Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Giampietro Bertasi1*, Mariana Peroni2
1University of Padua, Italy
2Ospedale Santa Maria del Carmine, Rovereto, Italy
*Corresponding author: Giampietro Bertasi, University of Padua, Italy
Received: April 27, 2021
Accepted: May 03, 2021
Published: May 06, 2021
Citation: Giampietro Bertasi, Mariana Peroni “Acetabular Revision using ReadiGraft® BLX Putty and Cortical/Cancellous Bone Chips”. Clinical Case Reports and Clinical Study, 3(4); DOI: 10.61148/2766-8614/JCCRCS/054
Copyright: © 2021 Giampietro Bertasi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
,
Dependent on the cause, pain or functional failure in the hip may be resolved by acetabular revision.1-2 Previously placed implants may have become loosened due to lack of bone ingrowth in uncemented hips or lack of cement interdigitation.3-5 Implant-wear can lead to debris which subsequently can incites an osteoclastic cascade resulting in osteolysis and possible loosening of the components.6 Patients may also be predisposed to hip instability due to cognitive deficits,7 neuropathic joints,8 and hyperflexibility9 which are often symptoms of disorders such as Charcot arthropathy or Ehlers-Danlos syndrome. Finally, infections in the hip joints caused by nearby infections or a compromised immune system can also compromise the integrity of the joint resulting in the need for acetabular revision.10
With these factors in mind the goal of reconstruction are as follows:11-13
Demineralized bone matrices (DBM) are one option for the treatment of large acetabular defects to restore bone and enhance fixation of the socket. Bone void fillers, such as allograft bone chips, can be used as a graft extender, eliminate donor-site morbidity, and overcome restricted availability and donor-site comorbidity associated with autografts.14-15 One such DBM, ReadiGraft® BLX Putty*, may be used in acetabular revisions. ReadiGraft BLX Putty is a demineralized bone matrix (DBM) used in orthopedic and spine procedures. This graft is biocompatible, osteoconductive, and osteoinductive. ReadiGraft BLX Putty is moldable, allowing it to conform to the surgical site, and resists migration under irrigation.16 If desired, ReadiGraft BLX Putty can be combined with Bone Marrow Aspirate (BMA), which will provide an osteogenic component. Furthermore, ReadiGraft cortical/cancellous bone chips can be used as a graft extender to aid in healing.
Paprosky Acetabular Revision Classification
The following acetabular revision cases follow the Paprosky classification which is based on the amount of hip center migration and the integrity of four acetabular supporting structures as evaluated on preoperative anteroposterior radiographs of the pelvis.17-19
Paprosky classification is based on:
Key of this classification:
Surgical technique
All patients under epidural anesthesia.
Anterolateral approach.
Lateral positioning with axillary roll and positioners to hold pelvis in stable position.
Interval is between tensor fascia lata and gluteus medius.
The anterior 1/3 of the gluteus medius is taken down to allow greater mobility of the femur and increase vision of the acetabulum.
Reamers were used for acetabular reconstruction and debris removed.
Liners were trialed to determine the proper size.
Case #1 – Paprosky Type 1
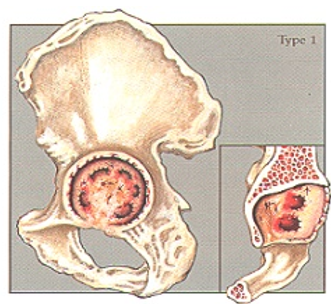
Case description / anamnesis: 72-year-old, male
Left acetabular cup mobilization 8 years postoperative.
Defect has minimal focal bone loss with maintenance of the hemispheric shape of the acetabulum. The supporting structures, including the acetabular walls and columns, are all intact and with no hip center (component) migration.
Treatment:
Old cup was removed.
5cc ReadiGraft BLX Putty was mixed with 15cc of cortical/cancellous chips to fill the acetabular bone void.
Elliptical cup with screws implanted.
Uncemented stem replaced after canal reaming.
