. The review concluded that paediatric anxiety disorders constitute a clinically significant, chronic condition. However, child anxiety is a highly treatable condition (Baker et al., 2021). Untreated childhood anxiety has been shown to increase the risk of the development of a range of other subsequent mental health conditions, including depressive disorders, substance- related disorders and personality (mood) pathology, as well as persistent internalising symptoms that can severely impact the lives of adolescents and young adults for years (James et al., 2020).
Child anxiety symptoms are not unusual. Most of the research in the field of child anxiety has assumed that symptoms of anxiety are part of a larger pattern of internalizing behavior consisting of mood symptoms (i.e., dysphoria), avoidance, and difficulty in regulating biological processes (e.g., sleep patterns, appetite). Given the continuity of these larger patterns from childhood into early adolescence, intervention at this stage should target the underlying processes that sustain them rather than attempt to modify the manifestations of these processes, the anxiety symptoms.
1.2 Mentalization Theory and Its Clinical Foundations
The mentalization theory is grounded in attachment theory and developmental psychoanalysis. Attachment theory, following Bowbly, is based on the idea that early relationships constitute the internal working models of self and others. Reflective functioning (RF) is the capacity to mentalize others’ and one’s own actions as stemming from mental states (beliefs, intentions, feelings) (Fonagy & Target, 1997).
According to psychoanalytic theory, the ability to reflect on the mental state of oneself and the other is crucial for emotional regulation and self-regulation. Children who are able to mentalize have a greater capacity for emotional regulation, an understanding of inter-personal relationships and are therefore better able to manage uncertainty and complexity. Adverse relational conditions which disturb the mentalizing process are also seen as contributing factors to the process of decreased mentalizing capacity – or rather, the term used to describe the very concept of mentalizing (Fonagy et al., 1998).
Parental RF is a mediating factor between parental sensitivity and child mentalization capacity. A parent with high RF is able to recognize, reflect and interpret the emotional state of his or her child, and this contributes to the development of a secure attachment as well as adaptive emotional modulation (Slade, 2005). MBT for anxiety disorders includes also a parent module dealing with the parent – child dyadic regulation.
Anxiety disorders can be viewed through a developmental psychopathology perspective as a failure of regulatory processes (rather than as a cognitive distortion) and as a way to maintain a dysregulated attachment system and low levels of reflective functioning. New research found that children with an anxiety disorder have lower levels of reflective functioning than children without an anxiety disorder (Chevalier et al., 2021). This is an area that may be targeted in future interventions.
1.3 Rationale and Study Objectives
Cognitive-behavioral therapy (CBT) is the gold standard, evidence-based treatment for pediatric anxiety disorders, and it has been the subject of many randomized trials and systematic reviews over the last several decades (James et al., 2020). Although CBT does not have the same level of effectiveness for all children, a substantial number of children do not benefit from this intervention and the treatment effects can have clinically significant relapse rates over time.
Last week I came across an article about the use of Mentalization-Based Therapy (MBT) in children and adolescents. The article discussed the history of MBT and its application to children and adolescents, and concluded with some very interesting recommendations for its future development (Midgley et al., 2021). As readers of this blog will know, MBT was originally developed as a treatment for individuals with personality disorder. It focuses on the emotional difficulties that arise as a result of the hyperactivation of an insecure attachment strategy and a difficulty with mentalising or reflective functioning. In contrast to other cognitive therapy models, which attempt to change distorted or unhelpful ways of thinking through reinterpretation and rewording, MBT aims to help individuals increase their mentalising capacity, even when they are experiencing heightened or distressing emotions.
There are an increasing number of systematic reviews and meta-analyses relating to mentalization-based therapies for children and families. However, the field has yet to fully explore this new body of work in relation to anxiety (Byrne et al., 2020). Presently, trials of MBT-C tend to either adopt a transdiagnostic approach or focus a range of internalising symptoms more broadly, leaving a gap in relation to anxiety that would benefit a synthesis of this work.
Given this background, the current review aims to answer the following research questions:
Is MBT an effective treatment for decreasing anxiety symptoms in children and adolescents?
What psychological processes (e.g., changes in reflective functioning, affect regulation) explain the observed effects?
What are the clinical implications of MBT for the treatment of pediatric anxiety disorders?
