Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Mohamed Gwila*, Mostafa Ebshina
Department of Orthopaedics and Traumatology Zliten Teaching Hospital Zliten-Libya
*Corresponding author: Mohamed Gwila, Department of Orthopaedics and Traumatology Zliten Teaching Hospital Zliten-Libya
Received: December 05, 2021
Accepted: December 13, 2021
Published: January 03, 2021
Citation: Mohamed Gwila, Mostafa Ebshina “The Surgical Outcome of Carpal Tunnel Release at Zliten Teaching Hospital: A 3years review (2016- 2018).” Clinical Case Reports and Clinical Study, 5(5); DOI: http;//doi.org/12.2021/1.119.
Copyright: © 2021 Mohamed Gwila. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A carpal tunnel syndrome (CTS) is a relatively common condition in Libya.
A retrospective study carried out in the department of Orthopedics and traumatology Zletin Teaching Hospital to examine the clinical outcome for the surgical treatment of carpal tunnel syndrome in our center from Jan 2016 to Dec 2018.
A 256 patients participated in the study (127 were bilateral CTS, 92 patient were Right sided CTS and 37 patient were Left sided CTS), females (80%) and males (20%) .All patients underwent open release of transverse carpal ligament.
Post-operative follow up were for a mean of 2 years.
A four patients developed wound dehiscence post operatively were unsatisfied with surgical release (0.8 %).
The study showed statistically significant reduction in pain, paranesthesia, night numbness and discomfort post operatively.
Conclusion
Open release of transverse carpal ligament (CTR) showed a statistical good clinical.
Literature Review:
To achieve a successful outcome, treatment must be individualized on the basis of a comprehensive analysis of the severity of symptom of limb, psychosocial status of thepatient, and ability of surgeon to execute a well outlined treatment plan with precision and safety.
Many surgical procedures have been described in management of carpal tunnel syndrome, including endoscopic and open carpal tunnel release. Techniques were further subdivided into traditional open, limited open, single-portal endoscopic, and two- portal endoscopic.
Carpal tunnel surgery, in general, gives satisfactory results regardless of technique. Less postoperative pain and faster recovery has been reported following endoscopic release (ECTR) when compared with an open technique. Has been reported by Agee JM et al (1992)1, Brown RA et al (1993)2 and. Palmer DH et al (1993)3.However, complications have been reported following endoscopic release byMurphy RX Jr et al (1994)4 and Seiler JG et al (1996)5. In an attempt to minimize the trauma of open carpal tunnel release, Lee .and Strickland et al (1998)6 described usingspecially designed instruments and a smaller palmar incision of 1.5 cm in length, and they obtained similar results as after ECTR, and with few complications.
A systematic review of the literature was performed to compare complications of endoscopic and open carpal tunnel release. This study also compared incidence of complications in each group based on chronological periods of data collection. The study found that endoscopic release has a higher incidence of transient nerve injury. There was also an increased incidence of superficial palmar arch injuries in the endoscopic group in the 1960-1990 time period as compared with the 1991-2000 and 2001-2012 periods. No difference was found in scar complications between
rate of nerve injuries has not changed since the introduction of endoscopic release. This higher incidence of transient nerve injury and lack of increased skin complications should be weighed when deciding between open and endoscopic techniques.
. Eason et al(1985)7divided the complications into three groups: incomplete TCL resection, recurrent median nerve compression due to tenosynovitis or fibrotic proliferation, and iatrogenic injury to the median nerve or its branches.
Mackinnon et al (1991)8distinguished three symptomatic groups based on indications for secondary carpal tunnel surgery: persistent symptoms, recurrent symptoms, or new symptoms.
Upton ARM et al (1973)9. The A high incidence of complication after carpal tunnel release failures due to diagnostic error or an incomplete diagnosis, as in the double crush in nerve entrapment syndromes
The author’s classification system follows that of Mackinnon et al(1991)8 in regards to the three principle groups: persistent symptoms, recurrent symptoms, and new symptoms. This personal classification system includes new and more updated information, specifically regarding the third group of complications. The author has not included in his classification the failures due to diagnostic error or an incomplete diagnosis, as in the double crush in nerve entrapment syndromes.