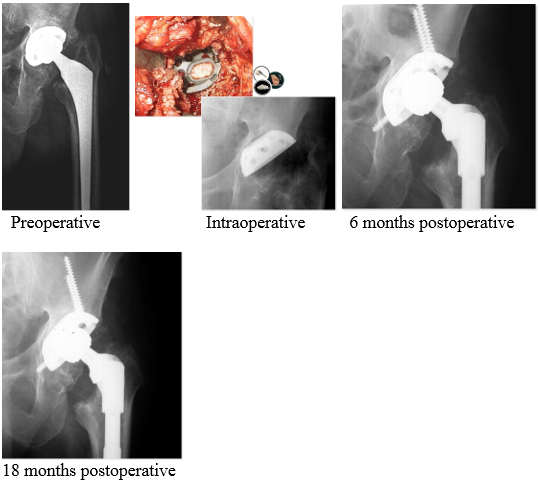
Outcomes:
Postoperative course was uneventful and at 6 months postoperative the cup was completely integrated in the bone.
Case #2 – Paprosky Type 2a
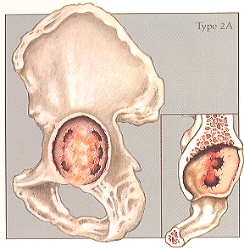
Case description / anamnesis: 71-year-old, female
Left acetabular cup mobilization 8 years postoperative.
Defects are characterized by global cavitation of the acetabulum with direct superior hip center migration, sufficiently intact superior dome and teardrop prevent concomitant lateral or medial displacement, respectively. Anterior column (Kohler line) and ischium (posterior column) intact.
Treatment:
Old cup was removed. Acetabulum preparation using successively larger reamers.
5cc ReadiGraft BLX Putty was mixed with 15cc of cortical/cancellous chips and ilum strip to fill the acetabular bone void.
Cup and screws implanted.
Uncemented stem replaced after canal reaming.
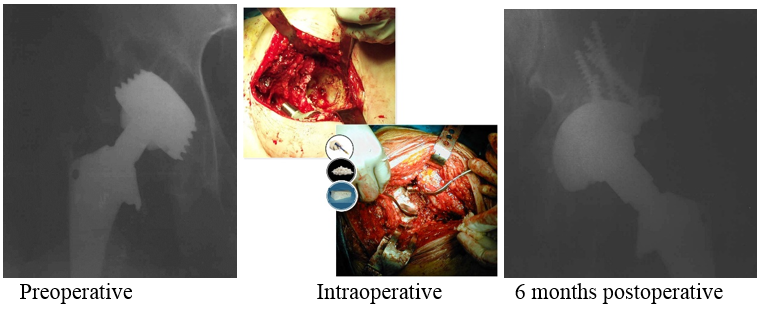
Outcomes:
Postoperative course was uneventful and at 6 months postoperative the cup was completely integrated in the bone.
Case #3 – Paprosky Type 2b
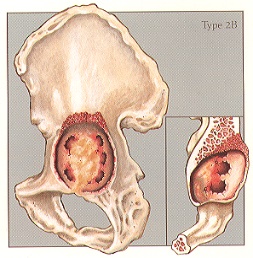
Case description / anamnesis: 78-year-old male
Right acetabular cup mobilization 10 years postoperative.
Defects are characterized by a deficient superior dome, allowing for superior and lateral component migration owing to the lack of a lateral stabilizing buttress, normally provided by the lateral margin of the superior dome.
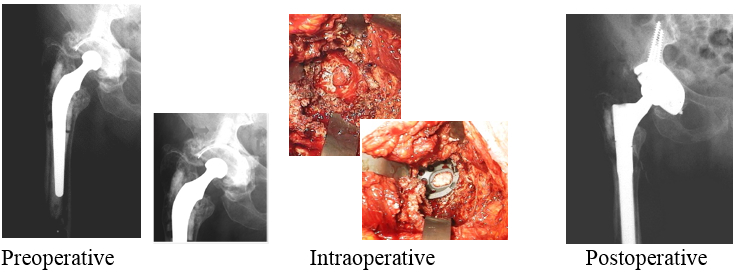
Treatment
Old cup was removed.
15cc ReadiGraft BLX Putty was mixed with 45cc of cortical/cancellous chips to fill the acetabular bone void.
Cage, screws, and cemented cup were replaced.

Outcomes:
Postoperative course was uneventful and the hip was completely restored at 10 months postoperative.
Case #4 – Paprosky Type 2c
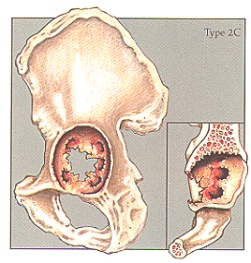
Case description / anamnesis: 80-year-old male
Right acetabular cup mobilization 18 years postoperative.
