Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Masume Sohrabi, Sima Koohestani, Amir Shokri, Naser Shagerdi Esmaeli, Shahin Asadi*
Medical Genetics Director of the Division of Medical Genetics and Molecular Pathology Research, Center of Complex Disease, U.S.A.
*Corresponding author: Shahin Asadi, Medical Genetics Director of the Division of Medical Genetics and Molecular Pathology Research, Center of Complex Disease, U.S.A.
Received: December 05, 2024
Accepted: December 13, 2024
Published: December 16, 2024
Citation: Masume Sohrabi, Sima Koohestani, Amir Shokri, Naser Shagerdi Esmaeli and Shahin Asadi. (2024). “A Comprehensive Review of Trisomy 9p Syndrome”. Clinical Case Reports and Clinical Study, 11(3); DOI: 10.61148/2766-8614/JCCRCS/189
Copyright: © 2024. Shahin Asadi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Trisomy 9p syndrome is a rare chromosomal disorder in which a portion of chromosome 9 appears three times (trisomy) instead of two times in the bodys cells. In trisomy 9p syndrome, the trisomy (or duplicated material) may involve part of the short arm (9p), the entire short arm, or one of the short arm and part of the long arm (9q) of chromosome 9. In many cases, the symptoms and associated findings may be relatively similar among affected infants despite the varying lengths of the trisomy (duplicated) portion of 9p. The specific symptoms of trisomy 9p can vary greatly from person to person, partly because of the specific length of the repeated material on chromosome 9p. Trisomy 9p is often characterized by low muscle tone (hypotonia) as well as growth failure and delayed bone maturation, meaning that the bones grow and develop more slowly than in people with 46 chromosomes. Hypotonia can affect infants, often associated with feeding difficulties, resulting in failure to gain weight and grow at the expected rate (growth failure). Many people with trisomy 9p may have various abnormalities of the hands and feet. These may include a reduction in the length of certain bones in the fingers and toes (phalanges) and in the hands (metacarpals) and feet (metatarsals). Short fingers and toes (digits) with small nails; or the smaller fingers may be fixed or locked in a bent position (clinodactyly). The syndrome may also be associated with unusual and distinctive skin ridge patterns in the fingers and hands (abnormal dermatoglyphics), including a single flexor crease on the fifth finger and a reduction in the total number of ridges on the fingers. In rare cases, there may also be a crease on the palm of the hand. In approximately 50% of cases, trisomy 9p may be due to a balanced chromosomal rearrangement in one of the parents. In most cases, the parental rearrangement is described as a “balanced translocation.” Translocations occur when parts of a chromosome break off and rearrange, resulting in the shifting of genetic material and a change in the set of chromosomes. However, no genetic material is gained or lost, it is just rearranged.
Overview of Trisomy 9p Syndrome:
Trisomy 9p syndrome is a rare chromosomal disorder in which a portion of chromosome 9 appears three times (trisomy) instead of two times in the bodys cells. In trisomy 9p syndrome, the trisomy (or duplicated material) may involve part of the short arm (9p), the entire short arm, or one of the short arm and part of the long arm (9q) of chromosome 9. In many cases, the symptoms and associated findings may be relatively similar among affected infants despite the varying lengths of the trisomy (duplicated) portion of 9p. However, in those with larger trisomy (for example, extending into the middle or distal regions of 9q), additional features may also be present that appear to be related to the extent of the duplication. In addition, certain individuals with duplications of specific regions of chromosome 9p have no symptoms or only very mild or subtle symptoms [1].
Children with trisomy 9p are affected by delays in reaching developmental milestones including crawling or walking (developmental delay), growth failure, and characteristic abnormalities of the skull and facial area (craniofacial region). As children get older, intellectual disability may become apparent. In some cases, additional physical abnormalities may also be present, such as other skeletal defects or structural heart abnormalities present at birth (congenital heart defects). In some cases, the trisomy appears to result from a balanced chromosomal rearrangement in one of the parents. In others, it is thought to result from spontaneous (de novo) errors very early in embryonic development that occur for unknown reasons (sporadically) [1].