Classification of CTS surgery complications:
1. Symptoms persistence 1.1 Incomplete or complete lack of median nerve decompression 1.1.1 Incomplete sectioning of the distal part of the TCL 1.1.2 Incomplete sectioning of the distal part of the antebrachial fascia 1.1.3 Complete lack of TCL sectioning 2 Symptoms recurrence 2.1 Perinervous fibrotic scar proliferation 2.2 Hypertrophic tenosynovitis of the flexor tendons 3 Onset of new symptoms 3.1 Cutaneous scar pathology 3.2 Painful symptoms of nerve origin correlated to the cutaneous scar
3.2.1 Neuroma from the sectioning of the palmar cutaneous branch of the median nerve or of a sensitive branch of the radial nerve 3.2.2 Mini-neuromas from the sectioning of palmar cutaneous terminal endings of the median and/or ulnar nerve
3.2.3 Cutaneous scar adhesions to the median nerve 3.3 Painful symptoms that are not correlated to the cutaneous scar 3.3.1 Thennar and hypothennar pain (pillar pain) 3.3.2 Piso-triquetral pain 3.4 Nerve complications that are not correlated to the cutaneous scar 3.4.1 Total or partial injuries of the median or ulnar nerve and their branches 3.5 Vascular complications 3.5.1 Hematomas from nonsevere vascular injuries 3.5.2 Severe vascular injuries 3.6 Tendon complications 3.6.1 Adhesions between flexor tendons 3.6.2 Subcutaneous anterior subluxation of the flexor tendons 3.6.3 Non-pre-existing trigger finger 3.6.4 Ulnar subluxation of flexor tendons outside the carpal tunnel
3.65 Injuries of the flexor tendons 3.7 Reduction of hand grip strength 3.8 Infection 3.9 Reflex sympathetic dystrophy (algodystrophy) 3.10 Causalgia One must point out the importance of a correct CTS diagnosis, which is the primary condition for surgical success. Possible surgical complications.
Finally, the prevention of the surgical complications is cited. Analysis of the Complications Symptom Persistence Postoperative CTS symptoms persistence is generally correlated to an incomplete or complete lack of median nerve decompression.
The author, in accordance with Hunt et al(1994)10and also with Strickland et al(1996)11, believes that it is possible to hypothesize that sometimes the persistence of specific neurological symptoms can depend on a partial irreversible damage of the median nerve caused by some nerve fiber bundles becoming ischemic and fibrotic. Incomplete or Complete Lack of Median Nerve Decompression The most common unsuccessful outcome of CTS surgery is due to the persistence of preoperative symptoms .This surgical failure generally is caused by an incomplete or complete lack of median nerve compression due to an incomplete sectioning of the TCL distal tract, or rarely, the distal part of the ante brachial fascia.
Justification of study:
Surgical release of carpal tunnel ligament is recommended for a carpal tunnel syndrome that is increasing in severity and disabling the patient.
Absolute indication for surgery is thennar muscle atrophy andweakness.

Figure 1: Showing clinical photographs of 63 year old female with bilateral thennar muscle atrophy.
General objective:
To examine clinical outcome for surgical treatment of carpal tunnelsyndrome in Zletin teaching hospital from JAN 2016- DEC 20018.
Specific objectives:
To determine the associated factors related to carpal tunnel syndrome
To identify thepost-operative complication.
To assess the relationship between the BMI and clinical outcome.
Hypothesis
There is no correlation between severity of Nerve conduction study (NCS) andclinical outcomeafter operation (post operative).
Select all cases of CTS , who undergone surgical intervention in Zletin teaching hospital from JAN 2016- DEC 2018.
All patient with carpal tunnel syndrome, those underwent surgical intervention in Zletin teaching hospital and Naima hospital as day case surgery from JAN2016- DEC 2018 (256patients)
Other causes of upper limb paraesthesia or pain regardless CTS.
Anatomy:
Carpal tunnel defined byscaphoid tubercle and trapezium radially
-hook of hamate and pisiform ulnarly ,transverse carpal ligament palmarly (roof) proximal carpal row dorsally (floor).
Carpal tunnel consists of nine flexor tendons, one nerve (median nerve) and FPL is the most radial structure.