Defects were characterized by a feicient medial wall (tear drop) causing direct medial migration of hip center. The superior dome is intact, presenting vertical deplacement.
Treatment
Old cup was removed.
15cc ReadiGraft BLX Putty was mixed with 45cc of cortical/cancellous chips to fill the bone void.
Elliptical cup and screws implant.
Uncemented stem replaced after canal reaming.
Outcomes:
Postoperative course was uneventful at 8 months post-operative.
Case #5 – Paprosky Type 3a
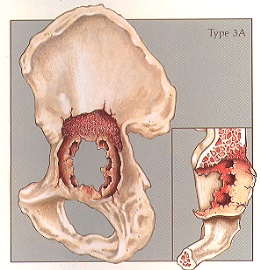
Case description / anamnesis: 68-year-old male
Left acetabular cup mobilization 8 years postoperative.
Defects were characterized by moderate-to-severe destruction of the acetabular walls and posterior column, rendering these structures non-supportive. The hip center migrates super-lateral (up-and-down deformity)
Treatment:
Old cup was removed.
20cc ReadiGraft BLX Putty was mixed with 60cc of cortical/cancellous chips to fill the bone void.
Cup and screws and cemented cup replaced.
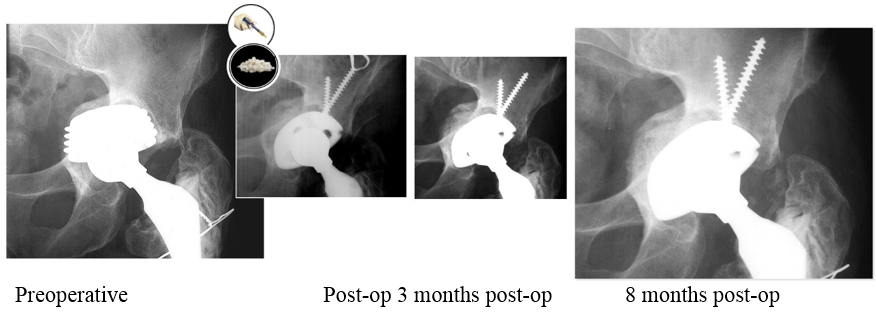
Outcomes:
Postoperative course was uneventful and at 8 months postoperative the cup was completely integrated in the bone.
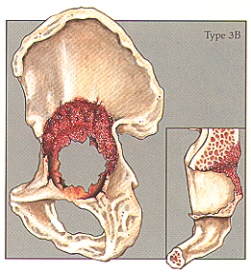
Case #6 – Paprosky Type 3b
Case description / anamnesis: 82-year-old, female
Left acetabular cup mobilization 10 years postoperative.
Defects are most severe and characterized by distruction of all acetabular supporting structure including both walls and both columns (“up-and-in” deformity).
Treatment:
Old cup was removed. Acetabulum preparation using successively larger reamers.
15cc ReadiGraft BLX Putty was mixed up with 45cc of cortical/cancellous and ilum strip to fill the acetabular bone void.to fill the acetabular bone void.
Cage and screws and cemented cup replaced.
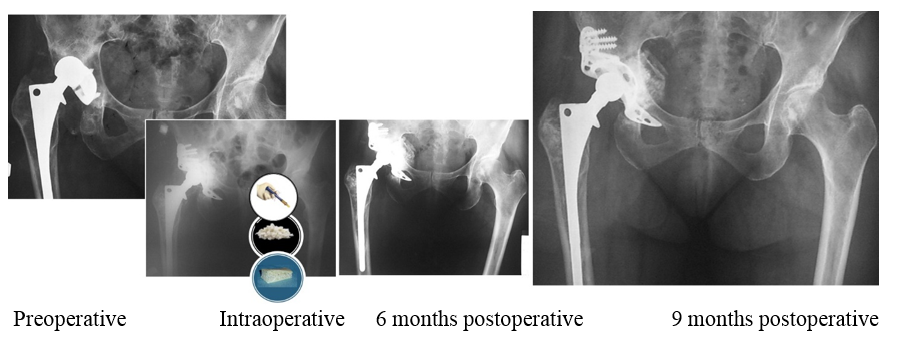
Outcomes:
Postoperative course was uneventful and at 9 months postoepartive the hip was restored.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org