Clinical Signs and Symptoms of Trisomy 9p Syndrome:
The specific symptoms of trisomy 9p can vary greatly from person to person, partly because of the specific length of the repeated material on chromosome 9p. Trisomy 9p is often characterized by low muscle tone (hypotonia) as well as growth failure and delayed bone maturation, meaning that the bones grow and develop more slowly than in people with 46 chromosomes. Hypotonia can affect infants, often associated with feeding difficulties, resulting in failure to gain weight and grow at the expected rate (growth failure). In general, growth failure begins primarily after birth. Some infants may have oropharyngeal dysphagia, in which it is difficult to empty food or drink from the back of the throat at the back of the mouth (oropharynx) into the esophagus. However, reports suggest that in those with larger trisomy segments (e.g., through bands 9q22 or 9q32), growth retardation may begin before birth (intrauterine growth retardation). Microcephaly, a condition in which the head circumference is smaller than expected for the age and sex of the infant, is also evident in infancy. In many cases, trisomy 9p is associated with varying degrees of intellectual disability, ranging from moderate to severe, and delays in the acquisition of skills that require coordination of mental and physical activities (developmental coordination disorder). Language development appears to be severely delayed, according to reports in the medical literature. Learning disabilities, ranging from mild to severe, also occur. Intellectual and learning problems go hand in hand. Intellectual and learning disabilities show a wide spectrum, especially when children with partial trisomy 9p are also considered. The gap with normally developing peers often widens with age [2].
Many infants and children with trisomy 9p also have a distinctive appearance. Most people with the condition present with a short, broad head (brachycephaly); a wide mouth with down-turned corners; a prominent, somewhat bulbous nose; large, low-set, "cup-shaped" ears; and/or a short vertical groove in the center of the upper lip (philtrum). Distinctive eye abnormalities may also be present, such as deep-set, widely spaced eyes; downward-slanting eyelid creases (palmar clefts); vertical folds of skin that may cover the inner corners of the eyes (epicanthal folds); or an abnormal deviation of one eye relative to the other (strabismus). Some affected infants may also have a short neck, a very arched roof of the mouth (palate); or widely spaced nipples. Teeth may erupt later than expected and may be crooked. In addition, in people with larger trisomy segments, additional craniofacial features may include a small jaw (micrognathia), incomplete closure (cleft) of the roof of the mouth (cleft palate), or an abnormal groove or gap in the upper lip (cleft lip) [2].
