Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Basema A. O. Khabaz1, Abdulwahab I. Al-Kholani1*, Ibrahim Zaid Al-Shami1, Abduljabbar M Al-Sameai2
1Department of Restorative and Esthetic Dentistry, Faculty of Dentistry, Sana’a University, Yemen
2Oral Medicine, Oral Diagnosis, Periodontology and Oral Radiology Department, Faculty of Dentistry, Sana’a University, Yemen.
*Corresponding Author: Abdulwahab Ismail Al-Kholani, Department of Restorative and Esthetic Dentistry, Faculty of Dentistry, Sana’a University, Yemen.
Received: February 26, 2023
Accepted: March 01, 2023
Published: March 03, 2023
Citation: Basema A. O. Khabaz, Abdulwahab I. Al-Kholani1, Ibrahim Zaid Al-Shami, Abduljabbar M Al-Sameai (2023) “Morphometric Relationships between Permanent Maxillary Central Incisors and Face Among a Sample of Yemeni Population”, Clinical Case Reports and Clinical Study, 1(9); DOI: http;//doi.org/03.2023/1.164.
Copyright: © 2023 Abdulwahab Ismail Al-Kholani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Background: The ultimate goal of aesthetic rehabilitation is to design a pleasant smile with teeth that have an inherent proportion and arrangement suitable in harmony with the gum and face.
Objective: To evaluate the morphometric relationships between permanent maxillary central incisors (MCIs) and face among a sample of Yemeni adults.
Material and methods: A prospective cross-sectional study was conducted on male and female Yemeni adults attended to the clinics of faculties of Dentistry and Medicine and Health Sciences, Sana’a University, Yemen during the period between January and March 2022. The sample were conveniently selected as per inclusion and exclusion criteria. The data included intraoral photographs for determining maxillary central incisors shapes and extraoral photographs for determining face shapes. The data collection process took a period of 6 months; from April to September 2022. SPSS was used for data analysis.
Results: A total of 315 participants with a mean age of 21.78 ± 2.29 were frequently distributed according to gender, face shape (brachyfacial, mesofacial, and dolichofacial), and MCIs form (square, ovoid, and triangular). Males were about three fourths of the total sample (234, 74.3%) compared to females (81, 25.7%). The brachyfacial shape was observed significantly more in males (21.4%) than females (3.7%), whereas the dolichofacial shape was observed significantly more in females (46.9%) than males (29.1%) (p<0.05). However, the mesofacial shape was equally observed in both genders (male, 49.6%; female, 49.4%). Moreover, the triangular MCIs shape was observed significantly more in males than females (53.4% vs 32.1%), whereas the ovoid and square MCIs shapes were observed significnatly more in females than males (43.2% vs 27.8% and 24.7% vs 18.8%, respectively) (p<0.05). The correlated cases were significantly less than non-correlated cases (129, 41% vs 186, 59%; p=0.003). Among the 129 correlated cases of both genders, the mesofacial/ovoid MCIs shape was the predominant (59, 45.7%), followed by the dolichofacial/triangular MCIs (56, 43.4%), then the brachyfacial/square MCIs (14, 10.9%). In addition, there are no statistically significant association of the correlated cases and gender (p=0.096). Furthermore, no significant association was observed between various face and MCIs shapes (p=0.184).
Conclusions: There are no significant morphometric relationships between face and MCIs among the studied Yemeni sample because nearly three‑fifths of the study sample showed no correlation between MCIs and face shapes. Besides, the study findings contradict Williams’ theory regarding the presence of harmony between the face and MCIs shapes; therefore, this method is not reliable for selecting artificial MCIs tooth shapes for edentulous Yemeni patients.
Introduction
The social attractiveness of individuals could be influenced by their dental-facial appearance (1). Several patients nowadays undergo dental treatments for solving their concerns about dental appearance since seeing patients with tooth defects or multiple missing anterior teeth is common in the esthetic dentistry practice. For a successful esthetic treatment, it is extremely essential to identify the dimensions of restorations for these anterior teeth, especially the maxillary central incisors (MCIs) (2), which are the most dominant in the anterior area when speaking or smiling (3). A precise knowledge of the esthetics of natural anterior teeth is necessary for dental treatments in the esthetic zone (2).
