Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Ali Ahmad, M.D*., Halina Kusz, M.D., Yousaf Ahmad
Faculty of Health Sciences, McMaster University, Hamilton, ON, Canada; Grey Bruce Geriatric Services, Brightshores Health System, Owen Sound, ON, Canada.
*Corresponding author: Ali Ahmad, Faculty of Health Sciences, McMaster University, Hamilton, ON, Canada; Grey Bruce Geriatric Services, Brightshores Health System, Owen Sound, ON, Canada.
Received: March 05, 2026 | Accepted: March 11, 2026 | Published: March 16, 2026
Citation: Ahmad A., Kusz H., Ahmad Y. (2026) “Impending Rupture of an Infected Abdominal Aortic Aneurysm - A Rare Sequelae of Salmonella Bacteremia” Clinical Case Reports and Clinical Study, 13(2); DOI: 10.61148/2766-8614/JCCRCS/234.
Copyright: © 2026 Ali Ahmad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Infectious aortitis is a very rare and life-threatening condition caused by microorganisms in the aortic wall which can precipitate aortic aneurysm and rupture.1 Infected aortic aneurysms only account for about 0.7-2.6% of all cases of aortic aneurysm.1,2 However, it has a mortality of 96-100% with medical treatment alone, and 40% with combined medical and surgical treatment.2 The presentation is often nonspecific and requires high clinical suspicion.3 Diagnosis of infectious aortitis may be suggested by positive blood cultures and abdominal CT findings.1,3 We present a rare case of an abdominal aortic aneurysm that was complicated by Salmonella bacteremia, leading to infectious aortitis and impending rupture.
Infectious aortitis; bacteremia; medical and surgical treatment
Background:
Infectious aortitis is a very rare and life-threatening condition caused by microorganisms in the aortic wall which can precipitate aortic aneurysm and rupture.1 Infected aortic aneurysms only account for about 0.7-2.6% of all cases of aortic aneurysm.1,2 However, it has a mortality of 96-100% with medical treatment alone, and 40% with combined medical and surgical treatment.2 The presentation is often nonspecific and requires high clinical suspicion.3 Diagnosis of infectious aortitis may be suggested by positive blood cultures and abdominal CT findings.1,3 We present a rare case of an abdominal aortic aneurysm that was complicated by Salmonella bacteremia, leading to infectious aortitis and impending rupture.
Case Summary:
A 56-year-old Caucasian male, with prior history of chronic obstructive pulmonary disease and nicotine dependence presented to the hospital with shortness of breath, productive cough, with fever and chills. He was found to be in acute exacerbation secondary to right basilar pneumonia and initiated on treatment. As part of the initial workup, computerized tomography (CT) scan of the chest and abdomen was also ordered, which revealed an incidental finding of an infrarenal abdominal aortic aneurysm, measuring 5.1 x 5.1cm x 10.4cm. Blood cultures ordered on admission returned positive for Salmonella enteritidis, which was sensitive to ceftriaxone, and appropriate antibiotic treatment was initiated.
The patient subsequently began to develop abdominal discomfort and new fever spikes. Repeat lab findings showed an increased leukocyte count, and CT angiogram demonstrated a significantly increased size to 7.6 x 9.1 x 13.3cm, concerning for impending rupture and underlying aortitis. Nuclear white blood cell scan was performed and revealed abnormal increased uptake involving the mid and distal abdominal aorta, suggestive of infection. Vascular consultation was obtained, and he successfully underwent percutaneous endovascular aortic repair. He tolerated the surgery well and observed improvement in symptoms, following which he was discharged.
Discussion:
Infectious aortitis is a very rare condition, which manifests as endovascular inflammation due to microorganisms.1 Common organisms identified are Gram-positive, such as Staphylococcus, Streptococcus, Enterococcus or Gram-negative, such as Salmonella.1 Salmonella is a Gram-negative, facultative anaerobic bacillus that is typically implicated in gastroenteritis and bacteremia, however it accounts for 40% of infectious aortitis.1,4,5 The infrarenal aorta is more susceptible to infection, as seen in this case.2
Infectious aortitis has a significant mortality rate. It ranges from 11 to 36% in patients who are treated with both antibiotics and surgery, compared to upwards of 90% in patients treated without surgical intervention.6 Although the intimal layer of the aorta is resistant to infections, underlying atherosclerosis poses a significant risk factor.1 Other risk factors for infectious aortitis include male gender, age above fifty years, diabetes mellitus, hypertension, coronary artery disease.3,6
Infectious aortitis may occur due to various underlying etiologies (Figure 1) and can be complicated by aneurysmal formation due to bacterial enzymatic degradation of elastic fibers damaging the aortic wall.1 Symptoms may include fevers, chills, diarrhea, back and abdominal pain.3 Diagnosis requires high suspicion and should be considered in patients with Salmonella bacteremia, risk factors, and laboratory findings (leukocytosis, elevated inflammatory markers).7 Abdominal CT with contrast is imaging of choice, and may reveal mural thickening, periaortic gas, soft tissue density, fluid retention or aneurysm.1,8 Treatment requires empiric intravenous antibiotics for 6-12 weeks after negative blood cultures, and resection of infected segment.1,2
Conclusion:
Although Salmonella aortitis is rarely seen in clinical setting, it is associated with rapid growth and an increased risk of rupture and death. Therefore, early diagnosis and prompt treatment with antibacterial therapy and surgical intervention is imperative.
