Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Fumiaki Takase*, Makoto Mitani, Isao Fujibayashi, Takahiro Furukawa, Takeo Tokura, Takuma Ozaki
Department of Orthopedic Surgery, Himeji Sei Maria Hospital 650, Nibuno, Himeji, Hyogo, 670-0801, Japan
*Corresponding author: Fumiaki Takase, Department of Orthopedic Surgery, Himeji Sei Maria Hospital 650, Nibuno, Himeji, Hyogo, 670-0801, Japan.
Received: February 04, 2021
Accepted: February 10, 2021
Published: February 15, 2021
Citation: Fumiaki Takase, Makoto Mitani, Isao Fujibayashi, Takahiro Furukawa, Takeo Tokura, Takuma Ozaki, (2021) Open Extensor Tendon Dislocation Following Bilateral Sagittal Band Injury: A Case Report. J Clinical Case Reports and Clinical Study, 2(2) ; DOI: 10.61148/2766-8614/JCCRCS/016
Copyright: © 2021 Fumiaki Takase, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Extensor tendon dislocation is relatively uncommon except rheumatoid cases. Here we present a case of open extensor tendon dislocation by bilateral sagittal band injury. The results of this case indicate that extensor tendons tend to be dislocated in the ulnar direction when the both side of the sagittal band is injured, even if the damage to the ulnar side is greater.
Introduction
Extensor tendon dislocation secondary to damage to the sagittal band is uncommon in patients without rheumatoid disorders. Traumatic dislocation accounts for 73% of all extensor tendon dislocations [1] and is usually caused by direct injury to the dorsal aspect of an incompletely flexed finger. These dislocations are known as “boxer’s knuckle,” which was first described by Gladden [2]; however, such cases are usually closed injuries. Open injuries are very rare; to date, there has been no report of an open extensor tendon dislocation by bilateral sagittal band injury. Here, we report a rare case of extensor tendon dislocation.
Case Presentation
A 36-year-old man was injured by a rolling machine at work. Although the machine was stopped as soon as his right hand rolled into it, he could not remove his fingers. Therefore, he pulled his finger forcefully out of the machine, lacerating the skin on the dorsum of the hand between the index and the middle finger. He could not fully extend his index finger after the injury. A local clinic examined the patient and diagnosed him with open extensor tendon dislocation of the index finger, and he was referred to our hospital for further management. The skin laceration was sutured at the local clinic, and there was swelling around the metacarpophalangeal (MP) joint of the index finger. He could not fully flex or extend his index finger. The extension lag of the MP joint was 25° (Fig. 1). Radiographs revealed no abnormal findings. Magnetic resonance imaging (MRI) showed a dislocation of the extensor tendons of the index finger (Fig. 2).
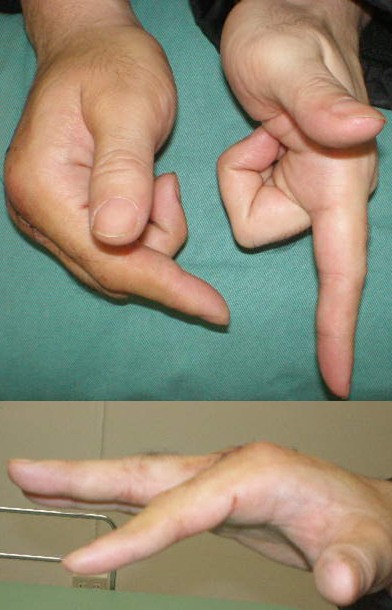
Figure 1: Preoperative physical findings. The patient could not fully extend his index finger. The extension lag of the metacarpophalangeal joint was 25°.
