Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 12 - Issue 5 - 2025
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Natalia Sayeg, BA, DMD, Liliana MosqueraDDS, MS, MBA*, Mauricio Schneider, DDS, MS, Alexander Bendayan DDS, CAGS, MBA, MSEd, Nydia Cummings, PHD
Nova Southeastern University, College of Dental Medicine, Fort Lauderdale, FL.
*Corresponding author: Liliana Mosquera DDS, MS, MBA, Nova Southeastern University, College of Dental Medicine, Fort Lauderdale, FL.
Received: November 20, 2025 | Accepted: November 28, 2025 | Published: December 08, 2025
Citation: Sayeg N, Mosquera L, Schneider M, Bendayan A, Cummings N. (2025) “Ergonomic Posture Behavior on Dental Students after Receiving Instructional Information: A Pilot Study” Clinical Case Reports and Clinical Study, 12(5); DOI: 10.61148/2766-8614/JCCRCS/225.
Copyright: © 2025 Liliana Mosquera. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Poor ergonomics in dentistry contributes to musculoskeletal disorders in dental professionals over time. Incorrect posture can lead to pain in the neck, back, shoulders, elbows, etc. (5). The worldwide prevalence of musculoskeletal disorders in dentistry ranges from 63 to 93% (8). Students’ postural habits typically develop early on in their academic career carrying over to their professional tenure (3). Therefore, promoting proper ergonomics in dental school curriculum is advisable aiming for a healthier lifestyle for dentists throughout their career as supported in the literature. Although ergonomics is an important part of education in dentistry there are no consistent standards for dental education. This pilot was intended to initiate curriculum content beyond the classroom.
dentistry
Problem:
Poor ergonomics in dentistry contributes to musculoskeletal disorders in dental professionals over time. Incorrect posture can lead to pain in the neck, back, shoulders, elbows, etc. (5). The worldwide prevalence of musculoskeletal disorders in dentistry ranges from 63 to 93% (8). Students’ postural habits typically develop early on in their academic career carrying over to their professional tenure (3). Therefore, promoting proper ergonomics in dental school curriculum is advisable aiming for a healthier lifestyle for dentists throughout their career as supported in the literature. Although ergonomics is an important part of education in dentistry there are no consistent standards for dental education. This pilot was intended to initiate curriculum content beyond the classroom.
Solution:
A Pilot study was executed with the purpose of investigating changes in predoctoral dental student’s ergonomic posture after intervention during fixed prosthodontic procedures utilizing an educational flyer for Predental dental students in the clinic reinforcing their prior basic didactic education on ergonomics in the classroom and during simulation sessions. Assessing the proper ergonomics intervention needs will justify the implementation of prevention programs that reinforce proper posture during clinical experiences in the predoctoral curriculum.
Participants qualifications for the study included: Third year NSU-CDM students with dominant right hand, performing seated fixed prosthodontics using loupes. The intervention was done as follows:
Pre-observation phase: A faculty member obtained posture assessment during the three (3) hour clinic session using the Rapid Upper Limb Assessment (RULA) observational tool that considers ergonomic clinical best practices. It uses subcategories of scores for different upper limb body parts position, movement and frequency and a total upper limb score (figure 1):
1–2: Posture is acceptable if not maintained.
3–4: Further investigation needed. May need changes. 5–6: Further investigation and changes needed soon. 7: Investigation and changes required immediately
Figure 2. shows the Ergonomics RULA Assessment form steps developed by the NSU Prosthodontics Department for use during the observations.
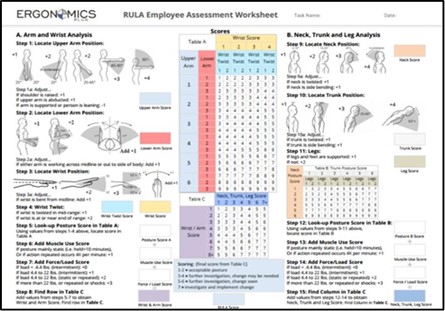
Figure 1: RULA Assessment Worksheet from Ergonomics Plus, based on RULA: a survey method for the investigation of work-related upper limb disorders, McAtamney & Corlett, Applied Ergonomics 1993, 24(2):91-99.

Fig 2: Ergonomics RULA Assessment form steps
A Participant Qualification Instrument and Preliminary Questionnaire was completed prior, which included: biological sex, the quadrant involved, appointment length and presence of assistant or not during the procedure.
Intervention phase: After the pre-observation appointment, participants received an educational flyer on proper ergonomics (Figure 3) for review prior to their next scheduled observation.
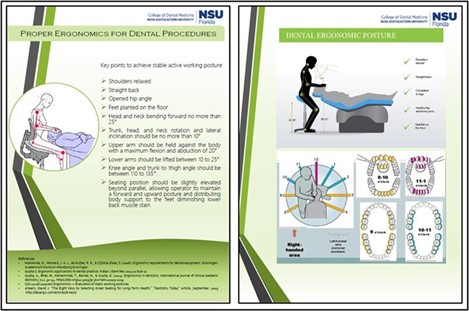
Figure 3: Interventional Informative Flyer on proper ergonomics for dental procedures
Post-observations phase: Same conditions as the pre-observation phase were repeated for each participant and the second observation was scheduled no later than 2 weeks after the first one.
Results:
A total of eight participants were observed. The total RULA pre-observation assessment scores varied from 5-7 while post-observation assessment varied from 3-6. Five participants improved their scores after the flyer intervention. This evidences an overall need for further investigation and improvement in students’ ergonomic scores.
The trunk and neck presented the least acceptable pre-observation scores and showed the best score improvement after the informative flyer intervention. The trunk was the body part most positively affected with improved scores after intervention.
The arm scores improved in three participants and the Wrist scores improved in two participants. The body part with the most acceptable overall initial RULA scores was the lower arm, and none of the participants showed any improved scores.
All participants showed leg and feet supported and balanced in the post-observation assessment and three participants improved lower limb support as compared to the Pre- observation.
Pre and Post RULA scores are summarized in Fig 4.
Initial pre-observation total RULA scores (above 5) justifies further investigation and the need for posture change intervention and reinforcement. The educational flyer showed improvement for the post-observation scores, but not to a fully acceptable ergonomic posture according to the RULA scale.
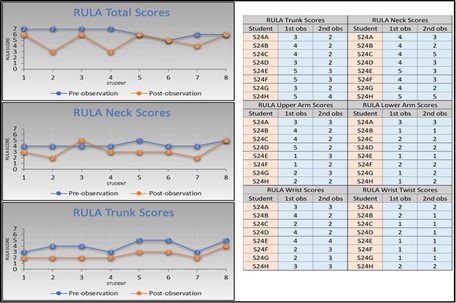
Figure 4: Pre- and post-RULA total score, RULA Neck Scores, RULA Trunk and RULA Body parts scores for each student participant
Whitin the limitations of this Pilot study in the sample size, the purpose of testing the feasibility of measuring NSU-CDM dental students’ ergonomics posture was achieved. A more extensive study will follow to achieve statistically significant data on the ergonomic posture of NSU-CDM dental students when performing seated prosthodontics appointments.
Conclusions: The need for further data on this study was deemed necessary and has now expanded to a research project for clinical and preclinical education. The Rapid Upper Limb Assessment instrument will continue to be utilized as a reliable observation tool for both research and education.
Acknowledgments:
The authors wish to thank the students of Nova Southeastern University College of Dental Medicine for their participation and consent to be observed in this study, without which this study would not have been feasible.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org