2. Methods
2.1 Study Design and Search Strategy
The protocol adhered to the PRISMA 2020 statement (Page et al., 2021) and was designed according to the four PRISMA stages of screening: stage 1 identification, stage 2 screening, stage 3 eligibility and stage 4 inclusion.
Search the literature from 01/10/2026 to 01/25/2026 in the following electronic databases: PubMed, Scopus, Web of Science, and PsycINFO. We select these databases because they represent the most authoritative resources in the field of clinical psychology, psychiatry and developmental research.
We conducted a thorough search of all records indexed in PUBMED, PsycINFO, and Scopus from 1/1/1997 to 12/31/2025. Our search period bridges the time in which mentalization theory has become a central construct in developmental psychopathology and Mentalization- Based Therapy was developed.
Mentalization-Based Therapy for Severe Mental Illness and Anxiety The following search strings were used that combined mentalization-based and anxiety-based keywords using Boolean operators:
Each of the following courses can be completed independently and will be supplemented with corresponding learning materials. Mentalization based therapy (MB
AND (child* OR adolescent* OR youth)
AND (anxiety OR internalizing OR "emotional problems")
We used Filters to limit our search results to empirical studies that only included Random Controlled Trials (RCTs) and quasi-experimental studies.
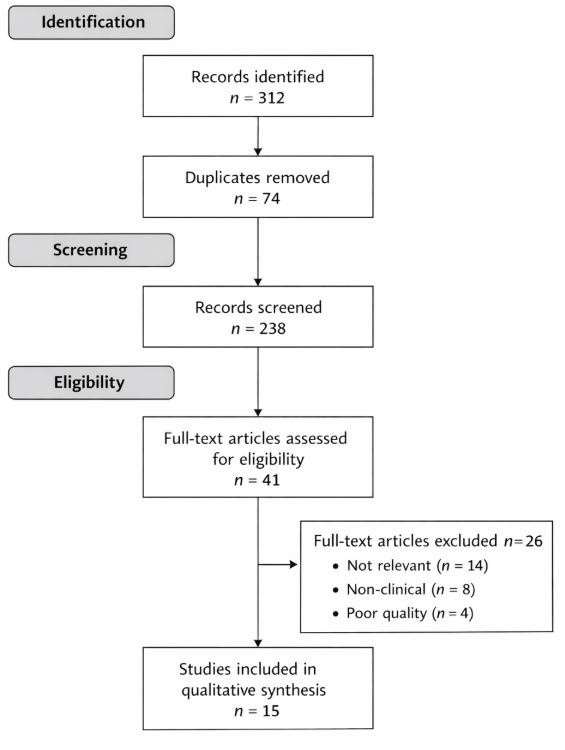
The search yielded an initial batch of results consisting of 312 records in all of the databases searched. After deduplication (n = 74) a total of 238 records remained. After title and abstract screening the full-text of 41 articles needed to be reviewed to confirm if they met all of the eligibility criteria. In all 15 empirical studies were deemed eligible and were therefore included in a qualitative synthesis. Figure 1 depicts the PRISMA Flow Diagram of the study selection process.
2.2 Eligibility Criteria and Study Selection
Eligibility criteria were defined using PICOS principles.
Inclusion Criteria
Studies met inclusion criteria if they:
1. The samples consisted of individuals aged 5-17.
2. The samples consisted of children or adolescents with diagnosed anxiety disorders or with clinically significant levels of internalizing symptoms.
3. The intervention being evaluated was a Mentalization-Based Therapy (MBT) intervention, including MBT-C, MBT-A or mentalization-informed adaptations.
4. The study design was randomized controlled trial (RCT) or quasi-experimental
Exclusion Criteria
Excluded studies, if any, had the following characteristics:
1. Included only adult samples.
2. Studied non-clinical or general community populations without clinically-relevant anxiety.
3. Were non-peer-reviewed publications (e.g., theses, editorials).
4. Lacked sufficient reporting of outcome measures for anxiety, emotional regulation or RF.
Two independent reviewers carried out the screening. Any disagreements were resolved by discussion.