Although the teeth must be in proportion to one another, they must also be in proportion to the face. A great variation in the size of the tooth in relation to the face may affect the ability to obtain a good esthetic appearance (4,5). A balanced proportion in the appearance of the teeth is fundamental to compose an esthetical pleasance (6).
Therefore, several methods have been suggested to identify the shape of central incisors, including the correlation between the inverted shape of the face and the shape of the upper permanent central incisors which was called “law of harmony” and confirmed by other scholars (7,8).
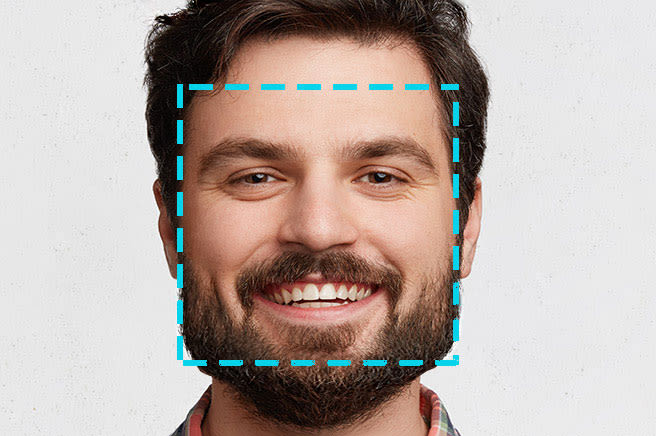
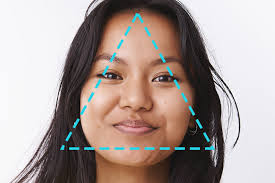
Face can be classified into three specific shapes which are square, oval and triangular (9,10), which correspond to brachyfacial, mesofacial and dolichofacial respectively (Figure 1).
|
|
|
|
|
a. Square (brachyfacial) |
b. Oval (mesofacial) |
c. Triangular (dolichofacial) |
Figure 1: Classification of face shape (11)
The MCIs shape was classified by Kina and Bruguera (12) into square, triangular and oval (Figure 2).
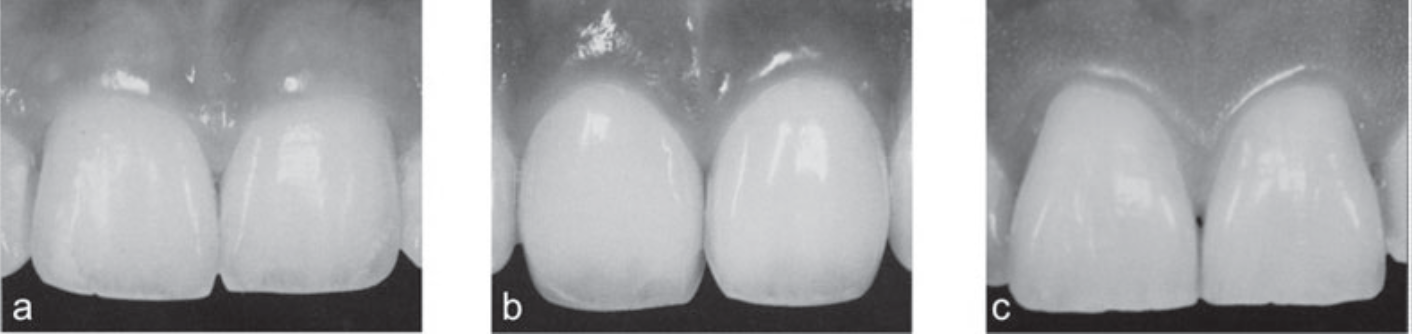
Figure 2: Dental morphology of MCIs: a. Square, b. Oval, and c. Triangular (13)
Even today, there are authors who recommend the determination of the shape of prosthetic reconstructions or the selection of artificial teeth from a facial analysis (14-16), not only taking the shape of the face contour as a reference (14,17), but also considering gender (16,18). However, there is neither agreement worldwide on such an approach nor a standard protocol for such an analysis (7).
