Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Garima Rawat1*, Gaurav Sharma2
1Oral & Maxillofacial Pathology Department of Pathology, Dharamshila Narayana Superspeciality Hospital, New Delhi
2Department of Pathology, Dharamshila Narayana Superspeciality Hospital, New Delhi
*Corresponding author: Garima Rawat, Oral & Maxillofacial Pathology Department of Pathology, Dharamshila Narayana Superspeciality Hospital, New Delhi.
Received: October 25, 2021
Accepted: December 24, 2021
Published: December 27, 2021
Citation: Garima Rawat, Gaurav Sharma “Pilar Csyt Of Scalp.” Clinical Case Reports and Clinical Study, 5(5); DOI: http;//doi.org/09.2021/1.109.
Copyright: © 2021 Garima Rawat. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
,
Pilar Cyst of Scalp
Trichilemmal or pilar cysts are common keratin filled cysts arising from the outer hair root sheath. They comprise 10% of all skin cysts and 90% of them occur on the scalp. Usually sporadic and no malignant transformation is reported. They arise from the epithelium between the sebaceous gland and arrector pili muscle. The pilar cyst rate of growth is very slow; it takes several years to grow to a big size. These cysts may be inherited as an autosomal dominant trait, although patients with familial pilar cysts are often younger and present with multiple lesions at the same time. The patients involved are commonly adult females. These cysts most commonly present as asymptomatic, mobile, firm and well circumscribed nodule.
Microscopically, these cysts are well circumscribed subcutaneous or dermal simple cyst, lined by stratified squamous epithelium with a palisaded outer layer and contains dense laminated eosinophilic keratin Granular layer is absent. Calcification may be present in up to 25% cases. Granulomatous response may be elicited due to rupture of cyst. The histological variants of trichilemmal cyst are1, 2, 3