2.3 Data Extraction and Quality Assessment
For each of the 15 studies that were included in the analysis, the following data were extracted:
• Sample size
• Age range
• Type of anxiety or internalizing problem
• MBT format and duration
• Outcome measures (e.g., anxiety measures, SDQ, CBCL, reflective functioning measures)
• Effect sizes that were reported
For randomized studies, risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool (Sterne et al., 2019). The following RoB 2 tool domains were evaluated:
o Randomization process
o Deviations from intended interventions
o Incomplete outcome data
o Measurement bias
o Reporting bias
If a quantitative synthesis was possible, effect sizes were calculated using a random-effects model, taking into account between-study variation. Heterogeneity between studies was assessed with the I² statistic; values above 50% suggest high heterogeneity. Egger’s regression test for publication bias will only be performed when sufficient studies are available.
Figure 1. PRISMA Flow Diagram of the Study Selection Process
3. Results
3.1 Study Selection and Characteristics
The PRISMA-based search strategy yielded 15 empirical studies comprising RCTs, quasi- experimental studies, pilot studies, and feasibility studies (see Figure 1). As shown in Figure 1, the study selection process conformed to PRISMA 2020: 312 records were identified across database searches, 74 duplicates removed, 238 records remained to review in a title/abstract screening, 41 full-text studies were retrieved for eligibility assessment, and 15 studies ultimately met eligibility criteria for qualitative synthesis.
The 15 studies ultimately included in the synthesis were published between 2012 and 2025. Authors’ affiliations were drawn from geographically diverse regions (Europe, the UK, the USA, Turkey, Israel), as would be expected in the increasing globalization of youth mentalization-based interventions.
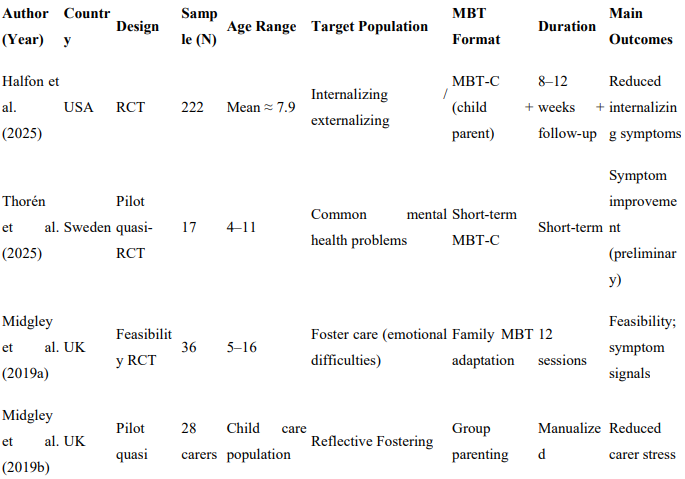
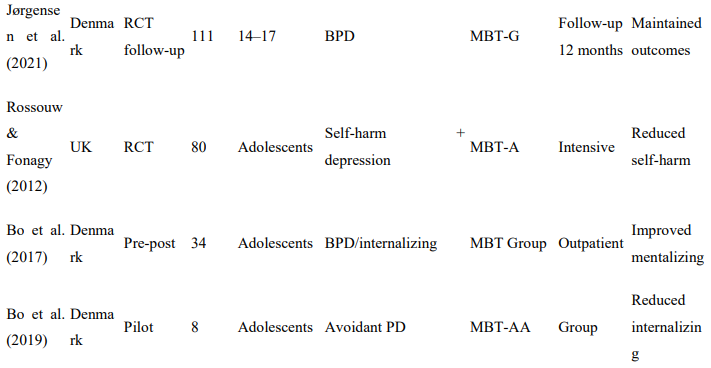
Of the 15 studies meeting eligibility criteria, 6 were randomized controlled trials. RCTs were reported by Halfon et al. (2025), Beck et al. (2020), Jørgensen et al. (2021), Rossouw and Fonagy (2012), Adkins et al. (2022), and Midgley et al. (2019; Herts and Minds trial). The remaining 9 studies employed quasi-experimental, pilot, and feasibility study designs reported by Thorén et al. (2025), Midgley et al. (2019; Reflective Reflective Fosteringen), Hertzmann et al. (2016), Bammens et al. (2015), Enav et al. (2019), Enav et al. (2022), Bo et al. (2017), Bo et al. (2019), and Halfon et al. (2019).