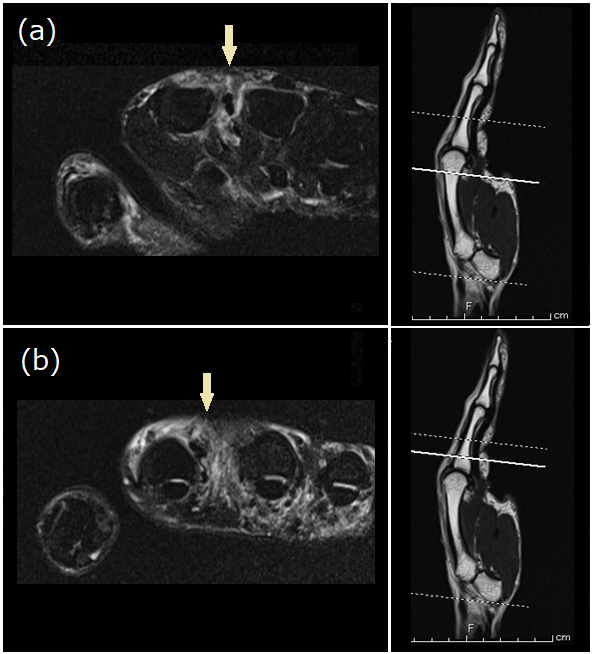
Figure 2: Preoperative magnetic resonance imaging, showing the dislocation of the extensor tendons of the index finger at the metacarpal head (a) and at the proximal phalanx base (b).
We performed a surgical operation because we believed that conservative treatment would not be successful. This operation was performed under local analgesia. Both the extensor digitorum communis (EDC) and the extensor indicis proprius (EIP) were dislocated in the ulnar direction over the MP joint (Fig. 3). The ulnar tissue of the extensor tendons, including the sagittal band, was crushed just below the skin laceration. Although the radial sagittal band was also ruptured at the radial border of the extensor tendon, there was no injury to the surrounding tissue. The tendons could be reduced manually, but they could be easily dislocated. We cut the distal part of the juncturae tendinum between the index and the middle finger because it pulled on the extensor tendons and dislocated the ulnar side, and it was thought to inhibit the reduction of the tendons. Retention of the reduction could not be achieved with only sagittal band repair. Therefore, the radial sagittal band was sutured directly to the EDC and the under tissue of the EDC was sutured to the EIP.(Fig. 4). After the repair, we asked the patient to move his finger, and he achieved full active range of motion of the index finger without dislocation of the extensor tendons.

Figure 3: Before the soft tissue repair. Both the extensor digitorum communis and the extensor indicis proprius were dislocated in the ulnar direction over the metacarpophalangeal joint.

Figure 4: After the soft tissue repair. After the repair of the sagittal band and soft tissue. The dislocation of the tendons was reduced.
Postoperatively, the involved finger was immobilized for three weeks with the MP joint in a slightly flexed position, allowing active motion of the interphalangeal joints. The patient felt no pain and regained almost full motion of the finger, and there was no recurrent dislocation of the tendon six months after the surgery (Fig. 5). MRI showed no dislocation of the extensor tendons of the index finger (Fig. 6). The grip strength of the affected side was 62 kg and that of the healthy side was 50 kg.
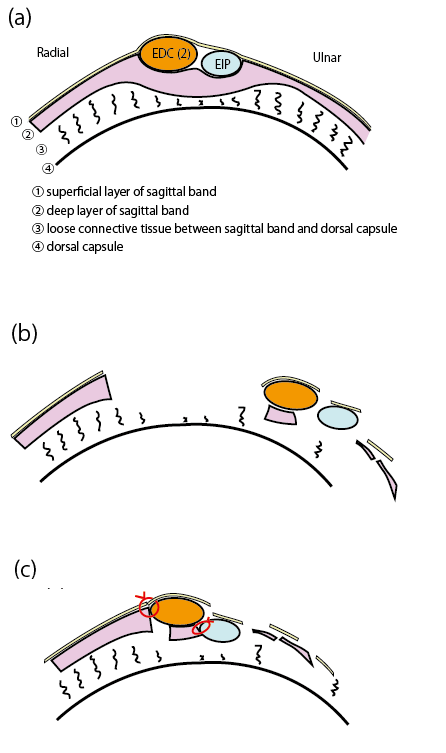
Figure 5: Schemes of extensor tendons at the metacarpophalangeal (MP) joint. (a) Normal anatomy. (b) Dislocation of the extensor tendons as shown in this case report. (c) After surgical repair with soft tissue suture around the tendons.