The ultimate goal of aesthetic rehabilitation is to design a pleasant smile with teeth that have an inherent proportion and arrangement suitable in harmony with the gum and face (19).
Therefore, the present study was conducted to determine the morpho-dimensional relationship between the permanent maxillary central incisors and the face among the Yemeni adult population in order to come up with a guideline or normative data which may help dentists in facilitating esthetic or restorative treatments.
Materials and methods
This is an observational cross-sectional study, conducted in the outpatient clinics of faculties of Dentistry and Medicine and Health Sciences, Sana’a University, Yemen. The study population represented all male and female Yemeni adults attended to the outpatient clinics of faculties of Dentistry and Medicine and Health Sciences, Sana’a University, Yemen during the period from March to December 2021. Therefore, the study population included 1530 individuals. Of them, only 315 individuals were eligible to be participated in the study according to identifiable inclusion and exclusion criteria.
Inclusion and exclusion criteria
Only Yemeni male or female adults with fully erupted permanent MCIs. However, individuals with incompletely erupted MCIs, crowding, decay, restoration, abrasion, fracture or diastema in MCIs, congenital or mal-shaped MCIs, gingival or periodontal problems in the anterior teeth, dentofacial deformities, previous or ongoing orthodontic treatment or proximal stripping, or characteristics which could alter the contour of the face were excluded.
Bioethical considerations
An ethical approval from the Medical Ethics Committee of Sana’a University, Yemen was obtained. After instructing to all subjects the study objectives and that their information will be kept confidential and only be used for research purposes, they were asked to agree or disagree to participate in the study using written informed consent forms.
The collected data included demographic characteristics (i.e., gender, age and place of birth) and morphometric (i.e., shapes of MCIs and face) information from the digital photographs of each participant. The data collection process took a period from February to August 2022.
Determination of facial biotype and MCIS shape
The photographs were taken using a digital camera (Canon, EOS 250D, Zoom Lens EF-S 18-55 mm, Japan). For each participant, two photographs were taken (20,21), including an extraoral photograph for determining the face shape and an intraoral photograph for determining the MCIs shape (Figure 3).

Figure 3: Extraoral and intraoral photographs
For photo shoots, the camera mounted on a tripod and placed at a distance of 50 cm from the participant’s face and at a height of 1 m from the floor. All participants were asked to sit on a chair and put their jaws’ bottom on a head positioning device (Figure 4) particularly developed for this study. Each participant was advised to sit on a stool. The head positioning device has two wooden bars running vertically at both sides of the participant’s face.

Figure 4: Head positioning device
After the participant put his/her jaw bottom on the device, these bars were carefully closed until they contacted both sides of the participant’s face (21); therefore, the head of the participant is of a real and natural position (22) for taking the photograph of the face.
In the same position of the participant, a lip retractor was used to visualize and take the photograph of the MCIs.
The photographs were transferred to a computer and analyzed using Adobe Photoshop CS 11 (Adobe Systems Incorporated, USA). On the photograph of the face, two horizontal lines were drawn: one tangential to the upper edge of the eyebrows and the other tangential to the lower margin of the jaw. Then the two lines were joined at the ofrion point (i.e., intersection of the midsagittal plane and the plane tangent to the upper edge of the eyebrows) and the gnathion point (i.e., the lowest and highest point of the chin contour) by drawing a vertical line that matched facial midline in order to determine facial height. Similarly, two tangent vertical lines at the sides of the face were made, being later joined at the level of the most external points of the face using a horizontal line to determine facial width (21) (Figure 5).