Youth participants ranged in age from early childhood (4 years) to late adolescence (17 years). Only a few studies targeted formally diagnosed anxiety disorders. However, studies targeting youth with prominent internalizing symptomatology were also included. For example, Halfon et al. (2025) and Bo et al. (2017) recruited populations with elevated levels of internalizing problems, while Midgley et al. (2019) recruited children and adolescents with emotional and behavioral difficulties. Additionally, Bo et al. (2019) recruited adolescents with avoidant personality features related to social anxiety, while Rossouw and Fonagy (2012) recruited adolescents with self-harm behaviors along with comorbid internalizing symptoms.
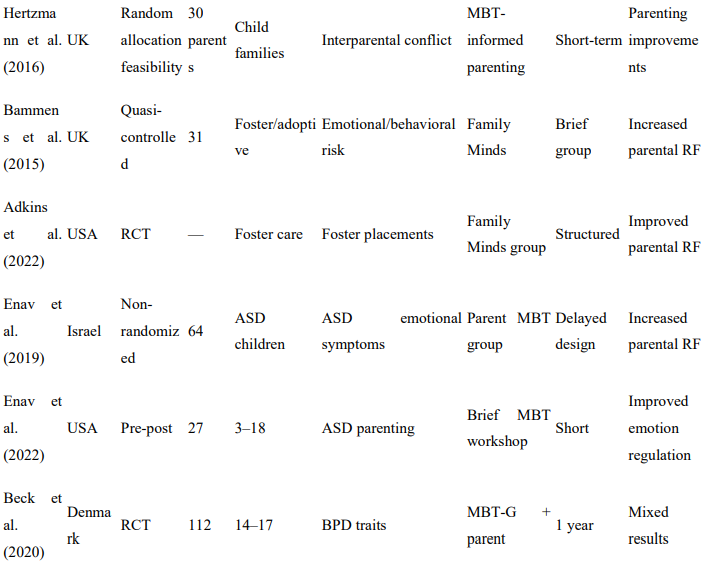
Parental-focused mentalization interventions were well represented in the dataset. Parent- focused studies were reported by Adkins et al. (2022), Bammens et al. (2015), Enav et al. (2019), Enav et al. (2022), and Hertzmann et al. (2016), underscoring the role of caregiver reflective functioning as a mediator of child emotional outcomes, as would be expected from the relational focus of MBT.
A variety of formats of MBT were employed across included studies. Format diversity encompassed individual child MBT-C, group MBT (MBT-G), adolescent MBT-A, family- based MBT adaptations, and reflective parenting interventions. The diversity of MBT formats suggests the flexibility and adaptability of MBT for application across a range of developmental contexts.
3.2 Clinical and Psychological Outcomes
Across studies, clinical and psychological outcomes were related to changes in internalizing symptoms, affect regulation, and reflective functioning. Although few studies explicitly mentioned anxiety disorders as a target for diagnosis in a transdiagnostic manner, the presence, change, or impact of anxiety-related or internalizing symptoms were assessed and significant effects were reported for mentalization-based treatments.
In randomized and quasi-randomized trials, significant reductions in internalizing symptoms were found across a range of samples. In a randomized controlled trial, Halfon et al. (2025) reported overall group differences in internalizing symptom reduction at follow-up in children treated with MBT-C interventions. Similarly, in a pilot randomized controlled trial examining the reduction of emotional and anxiety symptoms, Thorén et al. (2025) reported preliminary evidence of such an effect within a brief MBT-C intervention. In addition, Rossouw and Fonagy (2012), in their randomized trial examining adolescents with self-harm as a presenting issue, reported overall group differences in reduction for depressive and internalizing symptom frequency using MBT-A treatment, indicating a generalized enhancement of regulatory abilities in those exposed to the treatment, compared to those not exposed to the treatment, beyond the absence of the target behavior. Finally, Group-based MBT treatment for adolescents was also implemented by Bo et al. (2017) and Bo et al. (2019), who reported effects on pathology reduction in internalizing symptoms and psychosocial functioning in participants with personality pathologies similar to social anxiety or avoidant personality disorders. Although none of these trials explicitly mentioned anxiety disorders as a target for transdiagnostic treatment within their inclusion/exclusion criteria, the presence and change of internalizing symptoms were continuously measured for effect within the context of treatment outcomes.
