Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Afaf.Khouna 1*, Nada.Zizi 1,2, Siham.Dikhaye 1, 2
1 Department of Dermatology, Mohammed VI University Hospital of Oujda, Medical School of Oujda, Mohammed First University of Oujda, Morocco.
2 Department of Epidemiology, Clinical Research and Public Health Laboratory, Medical School of Oujda, Mohammed First University of Oujda, Morocco.
*Corresponding author : Afaf Khouna, Department of Dermatology, Mohammed VI University Hospital of Oujda, Medical School of Oujda, Mohammed First University of Oujda, Morocco.
Received: April 12, 2021
Accepted: May 03, 2021
Published: May 14, 2021
Citation: Khouna A, Zizi N, Dikhaye S “Allergic Contact Dermatitis to Amorolfine in Nail laquer”. Clinical Case Reports and Clinical Study, 3(4); DOI:10.61148/2766-8614/JCCRCS/059
Copyright: © 2021 Afaf Khouna. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Allergic contact dermatitis caused by antifungal drugs is very rare. Amorolfine is a widely prescribed as an antifungal treatment for onychomycosis, especially in nail lacquer. ]. Allergic contact dermatitis by amorolfine is rarely reported in the literature, hence we report a case of contact dermatitis to amorolfine in nail.
Introduction
Allergic contact dermatitis caused by antifungal drugs is very rare. Imidazole derivatives have been described as the most sensitizing agents [1]. Amorolfine is a widely prescribed as an antifungal treatment for onychomycosis, especially in nail lacquer. The side effects of this molecule seems to be rare and may be under-diagnosed as these products are sold without medical prescription [2]. Allergic contact dermatitis by amorolfine is rarely reported in the literature [1].
We report a case of allergic contact dermatitis of the first 2 toes of the left foot secondary to the application of amorolfine in nail lacquer for suspected onychomycosis of the nail of the left big toe, with a positive allergological test.
Case report
A 30-year-old patient, presented a distal onycholysis of the left big toe evolving since 3 months. By self-medication, the patient applied amorolfine nail lacuqer in the nail of the left big toe twice a week. The patient did not report the application of any other product on her toes. One month later she presented a severe pruritus of the first two toes of the left foot associated with edema, erythema and vesicles (figure 1,a).

Figure 1A: Edema, erythema and vesicles of the big and 2nd toes of the left foot.
A semi-open allergological test was performed on the patient's back, with application of the nail lacquer with medical petroleum jelly at the first site (figure 1,b, red star) and medical petroleum jelly alone at the second site (figure 1,b, black star),both covered by an oclusive bandage and left in place for 48 hours.
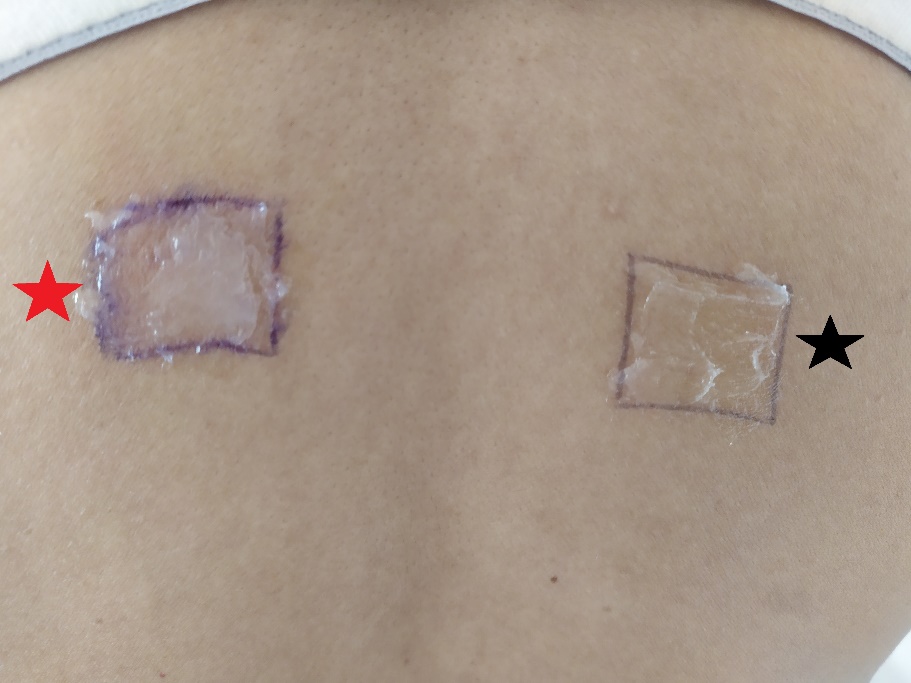
Figure 1B :
When the bandage was removed, a bright red erythema was noted at the site tested with amorolfin mixed with medical petroleum jelly (figure 1,c, red star) and no reaction at the site tested with medical petroleum jelly alone (figure 1,c: black star).

Figure 1C:
Black star : no site reaction tested with medical petroleum jelly
The patient was treated with dermocorticoids with cessation of amorolfine application with good evolution and disappearance of oedema, erythema and pruritus.
Discussion
Onychopathies such as onycholysis or onychodystrophy are often treated without a medical prescription, but rather empirically with topical antifungal treatments. Nail lacquer with amorolfine are the most frequently chosen by patients because of their weekly application.
Amorolfine is generally well tolerated and has a low allergenic potential, with few reported side effects and few reported allergic contact dermatitis. However, amorolfine in nail lacquer may have a higher allergenicity, increasing the risk of allergic contact dermatitis. Therapeutic nail lacquers contain excipients such as butyl acetate, ethyl acetate and ethanol, which evaporate after application of the product, thus increasing the concentration of amorolfine in the nail bed and peronychium [2].
In our patient, the intense pruritus, edema, erythema and vesicles were suggestive of allergic contact dermatitis. Allergy testing confirmed our patient's allergy to amorolfine.
Cases of allergic contact dermatitis with tioconazole contained in nail lacquer were also reported. This type of allergic contact dermatitis may be underestimated, as patients may consider allergic reactions to be irritating or infectious and does not report the use of topical treatment to their physician [3].
Conclusion
Antifungal nail lacquers solutions are widely prescribed for the treatment of onychomycosis with a rare cases of allergic contact dermatitis whicg would likely be underestimated due to their self-medication use.
Conflict of interest : none














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org