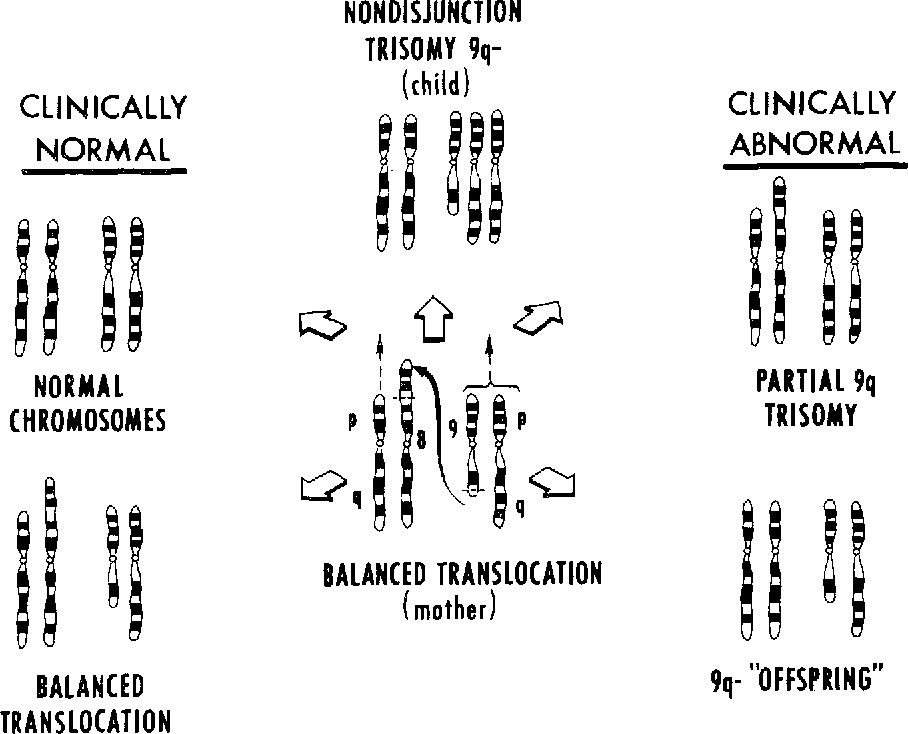
Figure 1: Schematic of chromosome number 9 disorders [1]
Many people with trisomy 9p may have various abnormalities of the hands and feet. These may include a reduction in the length of certain bones in the fingers and toes (phalanges) and in the hands (metacarpals) and feet (metatarsals). Short fingers and toes (digits) with small nails; or the smaller fingers may be fixed or locked in a bent position (clinodactyly). The syndrome may also be associated with unusual and distinctive skin ridge patterns in the fingers and hands (abnormal dermatoglyphics), including a single flexor crease on the fifth finger and a reduction in the total number of ridges on the fingers. In rare cases, there may also be a crease on the palm of the hand. In some cases, trisomy 9p may be associated with skeletal defects, including delayed closure of the "soft spots" (fontanelles) and fibrous joints (cranial sutures) between some of the bones of the skull; A deformity in which the foot is twisted out of shape or position (clubfoot), or an abnormal forward-backward or side-to-side curvature of the spine (kyphoscoliosis), which may develop in the second decade of life. Less commonly, partial fusion (syndactyly) of the fingers and toes and dislocation of the hip have been seen at birth [3].
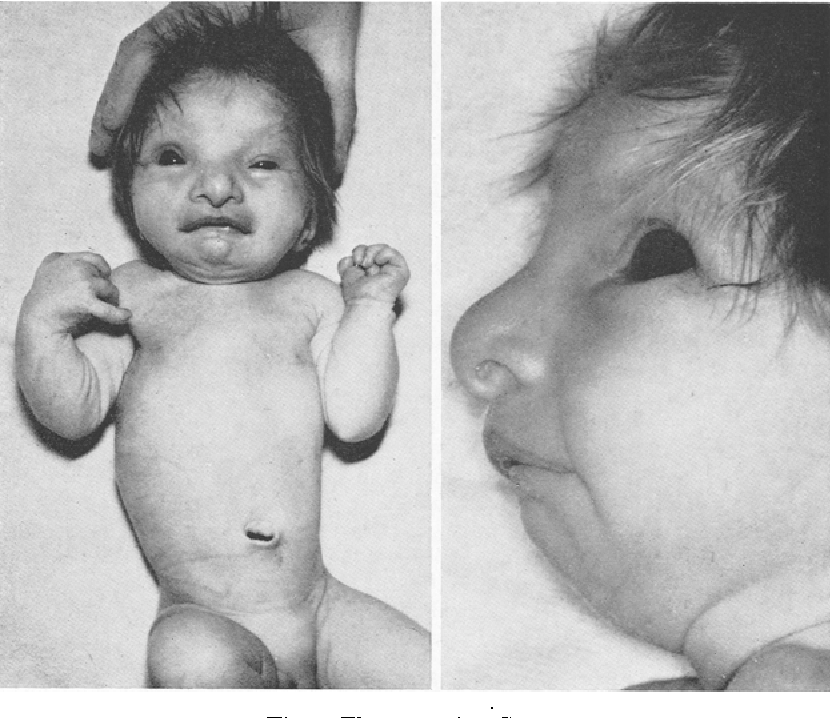
Figure 2: Image of a baby with trisomy 9p syndrome [1].
Approximately 5 to 25 percent of affected children may also have congenital heart defects, specifically an abnormal hole in the partition (septum) that separates the two lower chambers (ventricles) of the heart (ventricular septal defects [VSDs]). In people with heart defects, the signs and symptoms may vary depending on the size, nature, or combination of the heart defects present. For example, in some cases, such as those with small, isolated VSDs, there may be no obvious symptoms (asymptomatic). However, in other cases, such as in children with larger VSDs or other heart defects, the signs and symptoms may include feeding difficulties, shortness of breath, excessive sweating, irritability, fatigue, and a bluish discoloration of the skin (cyanosis) or mucous membranes. In severe cases, congenital heart disease may lead to potentially life-threatening complications. Surgery may be necessary to correct the heart defect, along with follow-up care and monitoring [3].