Opalmar cutaneous branch of median nerve:
Lies between PL and FCR at level of the wrist flexion crease O recurrent motor branch of median nerve:
- 50% are extraligamentous with recurrent innervation
-30% are subligamentous with recurrent innervation
-20% are transligamentous with recurrent innervation
-cut transverse ligament far ulnar to avoid cutting if nerve is transligamentous.
· Carpal tunnel is narrowest at the level of the hook of thehamate.
Pathophysiology:
-mechanism:
Precipitated byexposure to repetitive motions and vibrationscertain athletic activities –cycling, tennis, throwing.
Compression may be due to
-repetitive motions in a patient with normal anatomy
-space occupying lesions (e.g., gout)
o diabetes mellitus
o hypothyroidism
o rheumatoid arthritis
o pregnancy
o amyloidosis
The clinical pattern is well known, and two papers by the Quality Subcommittee of the American Academy of Neurology (AAN) defined the guidelines for clinical (1993)21. and neurophysiologic diagnosis Jablecki CK et al(2002)22.Two papers by the Quality Standards Subcommittee of the American Academy of NeurologyColombini D et al(2003)23.and American Association of Electro diagnostic Medicine, American Academy of Neurology and American Academy of Physical Medicine and Rehabilitation defined the guidelines for clinical and neurophysiologic diagnosis of CTS Netter et al (2007)24. Case history must focus on symptom onset (in the early stage, mainly nocturnal paraesthesia), provocative factors (positions, repeated movements), working activity (instrument use, vibrating tools), pain localization and irradiation (in the cutaneous median nerve region with ascending, sometimes up to the shoulder, or descending irradiation),manoeuvres which alleviate symptoms (hand shaking, position changes), presence of predisposing (prognostic no!) factors (diabetes, adiposity, chronic polyarthritis, myxoedema, acromegaly, pregnancy), sports activity (baseball, body-building).
Symptoms: numbness and tingling in radial 3-1/2 digits, clumsiness, pain and paraesthesia that awaken patient at night, self-administered hand diagramthe most specific test (76%) for carpal tunnel syndrome.
The list of findings and maneuvers used in the diagnosis of CTS is long; however, a recent literature review has focused its attention on a symptom diagram, and on two signs that are most of help in predicting a positive electro diagnosis of CTS (diagnostic test of reference)D’Arcy CA et al (2000)25.
The Katz hand diagram, Katz JN et al (1990) 26 is a self- administered diagram that allows the patient to localize symptoms and todescribe them as numbness, pain, tingling and hypoesthesia.
-inspection may show thennar atrophy
- carpal tunnel compression test (Durkan's test)is the most sensitive test to diagnose carpal tunnels syndrome performed by pressing thumbs over the carpal tunnel and holding pressure for 30seconds.onset of pain or paraesthesia in the median nerve distribution within 30 seconds isa positive result.
-Phalentest:wrist flexed with elbow extended for ~60 sec produces symptoms. Less sensitive than Durkin compression test.
-Tinel's test
Provocative tests performed by tapping the median nerve over the volar carpal tunnel.
Most sensitive sensory test for detecting early carpal tunnel syndromemeasures a single nerve fiber innervating a receptor or group of receptors.
static and moving two-point discriminationmeasures multiple overlapping of different sensory units and complex corticalIntegration. the test is a good measure for assessing functional nerve regeneration after nerve repair.
o numbness and tingling in the median nerve distribution
o nocturnal numbness
o weakness and/or atrophy of the thinner musculature
o positive Tinel sign
o positive Phalen test
o loss of two point discrimination.
Instrumental diagnosis and its evaluation: Neurophysiological diagnosis Nerve conduction studies and electromyography may confirm, but not rule out, the diagnosis of CTS. The aims ofthis evaluation are the following: (1) to confirm a focaldamage to the median nerve inside the carpal tunnel; (2) toquantify the neurophysiological severity by using a scale;(3) to define the nerve pathophysiology: conduction block,demyelination and axonal degeneration. In a recent review,the American Association of Electrodiagnostic Medicine,the American Academy of Neurology and the AmericanAcademy of Physical Medicine and Rehabilitation definedthe Practice Parameters for electro diagnostic studies in CTS Netter (2007)24 .