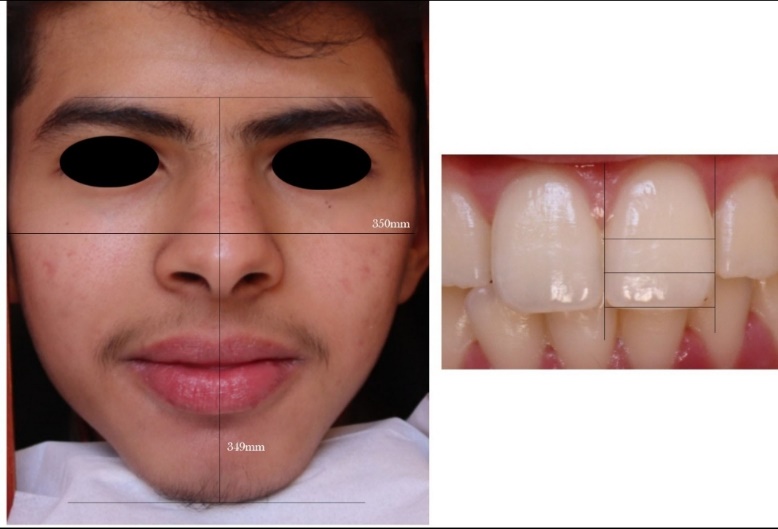
Figure 5. Lines drawn for determining facial index
Then data were set in the formula proposed by Mayoral (23) to determine the facial index (FI) which is the ratio of morphologically maximum facial height (FH) and maximum facial width (FW) and can be calculated according to the formula (24):
FI=FHFW×100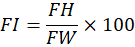
When the value is < 97, the face shape is considered square (brachyfacial), if the value is between 97-104, it is considered ovoid (mesofacial), and if the value is > 104, it is considered triangular (dolichofacial) (21).
On the other hand, the photograph of the teeth is used to determine the shape of the maxillary right central incisor using the method proposed by Williams (25) who suggested that there are three types of teeth: Class I: square tooth (parallel proximal surfaces), Class II: triangular tooth (converging proximal surfaces), Class III: ovoid tooth (rounded proximal surfaces) (26). Therefore, the tooth contour was drawn (Figure 6) for qualitatively evaluating the type of teeth.
Figure 6. Tooth contours drawn for evaluating the type of teeth
Data analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) (version 28.0, SPSS Inc., Chicago, IL, USA). Data were presented using descriptive statistics, including frequency and percentages. Chi-square test was used for determining the morphometric relationships between permanent MCIs and face. P-value < 0.05 was considered statistically significant.
Results
A total of 315 participants with a mean age of 21.78 ± 2.29 were frequently distributed according to gender, face shape (brachyfacial, mesofacial, and dolichofacial), and MCIs form (square, ovoid, and triangular) as shown in Table 1. Results revealed that males were about three fourths of the total sample (234, 74.3%) compared to females (81, 25.7%). Regarding facial shape, nearly half of the participants had a mesofacial shape (156, 49.5%), followed by those with dolichofacial shape (106, 33.7%), then those with brachyfacial shape (53, 16.8%). Regarding MCIs form, almost half of the participants had a triangular form (151, 48.0%), followed by those with ovoid form (100, 31.7%), then those with square form (64, 20.3%).
Table 1. Characteristics of the study sample
|
Characteristic |
N |
% |
|
|
Gender |
Male |
234 |
74.3% |
|
Female |
81 |
25.7% |
|
|
Face shape |
Brachyfacial |
53 |
16.8% |
|
Mesofacial |
156 |
49.5% |
|
|
Dolichofacial |
106 |
33.7% |
|
|
MCIs form |
Square |
64 |
20.3% |
|
Ovoid |
100 |
31.7% |
|
|
Triangular |
151 |
48.0% |
|
|
Total |
315 |
100 |
|
The association of face shapes and MCIs shapes with gender was presented in Table 2. In general, results revealed that there is a significant association between face shapes and gender (p<0.001), as the brachyfacial shape was observed more in males (21.4%) than females (3.7%), whereas the dolichofacial shape was observed more in females (46.9%) than males (29.1%). However, the mesofacial shape was equally observed in both genders (male, 49.6%; female, 49.4%). Moreover, results revealed that there is a significant association between MCIs shapes and gender (p<0.001), as the triangular MCIs shape was observed more in males than females (53.4% vs 32.1%), whereas the ovoid and square MCIs shapes were observed more in females than males (43.2% vs 27.8% and 24.7% vs 18.8%, respectively).