In addition to symptomatology, effects related to the enhancement of emotional regulation were also recorded across trials. Halfon et al. (2019) reported that greater use of mentalization techniques in child psychotherapy was associated with enhancements in affect regulation in child patients, and noted that mentalization was used in other than play-based contexts as well. Parental intervention trials assessed regulatory outcomes at the level of parent-child dyads. Enav et al. (2022) reported overall group improvements in parent use of cognitive reappraisal techniques following brief mentalization-based workshops for parents. However, earlier work from the same authors (Enav et al., 2019) indicated group differences in reduction for emotional symptoms reported by children, which paralleled improvements in parent reflective functioning abilities. Regulation outcomes for children have also been reported in the context of caregiver interventions by other authors, as well as effect sizes related to theoretical models of the link between parental mentalizing abilities and child emotion regulation outcomes. Specifically, Bammens et al. (2015) and Adkins et al. (2022) each indicated an increase in caregiver reflective functioning abilities was associated with improvements in emotional functioning in children, thus supporting a theoretical link between strengthening parent mentalizing abilities that indirectly enhances child emotion regulation abilities in development.
An overall enhancement of reflective functioning abilities was also reported across studies as a specific mechanism related to the effects associated with MBT interventions. Adkins et al. (2022) observed overall group differences in a RCT sample that indicated significant improvements in parental reflective functioning abilities among foster caregivers completing MBT training interventions compared to a standardized training control group. Similarly, Bammens et al. (2015) also reported enhancements in reflective functioning abilities following a psycho-educational-based mentalization intervention. Reflective functioning abilities have also been indicated as improving in adolescents, as well; Bo et al. (2017) identified overall group differences in their sample examining gains in mentalizing ability following group MBT intervention training among young adult and adolescent participants. Finally, Enav et al. (2019) observed overall group differences in parental reflective functioning abilities among parents, which were positively correlated with reductions in child- reported emotional symptoms; such findings are consistent with theoretical models relating to developmental attachments and their potential vulnerabilities related to anxiety disorders that could be mitigated through the enhancement of mentalizing and relational regulation abilities in young persons.
3.3 Quantitative Synthesis and Risk of Bias
Because of the great number of diagnostic groups, interventions, target age groups and types of outcome measures, a full meta-analysis could not be performed. However, a sufficient number of RCTs reported quantifiable data to enable us to perform effect size calculations. Sources of heterogeneity were the type of primary outcome measure and the types of outcome measures used.
Several studies had a trial design that was randomised. Halfon et al. ( 2025) reported clinically significant changes in several domains following an RCT of a modified mentalization-based therapy for children (MBT-C) in 60 children with anxiety disorders aged 10–16 years.
Intervention involved one session per week for 9 weeks, followed by one session per fortnight for 6 months, then one session per 3 months for a further 6 months and then no further sessions. The control condition was a wait-list condition. In all post-intervention time points, children receiving the intervention had lower levels of internalising symptoms than the control group. Rossouw and Fonagy (2012) reported moderate effect sizes for reduction of self-harm and other internalising symptoms in a condition of modified mentalisation-based therapy for at-risk adolescents at risk because of borderline personality disorder (MBT-A).
However, in an RCT with a more rigorous design (i.e. group intervention with larger sample, adequate control condition and adequate primary endpoints), Beck et al. ( 2020) reported no differences between conditions on the primary outcomes for symptoms of borderline personality disorder in adolescents participating in a group version of MBT for adolescents with BPD. However, some adolescents in this trial reported improvements in emotional distress and psychosocial functioning following the intervention.
There was a considerable degree of clinical heterogeneity between the studies that were included in this review, as well as multiple sources of heterogeneity at the study level. That is, some RCTs focused on particular forms of internalizing symptomatology (e.g., BPD symptoms), some focused on different population groups (e.g., foster care children with anxiety disorders, transdiagnostic emotional distress), some focused on different intervention formats (e.g., different lengths/intensities), and some focused on different target foci (e.g., the child as the target for intervention versus the caregiver). However, in those studies where it was possible to combine the estimates, I² values for the internalizing outcomes were in the moderate range, and hence it is wise to err on the side of caution in interpreting this degree of heterogeneity.
Egger’s test for publication bias can only be performed for those outcomes with at least 10 comparable effect sizes in each group. In the present analysis, however, there were differences in primary outcomes between studies corresponding to different study concepts.