- demyelination leads to :1 .NCV :increase latencies (slowing) of NCVdistal sensory latency of > 3.2 ms ,motor latencies > 4.3ms decrease conduction velocities less specific than latencies ,velocity of < 52 m/s is abnormal 2.EMG test the electrical activity individual muscle fibers and motor units detailinsertional and spontaneous activity,increased insertional activity ,sharp waves, fibrillations , fasciculation's, complex repetitive discharges.
Histology: nerve histology characterized byedema, fibrosis, and vascular sclerosis are most common findings,scattered lymphocytesamyloid deposits shown with special stains in some cases.
Classification: CTS may be classified on the basis of symptoms and signs into three stages:
First stage:
Patients have frequent awakenings during the night with a sensation of swollen, numb hand; furthermore, they report of severe pain that irradiates from the wrist to the shoulder, and an annoying tingling in their hand and fingers (brachialgiaparaesthetica nocturne). Hand shaking brings relief. At morning, a sensation of hand stiffness usually persists.
Second stage:
Presence of symptoms also during the day, mostly when the patient remains in the same position for a long time, or performs repeated movements with hand and wrist. When motor deficit appears, the patient reports that objects often fall from his/her hands.
Third stage:
Final stage, hypo-/atrophy of the thennareminence. In this phase, sensory symptoms may diminish. INAIL RAPPORTO et al(2005)27.
Differential diagnosis:
CTS must be differentiated from:
Definitions:
Carpal tunnel syndrome (CTS) is a relatively common condition caused bycompression of the median nerve within the carpal tunnel in the wrist. Thiscan arise for a variety of reasons, including fluid retention, particularly inpregnancy. This gives rise to pain, numbness or tingling in the thumb, indexand middle fingers. In severe cases it may cause nerve damage andweakness/wasting of the muscles of the hand, especially the thumb (thennar wasting). Patients often report their symptoms are worse at night and maydisturb sleep.
Symptoms do not necessarily progressively worsen and, for some, willresolve. In these cases carpal tunnel syndrome will disappear without treatment or with simple self-care. Non- surgical treatments, such as steroid injections or wrist splints are used to treat mild to moderate symptoms.
Surgical release (decompression) of the carpal tunnel may be carried out Ifnon-surgical approaches fail to relieve symptoms.
the treatment of choice to predictably relieve symptoms, and the most common and popular procedure performed in current orthopedic practice is the decompression of the median nerve by open release of the transverse carpal ligament When surgery is indicated,it is important to consider that significant complications may occur.
The clinical symptoms that may ensue following these complications may be more severe and distressing than the patient’s original complaints.
The purpose of this study was to present a number of complications following carpal tunnel surgery and to discuss how they may have occurred and how they may be prevented.
Material and methods
This is a retrospective study consists of reviewing patientsrecords.
Measurements of Nerve conduction study (NCS) and clinical presentation preoperative and post-operative and during follow up were used as outcome parameters for evaluation of open carpal tunnel release.
The study included 256patients, who were diagnosed as carpal tunnel syndrome by clinical and NCS assessment.
Open carpal tunnel releases weredone according the severity of the median nerve neuropathy at the department of orthopedics and traumatology, Zletin teaching hospital. 3yrs review JAN 2016 – DEC 2018.
The operations were done by orthopeadicsurgeonsinthe hospital.
All patients had regular follow up.
Statistical analysis:
Data was entered and analyzed using the statistical package for the social science (spss) version23.0.
All continuous variables were expressed as a mean and a standard deviation for normal distribution data. However if the data was not normally distributed ,median and interquartile ranges were used as well as non-parametric test- Mann Whitney test and Wilcoxon signed Ranks test in addition to repeated measurement analysis which was used to determine the difference in measurements in different time points. Statistical significance was set at p value of less than 0.05 (p<0.05).
ETHICS AND FUNDING:
Every patient knew about study and nothing harmful for them and the permission had been taken from patients verbally and there is no intervention neither during the study nor after and it is approved by ethical comity.