Table 2. Association of face shapes and MCIs shapes with gender
|
Variable |
Male |
Female |
Total |
P |
|
|
Face shape |
Brachyfacial |
50 (21.4%) |
3 (3.7%) |
53 (16.8%) |
0.000* |
|
Mesofacial |
116 (49.6%) |
40 (49.4%) |
156 (49.5%) |
||
|
Dolichofacial |
68 (29.1%) |
38 (46.9%) |
106 (33.7%) |
||
|
Total |
234 (74.3%) |
81 (25.7%) |
315 (100.0%) |
||
|
MCIs shapes |
Square |
44 (18.8%) |
20 (24.7%) |
64 (20.3%) |
0.004* |
|
Ovoid |
65 (27.8%) |
35 (43.2%) |
100 (31.7%) |
||
|
Triangular |
125 (53.4%) |
26 (32.1%) |
151 (48%) |
||
|
Total |
234 (74.3%) |
81 (25.7%) |
315 (100.0%) |
||
* Statistically significant at (p<0.05).
The difference between correlated (i.e., the tooth shape conforms to the face shape) and non-correlated cases (i.e., the tooth shape does not conform to the face shape) is presented in Table 3. In general, results revealed that there is a statistically significant difference (p=0.003) between correlated and non-correlated cases, where correlated cases were significantly less than non-correlated cases (129, 41% vs 186, 59%). Among the 129 correlated cases, the mesofacial/ovoid shape was the predominant (59, 45.7%), followed by the dolichofacial/triangular (56, 43.4%), then the brachyfacial/square (14, 10.9%).
Table 3. Association between correlated and non-corelated face and MCIs shapes
|
Group |
Brachyfacial/ Square |
Dolichofacial/ Triangular |
Total |
P |
|
|
Correlated |
14 (10.9%) |
59 (45.7%) |
56 (43.4%) |
129 (41%) |
0.003* |
|
Non-correlated |
50 (26.9%) |
41 (22.0%) |
95 (51.1%) |
186 (59%) |
|
|
Total |
64 (20.3%) |
100 (31.7%) |
151 (48.0%) |
315 (100.0) |
* Statistically significant at (p<0.05).
The association between the correlated cases in terms of face and MCIs shapes and gender is presented in Table 4. The results revealed that there is no statistically significant association of the correlated cases and gender (p=0.096). In particular, the highest association was observed in participants having mesofacial with ovoid MCIs shape (45.7%), where it was observed more in females than males (58.8% vs 41.1%). It was followed by the association observed in participants having dolichofacial with triangular MCI form (43.4%) then those having brachyfacial with square MCI form (10.9%), where their association was more in males than females (45.3% vs 38.2% and 13.7% vs 2.9%, respectively).
Table 4. Association of the correlated cases with gender
|
Gender |
Brachyfacial/ Square MCIs |
Mesofacial/ Ovoid MCIs |
Dolichofacial/ Triangular MCIs |
Total |
P |
|
Male |
13 (13.7%) |
39 (41.1%) |
43 (45.3%) |
95 (73.6%) |
0.096 |
|
Female |
1 (2.9%) |
20 (58.8%) |
13 (38.2%) |
34 (26.4%) |
|
|
Total |
14 (10.9%) |
59 (45.7%) |
56 (43.4%) |
129 (100.0%) |
The association between the various face and MCIs shapes is presented in Table 5. In general, results revealed that there is no significant association between various face and MCIs shapes (p=0.184). Results in particular revealed the predominance of triangular MCIs shape observed in 48% of the total participants, where its highest frequency was observed with the dolichofacial shape (52.8%), followed by the brachyfacial (47.2%), then the mesofacial (44.9%). The ovoid MCIs shape was observed in 31.7% of the total participants, where its highest frequency was observed with the mesofacial shape (37.8%), followed by the brachyfacial (26.4%), then the dolichofacial (25.5%). However, the least prevalent MCIs shape observed among the total sample was the square (20.3%), where its highest frequency was observed with the brachyfacial shape (26.4%), followed by the dolichofacial (21.7%), then the mesofacial (17.3%).