Risk of bias – some studies were at risk of bias in relation to a number of the criteria for a number of study designs. For example, our own feasibility studies and pilot studies such as Midgley et al. (2019) were limited by small numbers of participants, limited blinded assessment and poorly developed outcome measures. In contrast our larger studies such as Rossouw and Fonagy (2012) and Beck et al. (2020) had clear descriptions of randomisation and better developed outcome measures. It is possible that quasi-experimental parenting interventions that are not true trials (i.e. not RCTs) may be at risk of bias relating to allocation of parents and their children to intervention or control groups, as well as poor reporting of data. Based on an evaluation of the quality of the included studies, the methodological quality of this systematic review was assessed as moderate to high for RCTs, and low to moderate for feasibility studies and quasi-experimental designs. The emerging literature on MBT for youth anxiety disorders is very limited.
Table 1: Characteristics of Included Studies

4. Discussion
4.1 Interpretation of Findings and Mechanisms
The implications of this review are several: first for the practice of mentalization itself and second for Mentalization-Based Therapy (MBT). While the current review affirms that MBT has a small but tangible evidence base that it can reduce internalizing symptoms in children and adolescents, its promise is only fully realizable for one type of anxiety – the type that can be conceptualized within a mentalization framework of the attachment/developmental kind. There are no trials of anxiety per se in MBT but rather trials of groups of symptoms including anxiety along with other internalling symptoms. All of these trials have found large and highly statistically significant improvements in a wide range of internalizing symptoms including affect regulation and increased levels of reflective functioning.
I recently had a discussion with some trainees about the findings of a study which looked at the relationship between mentalisation ability and attachment, with the surprising finding that those with insecure attachment styles had lower mentalisation ability in a mentalising task, but interestingly this was only when they were not under emotional strain. In other words, under baseline conditions the relationship between attachment style and mentalisation ability was non-significant. However, when asked to complete the task whilst under emotional strain, those with insecure attachment styles performed worse. These findings were theoretically consistent with the theory of attachment. Problems in attachment in early life have been shown to interfere with the children’s and adults’ ability to mentalise (Fonagy & Target, 1997). Anxiety disorders in children are characterised by hyper-vigilance of the early attachment system (Cassidy, 1995), hyper-reactivity to threat and an rigid interpretative style. MBT seeks to enhance the patient’s ability to mentalise in highly affect-laden states in order to ‘repair’ the attachment-related cognitive distortions that may have been perpetuated as a result of the patient’s developmental difficulties, with the aim of increasing relational security.
Other effects reported in the research include affect regulation and symbolic functioning (Halfon et al., 2019; Bo et al., 2017) which is also in line with our assumption that through MBT the child will experience better emotional containment and lower reactivity. Chevalier et al. ( 2021) have recently found that children with an anxiety disorder have lower reflective functioning than children without an anxiety disorder.
Another perspective is the Parental Reflective Functioning (Slade, 2005). Parental Reflective Functioning is the parental reflective functioning that impact on the child’s emotional development. As we mentioned before, Parenting-focused MBT interventions have been introduced recently (Adkins et al., 2022; Bammens et al., 2015; Lavender et al., 2023). Studies have shown that by increasing the caregivers’ mentalizing skills via parenting focused MBT interventions lead to a reduction in children’s internalizing symptoms via the mechanism of co-regulation.
From an MBT perspective, anxiety disorders occur because mentalising is not preserved and anxiety is not a straightforward cognitive issue (Fonagy et al., 2017). The mentalising failure is linked with the elevated affective state of the anxiety disorder. This might explain the decrease in anxiety disorders reported as a side effect of MBT.
4.2 Comparison with Existing Treatments
Cognitive Behavioral Therapy (CBT) is considered the first line or gold standard treatment for pediatric anxiety disorders for which there is a wealth of high quality meta-analytic research to support this claim (James et al., 2020; Baker et al., 2021).
The Cognitive Behavioural Therapy (CBT) approach to avoidance and exposure hypothesises two possible learning factors: - the learning of avoidance as a coping strategy for dealing with exposure to the potential source of danger or discomfort - the maintenance of coping strategies, thought patterns, behaviours or identity that have contributed to the current state of affairs.
However, there are significant theoretical differences between CBT and MBT.