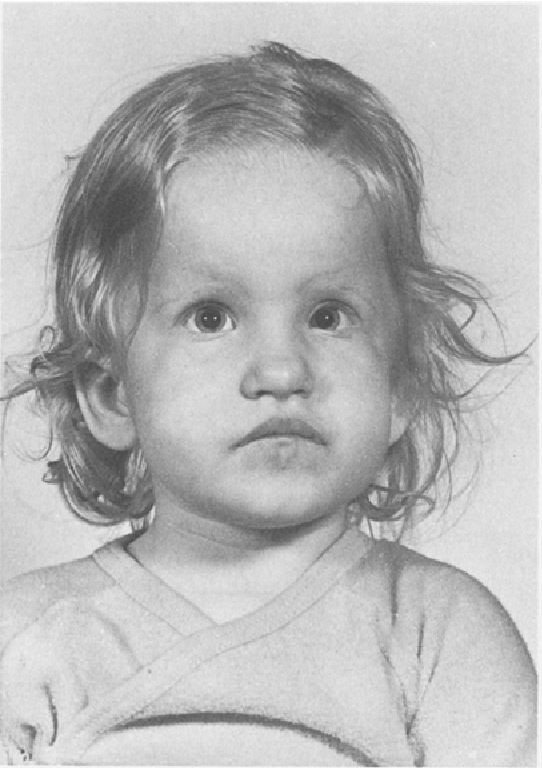
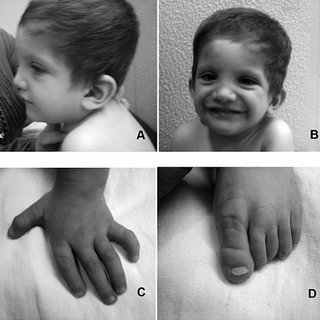
Figure 3: Other images of children with trisomy 9p syndrome [1].
In some cases, additional physical abnormalities have been reported. These include genital abnormalities in affected males, such as undescended testicles or abnormal placement of the urethra (hypospadias) on the underside of the penis. Kidney (renal) abnormalities; protrusion of part of the intestine and the fatty membrane in front of the intestine (omentum) through a defect in the abdominal wall at the navel (umbilical hernia); or hydrocephalus, in which the blockage of the normal flow of spinal fluid leads to an excessive accumulation of cerebrospinal fluid (CSF) in and around the brain. This leads to abnormally high pressure inside the skull and swelling of the head and can lead to neurological impairment. CSF is a watery protective fluid that lines the cavities (ventricles) of the brain, the canal containing the spinal cord (spinal canal), and the space between the layers of protective membranes (meninges) surrounding the brain and spinal cord (the subarachnoid space). Depending on the age of onset and other factors, associated symptoms may include sudden episodes of uncontrolled bioelectrical activity in the brain (seizures), irritability, vomiting, headache, loss of coordination, worsening mental function, or other findings. Some people may also have a brain abnormality known as Dandy-Walker anomaly (DWM). DWM occurs during fetal development of the cerebellum and fourth ventricle. The cerebellum is an area at the back of the brain that helps coordinate movement and may be involved to some extent with some cognitive and behavioral functions. The fourth ventricle is a space around the cerebellum that drains fluid from the inside to the outside of the brain. DWM is characterized by abnormal development (i.e., small size and abnormal position) of the middle part of the cerebellum, known as the cerebellar vermis, cystic enlargement of the fourth ventricle, and enlargement of the base of the skull (posterior fossa). DWM may be associated with hydrocephalus. Affected children may be shorter than average for their age (short stature). In some cases, children have been diagnosed with growth hormone deficiency [4].
