Case Reports International Journal
OPEN ACCESS | Volume 4 - Issue 1 - 2026
ISSN No: 3065-6710 | Journal DOI: 10.61148/ 3065-6710/CRIJ


Abdelmoneim Elhadidy1*, Abdelmoneim Elorbany2, Emad Balah1, Samir Elsherbiny1, Sayed Gamal1, Nermeen El Ghandour2, Amira Hodiehd3
1Gastroenterology and Hepatology department, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
2Clinical pharmacy department, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
3Clinical Pathology and Microbiology, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
*Corresponding author: Abdelmoneim Elhadidy, Gastroenterology and Hepatology department, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
Received: April 20, 2026 | Accepted: May 08, 2026 | Published: May 12, 2026
Citation: Elhadidy A, Elorbany A, Balah E, Elsherbiny S, Gamal S, Nermeen El Ghandour, Hodiehd A., (2026). “Purulent meningitis Unusual Presentation Complicated by Transverse Myelitis, Rare Case Report” Case Reports International Journal, 4(2); DOI: 10.61148/3065-6710/CRIJ/034.
Copyright: © 2026 Abdelmoneim Elhadidy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Bacterial meningitis is an infection of the meninges that results in inflammation. It is a serious and life-threatening condition that requires prompt diagnosis and treatment. This activity reviews the evaluation and treatment of bacterial meningitis and highlights the role of the interprofessional team in caring for patients with this condition.
Purulent meningitis is a critical bacterial infection targeting the subarachnoid space, constituting a medical emergency that demands immediate diagnosis and treatment. Delays in intervention can significantly jeopardize both survival and long-term functional outcomes for the patient. Effective management depends on the prompt initiation of bactericidal antibiotics selected empirically based on the patient's clinical presentation, predisposing factors, and local epidemiological patterns. Subsequent treatment is refined according to the specific pathogen identified during cerebrospinal fluid (CSF) analysis. The growing prevalence of penicillin-resistant *Streptococcus pneumoniae* has necessitated updates to conventional antibiotic regimens.
While acute meningitis is primarily linked to intracranial complications, it can occasionally lead to spinal cord dysfunction. The main mechanisms underlying such dysfunction include spinal cord compression, ischemic infarction, and acute myelitis. Magnetic resonance imaging (MRI) of the spinal cord serves as the diagnostic modality of choice, as it not only excludes compressive lesions but also confirms the presence of myelitis. Characteristic MRI findings in myelitis often reveal hyperintensities on T2-weighted images, notably affecting the gray matter and frequently spanning from the cervical to lumbar segments of the spine. Patients with such complications are at risk of enduring neurological deficits, including spasticity, muscle weakness, impaired mobility, and problems with bowel or bladder control. Here, we discuss a case of acute meningitis complicated by the development of acute transverse myelitis.
Bacterial meningitis is a severe infection that affects the meninges, the protective layers surrounding the brain and spinal cord, leading to inflammation. This condition is both serious and life-threatening, demanding immediate diagnosis and treatment.[1][2][3] Acute meningitis can lead to various intracranial complications, including cerebrovascular accidents, brain edema, hydrocephalus, and hearing impairment. Additionally, it may result in systemic issues such as septic shock, adult respiratory distress syndrome, or disseminated intravascular coagulation. [4] While spinal cord dysfunction is typically a rare complication, it is more frequently observed in children but has also been documented in adults. [5]
Acute Transverse Myelitis (ATM) constitutes a rare neuroimmune condition characterized by inflammation of the spinal cord. The disorder is typically marked by the rapid onset of muscle weakness, disturbances in sensory function, and impairments in bowel or bladder regulation. (6). Although it primarily manifests in adults, its occurrence among children, especially those under the age of two, is notably less common. (7,8)
The causes range from spinal cord compression to ischemic infarction and acute myelitis. Compression may result from a spinal abscess or hemorrhage following a lumbar puncture, while infarction could stem from conditions such as vasculitis, shock, herniation, or arachnoiditis. Acute transverse myelitis, though uncommon, accounts for 1 to 4 cases per million annually as a cause of myelopathy.[9] We report a case of a 47-year-old gentleman with acute meningitis, who developed Acute transverse myelitis as a complication which was confirmed by magnetic resonance imaging (MRI) of the spine.
Case Report
A 47-year-old man from Damietta presented with a 3-day history of headache, fever, vomiting after then neck pain and rigidity and disturbed level of consciousness. He was previously healthy and had no medical history in the past. He is married and is working as a carpenter. He is a smoker and nonalcoholic. He was admitted as a case of suspected meningoencephalitis. Initial laboratory tests in the Emergency Department showed a WBC count of 33,600/uL with 85% neutrophils, hemoglobin 11.2gm/dl, platelets 435,000/uL, Creatinine 1.3 mg l/dl, calcium 9.0mg l/dl, EBG normal. An ECG showed sinus tachycardia, chest x-ray was normal, head CT scan was normal.
An urgent cerebrospinal fluid (CSF) examination showed very tick CSF not flow in spinal needle and aspirated by syringe Purulent aspect with high white blood cell (WBC) of 114400 (90% neutrophils), very high protein of 140 g/L, very low glucose less than 10 g/L (<50% of serum glucose), and Gram stain and culture of CSF were negative. The CSF viral panel, tuberculosis (TB) smears and cultures, and TB polymerase chain reaction were negative. Radiological CT brain revealed normal and MRI revealed diffuse abnormal S1 of both temporal lobes involving mainly white matters and more the left side. It extends to involve most of left basal Anglia and mildly to right basal ganglia. It also extends to left cerebral hemisphere. It displays high signal on FLAIR and T2WI and low signal on TIWI highly suggested encephalitis.