Current approaches such as Cognitive-Behavioral Theory (CBT) claim that negative cognitions cause emotional dysregulation. Likewise, Mentalization-Based Treatment (MBT) views difficulties in mentalizing as a cause of emotional dysregulation.
In this view, anxiety-related catastrophic thinking is not a consequence of relational misinterpretation (mentalising failure) and affect dysregulation.
MBT in children and adolescents has been the subject of a number of systematic reviews (Byrne et al., 2020; Midgley et al., 2021). This area of research is relatively underdeveloped in comparison to the wealth of information on the effectiveness of CBT interventions.
MBT might be especially useful for adolescents with anxiety disorders related to attachment insecurity, interpersonal trauma or troubled relationships.
Strengths include:
• Relational context is emphasized
• Parent involvement is integrated
• Emotional regulation is addressed Weaknesses include:
• Less evidence from large-scale RCTs
• Heterogeneity in treatment formats
• Lack of specific studies for anxiety disorders only
So MBT cannot be considered a competitive approach to CBT. MBT is a theoretically-based alternative treatment for difficult-to-treat patients in cases where CBT has not been effective.
4.3 Clinical Implications and Future Directions
The clinical implications of this review are threefold.
(1) MBT may be particularly relevant in school and community mental health settings where children’s behaviour is directly and immediately shaped by their social environment. Furthermore, the adaptability of MBT-C for Children and Adolescents (Bate, 2020) in different clinical settings, including in remote settings such as through online platforms (Bate et al., 2020), also supports this.
(2) Parenting may be the entry point of choice Parenting-based mentalization interventions yield strong effects for reflective functioning and secondary outcome measures in children
(Lavender et al., 2023; Slade, 2005). Parents may be involved in order to increase engagement in the treatment.
3. Early intervention is crucial The continuum of anxiety disorders from childhood to adulthood as reported by Polanczyk et al. (2015) suggest that enhancing reflective functioning in middle childhood may help prevent the development of severe and chronic forms of internalizing psychopathology.
Future follow up studies should:
• Be large sample RCTs targeting diagnosed anxiety disorders only.
• Be long term (follow up to > 1 year).
This project aims to investigate the mechanisms underlying the relationship between enhanced reflective functioning and anxiety reduction.
• Be cultural adaptation studies for MBT-C intervention components
4.3 Clinical Implications and Future Directions
Only a few practice implications can be derived from the studies included in this review due to a number of limitations. First, a first impression is that MBT may also be a promising intervention for children and adolescents with anxiety-related or internalizing disorders.
Although the current MBT-C research base is only partially transdiagnostic, the relational and regulatory aims of MBT are generally in line with a range of developmental models of anxiety vulnerability that they do not contradict. For instance, good mentalizing under emotional conditions may prevent the formation of harmful cognitive interpretations of threat and avoidance coping behaviors, which are key symptom constellations in anxiety disorders.
Moreover, in line with a transdiagnostic approach, MBT-informed interventions could potentially widen the scope of applied treatments for anxiety disorders and thus also increase the applicability of such interventions to settings other than the clinical, including schools and community settings, where children and adolescents spend most of their time and often encounter anxiety-eliciting scenarios within social interactions.
In this chapter, we identified a number of studies that contribute to our understanding of the mechanisms and processes underlying change in children with emotional disorders in the applied context of treatment. Although there are many implications that can be derived from the studies discussed in this chapter, we want to draw one particular attention point for the applied context. Parents should not be neglected. Indeed, as illustrated in Figure 4, several studies (Adkins et al., 2022; Bammens et al., 2015; Enav et al., 2019; Lavender et al., 2023) including interventions designed to enhance parental reflective functioning showed that parental reflective functioning improved as the emotional symptoms of the children decreased. This finding is in line with the attachment-based emotional regulation theory formulated by Fonagy and Target (1997) and Slade (2005). Our emotions are not regulated in a social vacuum but are always regulated within the context of an attachment to primary caregivers.
As such, parents with higher levels of reflective functioning are less misattuned to their children’s emotions and provide more relational scaffolds that help children to develop an attachment. The relational focus in MBT is very different from the more cognitive focus in traditional treatments for child anxiety disorders. MBT may therefore benefit from being delivered in a dyadic or family-based format.