Table 5. Relationship between various face and MCIs shapes
|
Face shape |
MCI shape |
Total |
P |
||
|
Square |
Ovoid |
Triangular |
|||
|
Brachyfacial |
14 (26.4%) |
14 (26.4%) |
25 (47.2%) |
53 (16.8%) |
0.184 |
|
Mesofacial |
27 (17.3%) |
59 (37.8%) |
70 (44.9%) |
156 (49.5%) |
|
|
Dolichofacial |
23 (21.7%) |
27 (25.5%) |
56 (52.8%) |
106 (33.7%) |
|
|
Total |
64 (20.3%) |
100 (31.7%) |
151 (48.0%) |
315 (100.0%) |
|
Discussion
It is well known that facial esthetics mainly rely on the appearance of MCIs (27). Also, the placement, color, and form of MCIs play a significant role in an attractive smile (28,29). Threfore, this prospective cross-sectional study was conducted to identify face shapes and MCI forms in order to investigate any possible resemblance between them.
The present study found that, of the total sample, males were about three times more than females (74.3% vs 25.7%), which could be attributed to the cultural nature as well as the traditional customs and lifeways of the Yemeni population where the majority of females are veiled and refuse to have their faces photographed.
Regarding the face shapes, the present study found that the mesofacial/ ovoid/ oval was the most frequent face shape, followed by the dolichofacial/ tapered/ triangular, and finally the brachyfacial/ square. These results comply with those of Farias et al. who revealed that the most frequent face shape observed in the Brazilian population was the oval, followed by the triangular and the square (7). They also partially comply with results of Wolfart et al. who found that the most frequent face shape in the Caucasian population was the ovoid followed by the square, and finally the tapered (28). On contrary, these results are not in agreement with those of DeSouza et al. in Brazil, Cabello and Alvarado in Peru, and Mehndiratta et al. in India, in which the most frequent face shape observed was the tapered, followed by the ovoid, then the square (19,21,30). In addition, other studies conducted in Cuba, Chile and Peru found that the most frequent biotype was brachyfacial followed by mesofacial, and finally dolichofacial (31-33).
Regarding the tooth form, the present study found that the triangular was the most frequent MCI form, followed by the ovoid, and finally the square. These results are partially consistent to the studies of Cabello and Alvarado in Peru and Mehndiratta et al. in India who reported that the least frequent MCI form was the square (19,21). On contrary, these results are not in agreement with that of Farias et al. in Brazil, Cabello and Alvarado in Peru, Carrasco et al. in Spain, and Acosta et al. in Colombia who found that the most frequent MCIs form was the ovoid (7,21,34,35). Moreover, they are not consistent to those of Mehndiratta et al. who reported that the most frequent MCI form in the Indian population was the ovoid followed by the tapered, and finally the square (19). Besides, they are inconsistent to those of Wolfart et al. conducted on the Caucasian population and Pedrosa et al. on the Brazilian population, in which they reported that the most frequent MCI form was the ovoid followed by the square, and finally the tapered (28,29).
The present study also revealed that there is a significant association between face shape and gender (p<0.001), with the predominance of brachyfacial shape in males and the dolichofacial shape in females. This result is similar to that of Koralakunte and Budihal in India in which they found a significant association between face shape and gender with the predominance of square shape in males and ovoid in females (36). Moreover, it is in line with that of Wolfart et al. conducted on the Caucasian population, which showed a significant correlation between face shape and gender with the predominance of square-shaped faces in males and tapered faces in females (28). On contrary, this result contradicts those of Modi et al. in India and Farias et al. and Furtado et al. in Brazil which reported no significant association between face shape and gender (7,37,38).
In addition, the present study also observed a significant association between MCI form and gender (p<0.05), with the predominance of triangular MCI in males and the ovoid MCI in females. This result partially proves the dentogenic theory of Frush and Fisher which claims that the female tooth form is more often ovoid and the male tooth form is more often square shaped (39). Moreover, this result is partially in line with that of Farias et al. in Brazil which reported a significant correlation between MCI form and gender with the predominance of oval form in both genders (7). On contrary, this result contradicts those of Modi et al., Koralakunte et al., Wolfart et al., Bell, and Mavroskoufis and Ritchie which showed no significant correlation between MCI form and gender (28,37,40-42).