Etiology of Trisomy 9p Syndrome:
In many cases, the trisomy appears to be caused by spontaneous (de novo) errors very early in embryonic development that occur for unknown reasons (sporadically). In such new cases, the parents of the affected child usually have normal chromosomes and have a relatively low risk of having another child with the chromosomal abnormality. In approximately 50% of cases, trisomy 9p may be due to a balanced chromosomal rearrangement in one of the parents. In most cases, the parental rearrangement is described as a “balanced translocation.” Translocations occur when parts of a chromosome break off and rearrange, resulting in the shifting of genetic material and a change in the set of chromosomes. However, no genetic material is gained or lost, it is just rearranged. If a chromosomal rearrangement is balanced, meaning that it consists of an altered but balanced set of chromosomes, it is usually harmless to the carrier. However, such a chromosomal rearrangement may be associated with an increased risk of abnormal chromosome development in the carriers offspring. Such children may inherit an unchanged set of chromosomes, the same as the parents balanced translocation, or an unbalanced translocation in which the chromosome has extra (trisomy) or missing (monosomy) genetic material [4].
Rare cases have also been reported in which the parents chromosomal rearrangement was inverted. An inversion is characterized by a chromosome breaking at two locations and rejoining the segments in the reverse order of the original arrangement. Chromosomal analysis and genetic counseling are usually recommended for the parents of an affected child to help confirm or rule out the presence of a balanced translocation or other chromosomal rearrangement involving chromosome 9 in one of the parents [4].
Specific Breakpoints and "Critical Regions":
In individuals with trisomy 9p, all or part of the short (p) arm of chromosome 9 (9p) appears three times (trisomy) instead of twice in the bodys cells. In addition, in some cases, part of the long arm of chromosome 9 (9q) may also be trisomy (duplication). In very rare cases, individuals with trisomy 9p may also have a deleted or missing segment (monosomy) [5].
Evidence suggests that in many cases, clinical features may be relatively similar among affected individuals despite the varying lengths of the 9p repeat segment. According to some researchers, such findings suggest that some of the characteristic abnormalities associated with the syndrome may be due to trisomy of the distal portion of 9p. ("Distal" refers to the farthest or furthest point of reference, meaning the centromere of the chromosome. The distal region of 9p is sometimes referred to as "9p2" and includes bands 9p21 through 9p24, the latter being the end or "terminal" band of 9p [also known as "9pter"). However, in individuals with larger trisomies, such as those extending from bands 9p22, there may be other clinical findings that appear to be related to the extent of the duplication [5].
In general, according to the researchers, trisomies that involve part or all of 9p and, in some cases, extend to 9q11-13 may be characterized by intellectual disability and the distinctive craniofacial anomalies described earlier. However, in addition to such features, intrauterine growth retardation, congenital heart defects, other skeletal anomalies (such as congenital dislocation of the hip), and additional craniofacial anomalies (such as micrognathia, cleft lip, and cleft palate) are more common with trisomies that extend to or beyond band 9p21.3-p24. Researchers believe that 9p22 is a "critical" region responsible for most of the classic symptoms of trisomy 9p. However, individuals have been reported in the medical literature to have duplicates in this region and to have only mild symptoms. Further research is needed to determine the specific association between the 9p duplication and associated symptoms and whether additional factors, such as modifier genes, play a role in causing specific symptoms in each individual case. Twice in the bodys cells In addition, in some cases, part of the long arm of chromosome 9 (9q) may also be trisomy (duplication). In very rare cases, people with trisomy 9p may also have a deleted or missing segment (monosomy) [5].
Frequency of Trisomy 9p Syndrome:
In observed cases, trisomy 9p appears to affect women approximately twice as often as men. As of 2013, more than 150 cases have been reported in the medical literature since the disorder was first described in 1970. Trisomy 9p is the fourth most common type of trisomy after trisomy 21 (Down syndrome), trisomy 18 (Edwards syndrome), and trisomy 13 (Patau syndrome) [6].