The case being presented here is a female in the 7th decade of her life who presented with a long standing, well circumscribed, asymptomatic swelling on scalp. Clinical provisional diagnosis of lipoma or sebaceous cyst was made. The patient underwent excision of the lesion followed by uneventful healing. The microscopic picture was consistent with that of a Trichilemmal cyst.
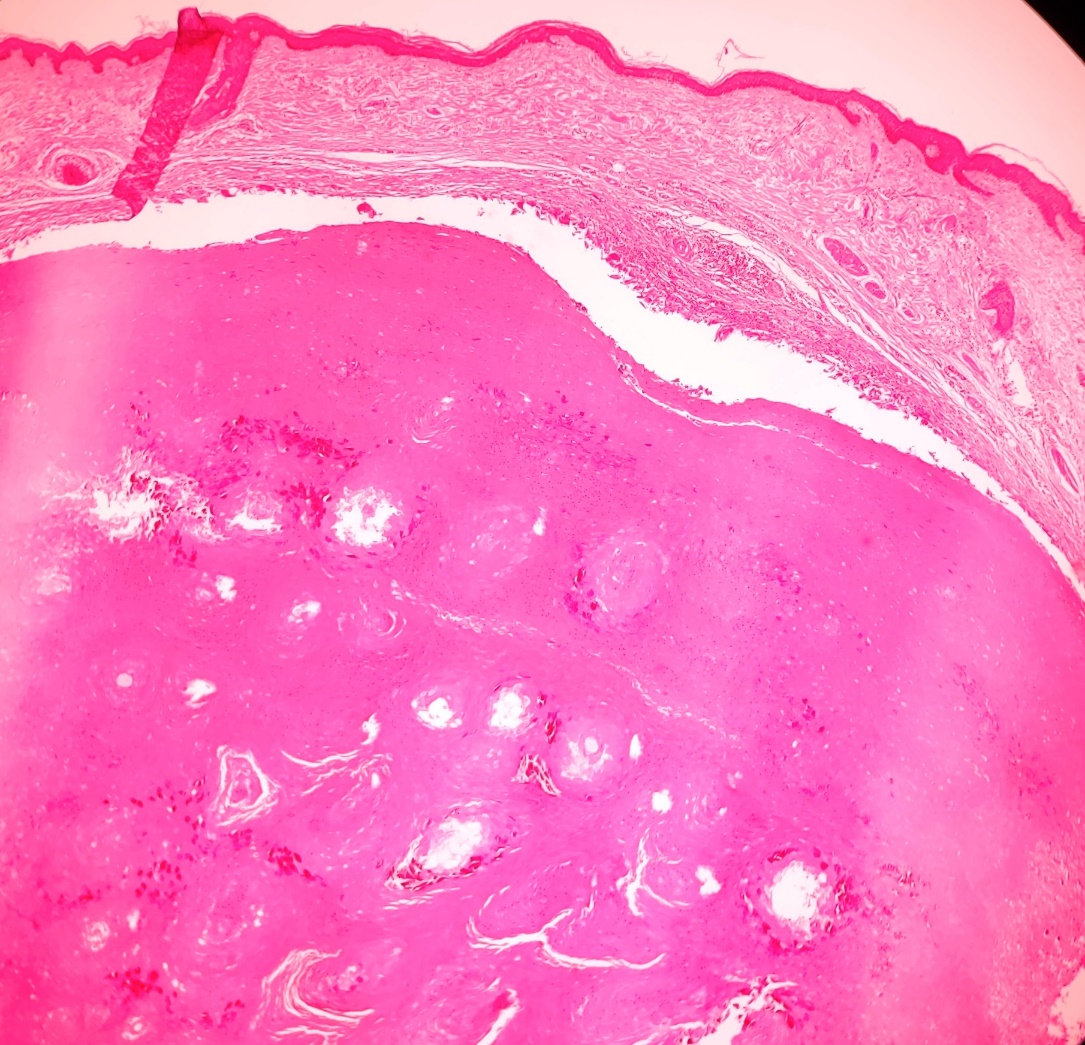
Figure 1 – Photomicrograph showing cyst lined by stratified squamous epithelium with a palisaded outer layer. (HE 40x)
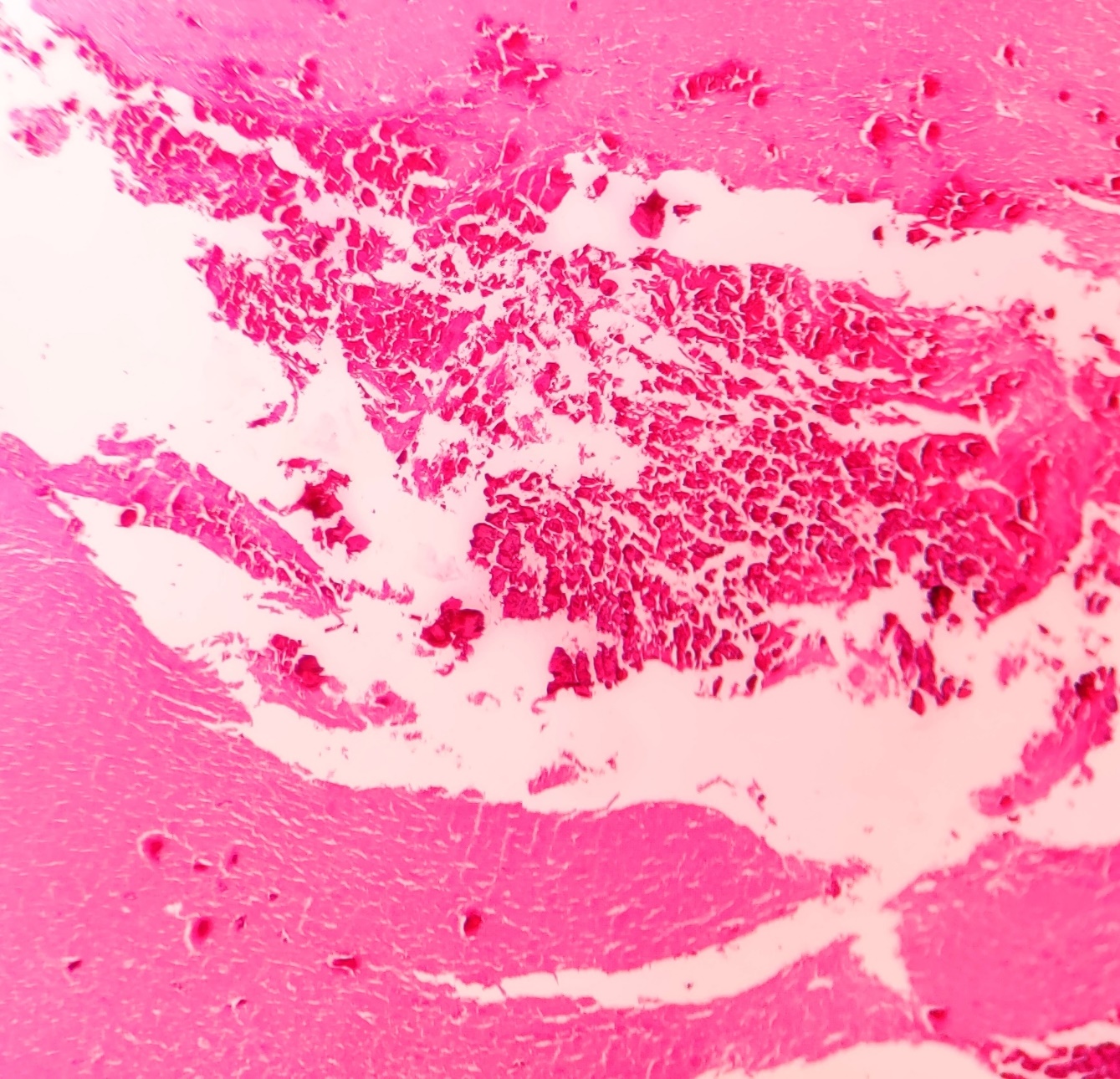
Figure 2- Photomicrograph showing dense laminated eosinophilic keratin and calcifications. (HE 100x)
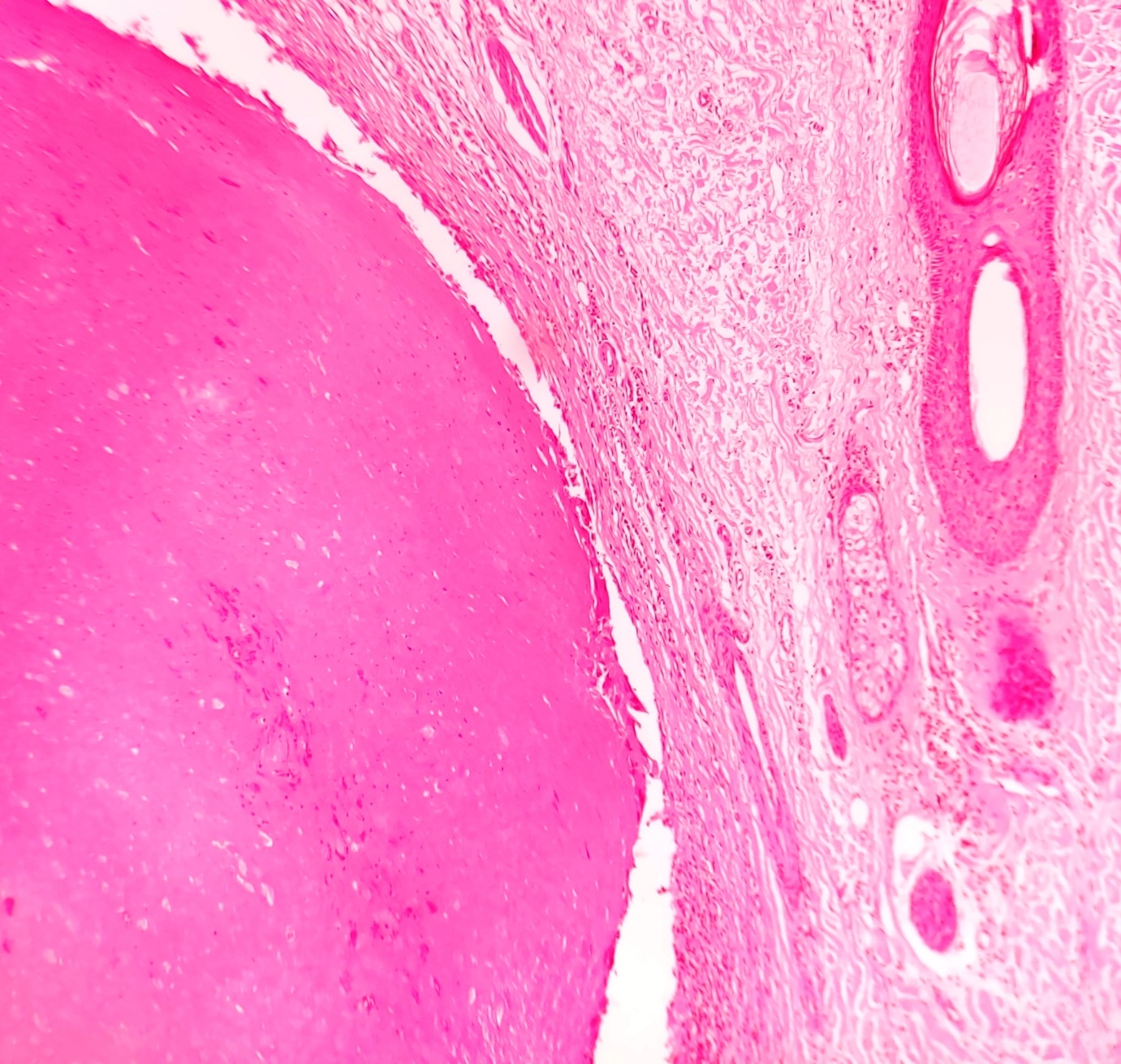
Figure 3- Photomicrograph showing with absence of granular layer. (HE 100x)














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org