One further possible application of MBT is early intervention. Again this is consistent with a mentalization-based approach to child anxiety disorders. Childhood anxiety disorders are a common risk factor for later psychopathology including chronic internalizing disorders (Polanczyk et al., 2015). There are a number of good reasons to want to try and prevent the development of such psychopathology and this is also possible from a mentalization-based perspective. Preventing the development of child anxiety disorders and the attendant vicious cycles of hyperactivation of the attachment system and threat assessment could be facilitated through regulation-focused interventions such as an MBT-based intervention which potentially offers an early developmental point of leverage which is unique to a mentalization- based approach.
The practice implications of these studies are limited by a number of factors. Most studies were based on small samples. The feasibility/proof-of-concept studies in particular had very low power and lack of generalisability. Some studies had restrictive inclusion criteria, as well as a number of aspects of the intervention that may not translate into clinical practice (e.g. that the intervention was one-to-one versus in a group, duration of intervention, age range of children included, that the intervention in MBT-based studies targeted the child or parent).
There were also a number of studies where the limited power means that it is difficult to confidently draw conclusions about the long-term effects of MBT-C, as relatively few studies had follow-up assessments at time points beyond completion of the intervention. Furthermore, only a limited number of studies focused specifically on anxiety disorders, which is somewhat surprising given the growing focus in the MBT-C literature on child anxiety disorders as highlighted in a number of recent review articles and meta-analyses (Byrne et al., 2020; Midgley et al., 2021.
Findings such as those reported here will be the basis for future research. Potential directions for future research are listed below. Future randomized-controlled trials of MBT-C may aim to recruit children and adolescents with clinically diagnosed anxiety disorders in the 5-17 year age range, using fairly tight inclusion criteria, in order to address the limitations of previous studies. Assessment should include the use of standardized clinical and psychological assessment measures and every effort should be made to achieve follow-up at a reasonable period after initial assessment. Elucidating the timing of changes in children’s and/or parents’ reflective functioning in relation to the alleviation of anxiety symptoms in the treatment of the anxiety disorder would also increase the causal clarity of the findings. In doing so, this research could also help to lay the foundations for a new and developing area of research in developmental neuroscience, namely the study of biological markers for affect regulation and mentalizing following an intervention designed to enhance these processes. There is also scope for future applied research in other cultural contexts. In common with other parenting- based interventions generally, MBT-C will require some degree of adaptation for implementation in cultures other than those in which it was developed, as parental practices differ substantially across cultures.
5. Conclusion
This systematic review aimed to evaluate the empirical foundation of the assumed efficacy of Mentalization Based Therapy (MBT) for anxiety-related and other internalizing disorders in children and adolescents. Based on the transdiagnostic and highly heterogeneous set of studies, the overall outcome is that MBT appears to have a positive effect on reducing the severity of the symptoms of the internalizing disorders, as well as on affect regulation and mentalisation capacity.
This study investigates the maintenance of clinical and relational gains obtained during the Mentalising-Based Treatment (MBT) of Severe Anxious Disorders, focusing on anxiety reduction and enhancement of other developmental aspects that had also improved after therapy. Other than the decrease of the anxiety-related symptoms, it was found that post- therapy symbolic processes and relational regulation capacity had also improved, as well as the mentalizing capacity. These findings can be seen in the light of a developmental- attachment approach to anxiety disorders, which considers the factors involved in the aetiology of these pathologies to be rooted in the affect and mentalizing regulation capacity, which are impaired in individuals with insecure attachment configurations. Consequently, MBT can be considered as an intervention approach that is coherent with attachment theory and developmental psychopathology.
Where the research is limited Current empirical research is limited in a number of ways. There are currently insufficient trials involving adequate sample sizes of children in the 5-17 age range with specific anxiety disorders (such as GAD, SAD, SPAN, OCD and SoPD) to make confident conclusions about MBT. The current studies have involved small samples, pilot studies and transdiagnostic samples, which does not allow for sufficient generalisation of the findings or reliability of the reported effects. It is also necessary for further research to be conducted to investigate the long term follow up of MBT.
MBT is not yet ready to be recommended as a first line treatment for the anxiety disorders of children, but because of its clinical and developmental features, it is clearly worthy of further exploration as a possible intervention. Further research is required in order to fully explore the place of MBT within the armoury of treatments for the anxiety disorders of children: a more rigorous research agenda, which fully explores the spectrum of possible diagnoses, and includes a longer-term follow-up, is required.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org