Furthermore, the present study showed that there is a statistically significant difference between correlated and non-correlated cases in terms of face and MCI shapes (p<0.05), where correlated cases were significantly less than non-correlated cases (129, 41% vs 186, 59%). Among the correlated cases, the highest correlation was observed in participants with mesofacial/ovoid shapes, followed by those with dolichofacial/ triangular shapes, then those with brachyfacial/square shapes. This finding is similar to those of Mehndiratta et al. in India and DeSouza et al. in Brazil who found that the highest correlation was observed in participants with ovoid shapes, followed by those with tapered shapes, then those with square shapes (19,30).
Moreover, the present study showed that there is no significant association between correlated face and MCI shapes according to gender (p>0.05). This finding is similar to that of Mehndiratta et al. who revealed that the correlation between facial shape and tooth form between men and women was non-significant (p=0.4358) (19).
The present study showed that individual examinations revealed no significant association between the various face and MCI shapes (p=0.184) with a greater prevalence of the triangular/dolichofacial shape. Accordingly, this result disproves the typal form theory of Williams (25). A similar result was observed in the studies of Hussein et al. in Sudan, Vinothini, Koralakunte and Budihal, and Shah et al. in India, Farias et al. and Silva et al. in Brazil, and Wolfart et al. conducted on the Caucasian population, which found no significant association between various face and tooth shapes (7,28,36,43-46). In contrast, studies of Boujoual et al. in North Africa, Shaweesh et al. in Jordan, Abdulhadi in the Malays and Chinese, Pedrosa et al. in Brazil, Lindemann et al. in Germany, Berksun et al. in Türkiye, and Modi et al. in India showed a significant relationship between various face and MCIs shapes (29,37,47-51). According to Shaweesh et al., the use of different analytical approaches in those studies, including qualitative ones, may partly explain such disagreement (48).
Also, the present study showed that most participants, irrespective of the face shapes, had a higher correlation with triangular tooth form in comparison to the other forms. Thus, the triangular tooth form has better chances of matching various face shapes among the Yemeni population. This result is not similar to those of Mehndiratta et al. in India and Brunetto et al. in Brazil, in which most of the participants, irrespective of the face shapes, had a higher correlation with ovoid tooth form in comparison to the other forms (19,52).
These variations in the face shape and tooth form reported in the results of different studies could be attributed to the differences in the various populations assessed as well as their respective ethnicities (19,21).
The most important finding in this study would not be the MCIs form itself, but its overall harmony with the face shape. Therefore, understanding the visual perception’s limitations should prompt us to develop more reliable and validated criteria for the classification of the MCI shape so as to reduce the risk of error caused by the subjective misinterpretation. Besides, we must take into account the elements that can harmonize the shape of the tooth with periodontal, perioral structures and the face shape as a whole (47).
The sum of all these elements makes the classification of the facial forms and the central incisor more prone to failures (7). Therefore, this study showed no significant morphometric relationship between the face and MCIs, serving as dissent for the "Williams' Law of Harmony". Accordingly, further research studies are required to analyze and compare other morphological structures in order to improve the aesthetics and quality of life of patients with dental prosthetic restorations (47,53).
Conclusion
The study concluded that there are no significant morphometric relationships between face and MCIs among the studied Yemeni sample because nearly three‑fifths of the study sample showed no correlation between MCIs and face shapes. Since results do not confirm “Williams' law of harmony”, the study recommends dentists in Yemen to consider their clinical experience and critical sense for achieving good esthetic results when choosing the most suitable anterior tooth. Patients’ opinions and desires should also be taken into account by dentists to ensure optimal and satisfactory esthetic outcomes.
Abbreviations
FH Facial Height
FI Facial Index
FW Facial Width
MCIs Maxillary Central Incisors
SPSS Statistical Package for Social Sciences














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org