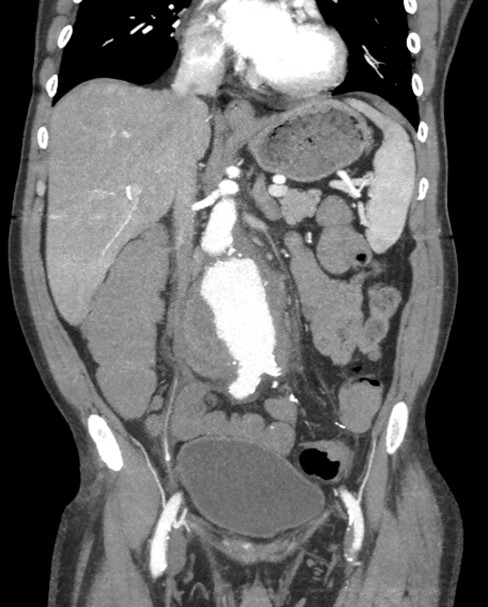
Image 1: Abdominal CT scan with contrast (Coronal plane) demonstrating Abdominal aortic aneurysm.
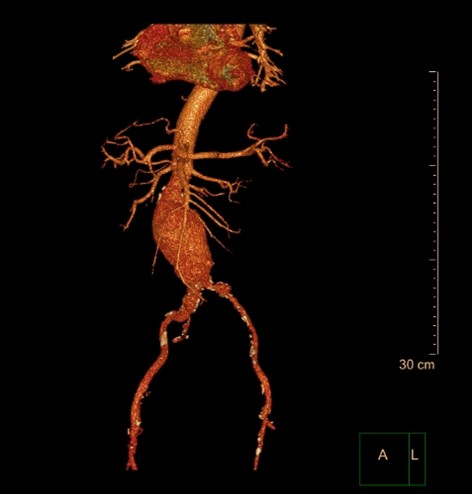
Image 2: 3D Reconstruction of CT of Abdominal Aortic Aneurysm.
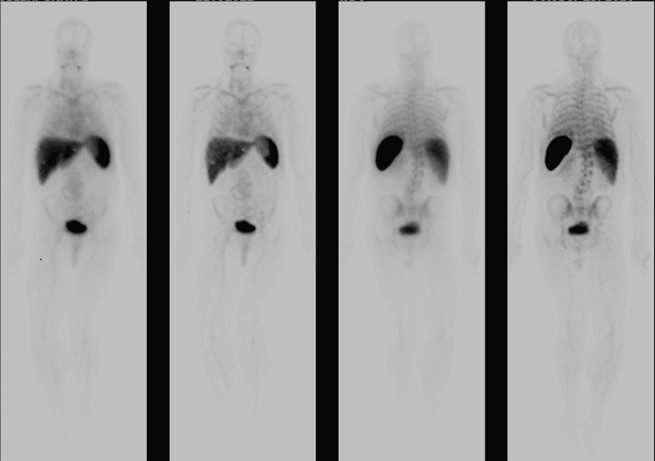
Image 3: Tagged White Blood Cell Scan.

Image 4: Tagged White Blood Cell Scan of Abdomen shows increased uptake in Abdominal Aorta.
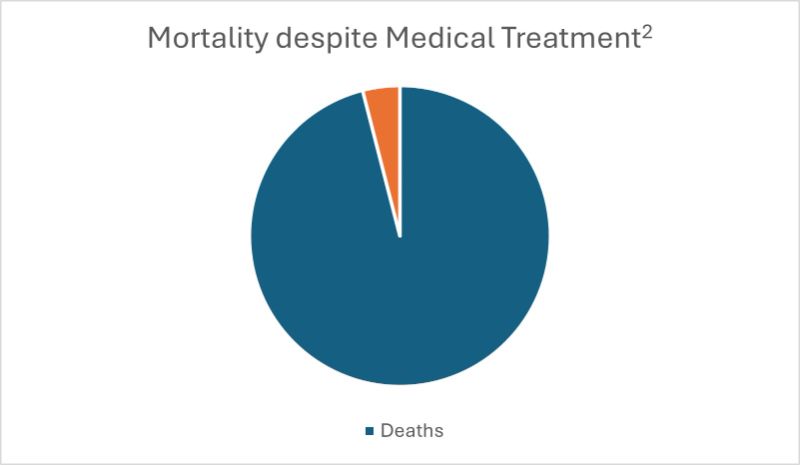
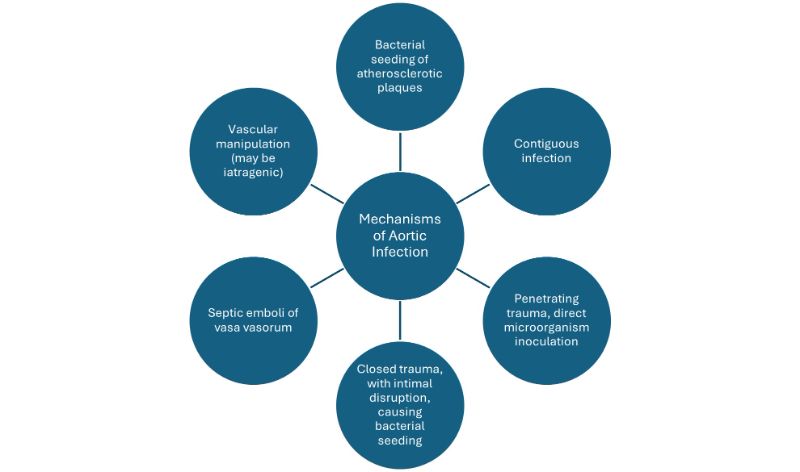
Figure 1: Mechanisms of Aortic Infection. 1,9,10














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org