A total of 256 patients were included in this study, 127 patientswere bilateral CTS (49.6%), 92 patientshad Right CTS(35.9%) and 37 patientshad LeftCTS (14.4 %). The mean post operative follow up were 2 years.Age group were 22years to 90 years (The mean age at presentation was 47 years)<figure:1>,204 patients (80%) were females and 52 patients (20%) were males. the mean body mass index (BMI) were28.085m2/kg which was categorized as overweightrange according to the WHO classification<figure :2>.50.8 %of patientswere severing compression of median nerve reported in Nerve conduction study <figure:3>.
Figure: 1

Figure: 2
|
|
Figure: 3
|
|
Carpal tunnel syndrome patients presented with Dull aching discomfort in the hand, forearm and withhand paraesthesia
,numbness werepresent in (95%) of patients, Clumsiness were present in 66 patients( 25%) and thennar muscle atrophy were seen in 13 patients( 5 %).
There were statistically significant reduction in Dull aching discomfort in the hand ,forearm, paraesthesia and numbness post operatively compared to pre operatively(p<0.001).However, there were no statistically significant improvement in Clumsiness and thennar muscle atrophy during last follow up compared to pre operative assessment.
The result of this study show no statistically significant relation between post operative complication and BMI with (p=0.194), as well as there was statistically significant correlation between Nerve conduction study (NCS) severity and recurrentsymptoms afteroperation (p=0.011).
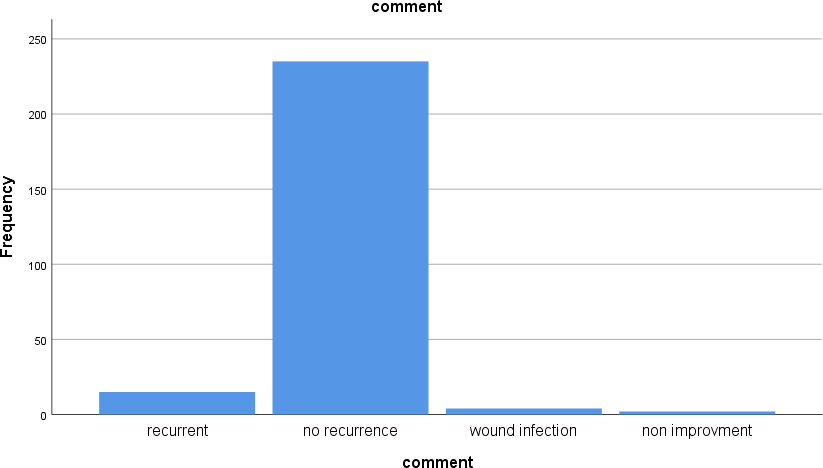
There were three complications: 4 patients had wound dehiscence (superficial infection) which was treated with dressings and antibiotics,15 patients had recurrence symptoms of CTS (3 of were treated with revision Carpal tunnel release)and 2 patients were unsatisfied after operation(persistent symptoms).<Figure: 4>
FIGURE: 4
Carpal tunnel release is an established treatment for Carpal tunnel syndrome. A variety of techniques have been Advocated, includingendoscopic and open carpal tunnel release. Techniques were further subdivided into traditional open, limited open, single-portal endoscopic, and two-portal endoscopic.
In our study, we reviewed 384 hands in 256 patients with CTS.The mean age at presentation were 47 years. Females(80%)and 20% males. The mean BMI 28 m2/kg and compared with other studies that shown similar finding as result a stronger relationship between Nerve conduction study ( NCS ) severity and recurrent symptom after operation.
127 patients had bilateral CTS and 129 unilateralCTS and this concluded same result by other author.The most cases had sever nerve compression 50%confirmed using electro diagnostic (EDX) techniques and others moderate nerve compression 33%..In this study the surgical technique was performed by open carpal tunnel release under local anesthesia. <Figure: 2 >
|
|
FIGURE 2 (A): Showing clinical photographs of a53 year old female with open technique CTR showing hyperemic median nerve.

Figure 2: (B)Showing clinical photographs of a 61 year old female 1 years post open technique CTR.
There were statistically significant decreases in symptomsof CTS post operative.
Compared to other study byKuschner et al. (1991)12 found the Overall complication rate of this operation to be between1% and 2%. Kulick et al. (1986)13 reported that out of130 hands treated by the open technique, 4.6% laterdeveloped recurrence of symptoms. Nancollas et al.(1995) 14published a retrospective study, including 60patients operated by the open technique, with onlyone patient requiring revision, within a mean follow-uptime of 5.5 years. But in our study we achieved good result and long follow-up mean 2 years.