Disorders Associated with Trisomy 9p Syndrome:
The symptoms of the following disorders may be similar to those of trisomy 9p. Comparison may be helpful in the differential diagnosis:
Chromosome 9, Tetrasomy 9p is a rare chromosomal disorder in which the short arm of chromosome 9 (9p) is present four times (tetrasomy) instead of twice in all or some of the bodys cells. Although many of the associated symptoms and findings may be similar to those seen in people with trisomy 9p, researchers suggest that such features may be more variable or severe in some cases. Characteristic abnormalities associated with tetrasomy 9p may include growth failure, developmental coordination disorder; moderate to severe intellectual disability; and various craniofacial, skeletal, cardiac, renal, or other physical defects. Cranial abnormalities may resemble those associated with trisomy 9p, such as a bulbous nose. Low-set, malformed ears; a downward-slanting mouth; deep-set, widely spaced eyes; a short neck; and/or other features of microcephaly, a condition in which the head circumference is smaller than expected for the age and sex of the baby, are also evident in infancy. Tetrasomy 9p appears to result from spontaneous (de novo) errors very early in embryonic development that occur randomly for unknown reasons. Mosaic trisomy of chromosome 9 is a chromosomal disorder characterized by trisomy of the entire ninth chromosome in some cells of the body (mosaicism). The term "mosaicism" indicates that a percentage of the affected individuals cells have the chromosomal abnormality, while other cells may have normal chromosomal structure. The range and severity of symptoms and associated findings may depend on the percentage of cells with the extra chromosome. Characteristic features may include prenatal growth retardation (intrauterine growth retardation), congenital heart defects; Skeletal, genital, renal, or neurological abnormalities; or variable craniofacial defects, such as bulbous nose, short eyelid creases (palmar clefts), deep-set eyes, small jaw (micrognathia), poorly formed and malformed ears, short neck, or other abnormalities. Mosaic trisomy 9 may be caused by errors during the division of parental reproductive cells (meiosis) or during the division of body tissue cells (somatic cells) early in fetal development (mitosis). The cause of such errors is not known. Additional chromosomal abnormalities may present with symptoms and findings similar to those of trisomy 9p. Chromosomal testing is necessary to confirm the specific chromosomal abnormality present [6].
Diagnosis of Trisomy 9p Syndrome:
In some cases, a diagnosis of trisomy 9p may be suggested before birth (fetal) with specialized tests such as ultrasound, amniocentesis, or chorionic villus sampling (CVS). During a fetal ultrasound, reflected sound waves create an image of the developing fetus, potentially revealing characteristic findings that indicate a chromosomal disorder or other developmental abnormality. During amniocentesis, a sample of the fluid surrounding the developing fetus is removed and analyzed, while CVS involves removing tissue samples from part of the placenta. Chromosomal studies performed on such fluid or tissue samples may reveal trisomy of part or all of the short arm of chromosome 9 (9p) and, in some cases, part of the long arm (9q). Trisomy 9p may also be diagnosed or confirmed after birth by a thorough clinical evaluation, identification of specific physical findings, chromosome analysis, and other specialized tests. Chromosomes can be obtained from a blood sample [6].
There are several tests that can be performed on tissue samples for chromosome analysis. Chromosomes obtained from tissue samples are stained to make them easier to see and then examined under a microscope where the duplicated portion of chromosome 9p can be identified (high-resolution karyotyping). To determine the exact breakpoint on 9p, a more sensitive test may be needed, such as fluorescent in situ hybridization (FISH), a diagnostic test in which probes labeled with a specific color of fluorescent dye are attached to a specific chromosome, allowing researchers to better see which region of the chromosome is affected; Array comparative genomic hybridization (CGH) is a method in which normal DNA is mixed with patient DNA to analyze gains (duplications) or losses (deletions) of chromosomal regions. Array CGH allows for better definition of breakpoints in trisomy 9p, but cannot detect balanced rearrangements (such as balanced translocations that can sometimes be detected in one of the parents of an affected child) [6].
In some cases, the diagnostic evaluation may include enzyme tests to detect increased activity of the enzyme galactose-1-phosphate uridyl transferase (GALT) or the enzyme nucleoside triphosphate adenylate kinase (AK3), both of which are regulated by genes on the short arm of chromosome 9. In addition, in individuals diagnosed with trisomy 9p, various specialized tests may be performed to help identify or characterize specific abnormalities (such as specific skeletal abnormalities, congenital heart defects, etc.) that may be associated with the syndrome [6].