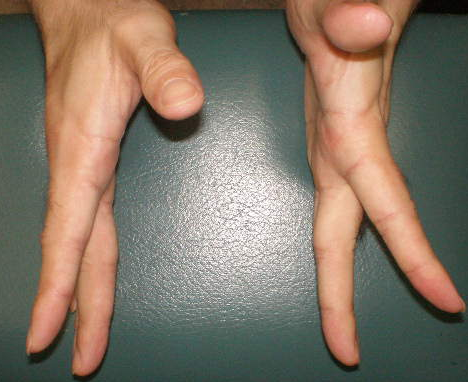
Figure 6: Postoperative physical findings at six months after surgery. The patient regained nearly full motion of the finger, although there was a slight extension lag compared with the healthy side.
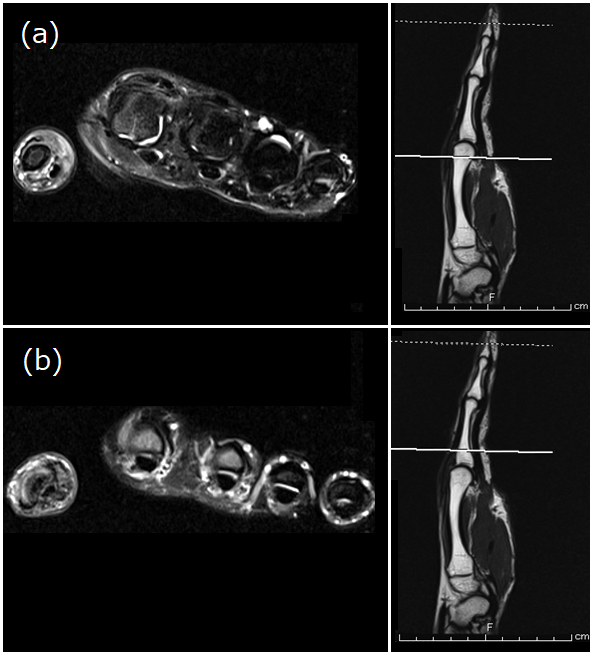
Figure 7: Postoperative magnetic resonance imaging (MRI) at six months after surgery. MRI of the metacarpal head (a) and the proximal phalanx base (b) showed no dislocation of the extensor tendons of the index finger.
Discussion
The flexor and extensor tendons of the hand tend to pull on the ulnar side of the MP joint. Ulnar deviation of the MP joint of the fingers is often observed in patients with rheumatoid disorders due to the relaxation of the soft tissues caused by arthritis. Dislocation of the extensor tendon over the MP joint is rare in patients without rheumatoid disorders. Other factors predisposing individuals to dislocation of the extensor tendons of the fingers can be congenital, idiopathic, traumatic, and atrophic [3]. It is caused by a defect in the primary and secondary stabilizing structures of the EDC. The sagittal band over the MP joint is the primary stabilizing structure [4], and the intertendinous fascia and juncturae tendineae behave as secondary stabilizers of the extensor tendons [5,6]. Traumatic dislocation of the extensor tendon at the MP joint is usually a closed injury. Inoue et al. reported four patients with closed traumatic dislocation of the extensor tendons over the index MP joints. Of the four patients, two had an ulnar dislocation of both the EDC and the EIP tendons and two had a radial dislocation of the EDC tendon and ulnar dislocation of the EIP tendon [7]. Open injuries are very rare and usually involve a laceration over the MP joint, typically on the radial side [8]. Published treatment options for dislocation of the extensor tendon include splinting [9], realignment and direct repair [10,11], and various forms of tendon reconstruction [12]. In this case, the skin laceration occurred on the ulnar side, and the ulnar tissue of the extensor tendons was more damaged than on the radial side. However, both the EDC and the EIP of the index finger were dislocated in the ulnar direction. Although the radial side of the sagittal band was somewhat damaged, it was useful for realignment of the extensor tendons; thus, we performed a direct repair, which achieved a good clinical result.
Conclusion
In this study, we presented, for the first time, a case of open extensor tendon dislocation by bilateral sagittal band injury. Direct repair was useful for the open extensor tendon dislocation due to bilateral sagittal band injury. The results of this case indicate that extensor tendons tend to be dislocated in the ulnar direction when the both side of the sagittal band is injured, even if the damage to the ulnar side is greater.
Conflict interest
None declared.
Author contributions
FT: followed up the patients, and drafted the manuscript. MM, IF, TF, and TT: reviewed the manuscript. TO: revised and approved the manuscript.
Ethical approval
The patient provided consent for publication of this report and the accompanying images.
Acknowledgements
We thank the patient for his participation in this report.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org