We found the overall complication rate of this operation to be between8% and 9% .we reported that out of256 patient treated by the open technique( CTR) 5.9 % laterdeveloped recurrence of carpal tunnel symptoms and 0.8 % no improvement after operation.
In 2 patients of these 17 patients, the pre-operative symptoms were entirely unchanged. In 15 patients, the symptoms recurred shortly after the initial surgery.
In a study of 2053 open carpal tunneldecompressions, Langloh et al (1972)15reportedonly 34 patients, accounting for 1.6% of their cases, whounderwent re-exploration for recurrence.
However, in contrast to these figures, other authors have reportedrecurrent symptoms of CTS in up to 19% of patientsfollowing CTR, with up to 12% requiring re- exploration.Concanoon et al (1997)16; Huang et al (2004)17;Langloh et al (1972)15; MacDonald et al (1978)18;Repaci et al (1999)19.
Gerritsen et al (2002)20 reported adverse effects during the follow-up period.Adverse effects include painful or hypertrophic scar; woundhematomas and infection; stiffness, swelling or discomfort of thewrist and reflex sympathetic dystrophy. Fifty- eight out of 87 participants (56.6%) allocated to surgery.
Statistics:
|
Stage |
|||||
|
Freque ncy |
Percen t |
Valid Percent |
Cumulati ve Percent |
||
|
Vali d |
|
41 |
16.0 |
16.0 |
16.0 |
|
Severe |
130 |
50.8 |
50.8 |
66.8 |
|
|
Moder ate |
85 |
33.2 |
33.2 |
100.0 |
|
|
Total |
256 |
100.0 |
100.0 |
|
|
|
Age |
||
|
N |
Valid |
256 |
|
|
Missi ng |
0 |
|
Mean |
47.24 |
|
|
Median |
46.00 |
|
|
Std. Deviation |
12.125 |
|
|
BMI |
||
|
N |
Valid |
188 |
|
|
Missi ng |
68 |
|
Mean |
28.085 |
|
|
Median |
28.200 |
|
|
Std. Deviation |
2.5096 |
|
Comment
|
Freque ncy |
Percen t |
Valid Percent |
Cumulati ve Percent |
||
|
Vali d |
Recurrent |
15 |
5.9 |
5.9 |
5.9 |
|
no recurrence |
235 |
91.8 |
91.8 |
97.7 |
|
|
wound infection |
4 |
1.6 |
1.6 |
99.2 |
|
|
non improveme nt |
2 |
.8 |
.8 |
100.0 |
|
|
Total |
256 |
100.0 |
100.0 |
|
|
Correlations
|
comme nt |
stage |
|||
|
Spearman's rho |
Comm ent |
Correlation Coefficient |
1.000 |
.172* |
|
Sig. (2-tailed) |
. |
.011 |
||
|
N |
256 |
215 |
||
|
stage |
Correlation Coefficient |
.172* |
1.000 |
|
|
Sig. (2-tailed) |
.011 |
. |
||
|
N |
215 |
215 |
||
*. Correlation is significant at the 0.05 level (2-tailed).
Correlations
|
Bmi |
comme nt |
|||
|
Spearman's rho |
Bmi |
Correlation Coefficient |
1.000 |
-.095 |
|
Sig. (2-tailed) |
. |
.194 |
||
|
N |
188 |
188 |
||
|
Comm ent |
Correlation Coefficient |
-.095 |
1.000 |
|
|
Sig. (2-tailed) |
.194 |
. |
||
|
N |
188 |
256 |
||
CONCLUSION:
The goal of treatment of carpal tunnel syndrome is to attain decrease in symptoms of CTS post-operative. Although the etiology of CTS may be multifactorial and based on four finding, there is nostatistically significant relationship between the BMI and recurrence of the symptom.
There isstatistically significant correlation between severity Nerve conduction study (NCS) and recurrence clinical symptom of patient.
There is no correlation between the age of patient and recurrence clinical symptom of CTS.
The result showed a good clinical outcome,werecommend open Carpal tunnel release (CTR) in treatment of Carpal tunnel syndrome.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org