Treatment Pathways for Trisomy 9p Syndrome:
Treatment for trisomy 9p is directed toward the specific symptoms and physical findings that are present in each individual. Such treatment may involve the coordinated efforts of a team of medical specialists such as pediatricians, surgeons; Doctors who diagnose and treat abnormalities of the skeleton, joints, muscles, and related tissues (orthopedic specialists); doctors who specialize in heart abnormalities (cardiologists); neurologists; and other health care professionals may be needed. Genetic counseling is recommended for families with children with this condition. Psychosocial support for the entire family may also be needed [7].
Early intervention services in infancy and toddlerhood (before age three) are important in ensuring that affected children reach their potential. Early speech therapy is especially important for children who experience severe communication and language difficulties. Specialized services that may be helpful in early childhood include special education, physical therapy, occupational therapy, speech therapy, or other medical and social services. In the United States, an Individual Family Support Plan (IFSP) may be developed to guide the early intervention process for infants and toddlers with disabilities. An Individualized Education Program (IEP) may be developed to help children in school if they need special services, or a plan that can ensure that the child has equal access to education through accommodation in their educational setting. Vocational and rehabilitation services are often necessary in adulthood [7].
Additional treatment for this disorder is symptomatic. For example, for congenital heart defects, medication, surgical intervention (salvage or corrective), and/or other measures may be needed. In addition, in some cases, doctors may recommend repair or correction of characteristic craniofacial abnormalities, skeletal abnormalities, genital defects, hernias, renal abnormalities, or other abnormalities associated with the disorder. The specific surgical procedures performed depend on the nature and severity of the anatomical abnormalities, their associated symptoms, and other factors. In addition, growth hormone deficiency has been successfully treated with supplemental growth hormone [7].
Discussion:
This chromosomal abnormality was first reported in the medical literature in 1970. Trisomy 9p was first described as a distinct syndrome with characteristic symptoms and findings in 1975. Children with trisomy 9p are affected by delays in reaching developmental milestones including crawling or walking (developmental delay), growth failure, and characteristic abnormalities of the skull and facial area (craniofacial region). As children get older, intellectual disability may become apparent. In some cases, additional physical abnormalities may also be present, such as other skeletal defects or structural heart abnormalities present at birth (congenital heart defects). Trisomy 9p is often characterized by low muscle tone (hypotonia) as well as growth failure and delayed bone maturation, meaning that the bones grow and develop more slowly than in people with 46 chromosomes. Hypotonia can affect infants, often associated with feeding difficulties, resulting in failure to gain weight and grow at the expected rate (growth failure). In general, growth failure begins primarily after birth. Some infants may have oropharyngeal dysphagia, in which it is difficult to empty food or drink from the back of the throat at the back of the mouth (oropharynx) into the esophagus. If a chromosomal rearrangement is balanced, meaning that it consists of an altered but balanced set of chromosomes, it is usually harmless to the carrier. However, such a chromosomal rearrangement may be associated with an increased risk of abnormal chromosome development in the carriers offspring. In general, according to the researchers, trisomies that involve part or all of 9p and, in some cases, extend to 9q11-13 may be characterized by intellectual disability and the distinctive craniofacial anomalies described earlier. However, in addition to such features, intrauterine growth retardation, congenital heart defects, other skeletal anomalies (such as congenital dislocation of the hip), and additional craniofacial anomalies (such as micrognathia, cleft lip, and cleft palate) are more common with trisomies that extend to or beyond band 9p21.3-p24. Researchers believe that 9p22 is a "critical" region responsible for most of the classic symptoms of trisomy 9p. There are several tests that can be performed on tissue samples for chromosome analysis. Chromosomes obtained from tissue samples are stained to make them easier to see and then examined under a microscope where the duplicated portion of chromosome 9p can be identified (high-resolution karyotyping). Treatment for trisomy 9p is directed toward the specific symptoms and physical findings that are present in each individual. Early intervention services in infancy and toddlerhood (before age three) are important in ensuring that affected children reach their potential. Early speech therapy is especially important for children who experience severe communication and language difficulties [1-7].














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org