Based on the CSF findings as well as systemic signs, a presumptive diagnosis of Purulent meningococcal sepsis was made and Meropenem (2 g every 8 hours I.V.) ,Vancomycin (1g every 8 houres) and Dexamethasone given at the time of antibiotic administration, follow up labaratory as table (1) . On day 5 of admission, her impaired consciousness persisted; therefore, we decided to repeat lumber puncture revealed marked decrease of WBC but still high and very low glucose ,after 8th day the level of consciousness improved and temprature became normal .
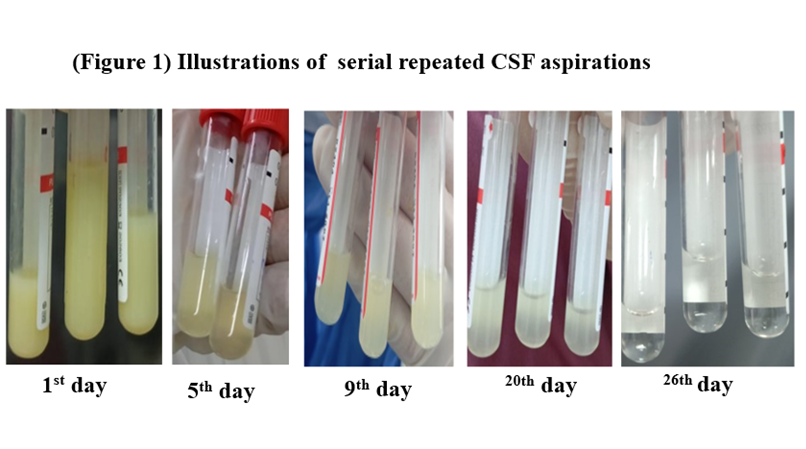
Repeated CSF analysis because unusual purulent as follow up in a 5th day ,9th day ,20th day and lastly in 25th day before discharge time showed improvement as in (Table 2).
As the patient showed very slow recovery, the power in the lower limbs worsened to zero in 15th days of admission; therefore, an urgent MRI spine was done which demonstrated Swollen upper dorsal cord with slight increased S1on T2W1, Finding is suggesting transverse myelitis. MRI brain was normal, consultation of neurological to follow up.
The patient was therefore considered disease-free in 25th day and was committed to a neurology for monitoring transverse myelitis and rehabilitation center.
Figure 1: Routine peripheral blood test results.
|
Date |
1st day |
4th day |
8th day |
15th day |
20th day |
25th day |
|
WBC |
33,600/uL |
22.300 |
18.800 |
12.700 |
10.300 |
8.300 |
|
Neutrophil |
85% |
84% |
86% |
75% |
76% |
72% |
|
Hemoglobin |
11.2gm/dl |
8 |
9 |
10.2 |
10.7 |
11,0 |
|
platelets |
435,000/uL |
410,000 |
390,000 |
380000 |
360000 |
350000 |
|
Creatinine |
1.3 |
0.9 |
0.8 |
0.8 |
0.7 |
0.6 |
Figure 2: Serial CSF reports during the course of illness.
|
Date |
1st day |
5th day |
9th day |
20th day |
26th day |
|
WBC |
114400 |
28400 |
6300 |
500 |
20 |
|
Neutrophil |
98% |
95% |
93% |
90 |
70 |
|
Protein |
140 g/d |
80 g/d |
66 g/d |
42 g/d |
30 g/d |
|
Glucose |
Less than 10 |
Less than 10 |
Less than 10 |
25 g/d |
55 g/d |
Discussion
Bacterial meningitis can be complicated by a variety of systemic and neurological complications; spinal cord involvement is a rare complication, and its occurrence in early childhood is rare. Between 1971 and 2001, only 29 cases had been reported: four adults and 25 children [10]. The condition is most prevalent in people between the ages of 10 and 19 or between 30 and 39 [11]. The possible causes of spinal cord dysfunction in acute meningitis are mass effects, i.e., cord compression, vascular compromise, or myelitis [12].
Our case report is an example of a rare complication of acute meningitis in adults. The usual causes of spinal cord dysfunction in acute meningitis are compression by spinal abscess, epidural hemorrhage, and ischemic infarction of the cord due to vascular compromise.[13]
The most common initial symptoms include motor issues like quadriplegia or paraplegia, sensory disturbances, and bladder and bowel dysfunction. Spinal cord symptoms typically manifest at the time of meningitis diagnosis, persisting for varying durations, with some patients experiencing lasting impairments. Frequently reported residual effects include spasticity, weakness, difficulty walking, and continued bladder and bowel dysfunction. [14]
Myelitis was the cause in our case, as confirmed by an MRI of the spinal cord, which showed demonstrated Swollen upper dorsal cord with slight increased S1on T2W1, Finding is suggesting transverse myelitis. The most frequent initial symptoms are quadriplegia or paraplegia.
Cord dysfunction does not appear to be linked to the causative organism of meningitis, as it has even been observed in cases where no organism was isolated. [15] In our case, no bacterial organism was identified, and tests for tuberculosis and viral infections returned negative results. Evaluating patients with suspected cord dysfunction requires the use of spinal MRI, which is essential. [16] This imaging helps rule out compression and differentiate between various forms of transverse myelitis, as prognosis, recurrence risk, and treatment options may vary significantly between these conditions. [17 ]
Studies indicate that myelitis associated with acute bacterial meningitis is linked to a poor prognosis. Kathryn's review of 23 cases involving patients with spinal cord dysfunction revealed five fatalities, all occurring in children, including four neonates with E. coli meningitis. Among the 18 survivors, only two achieved complete neurological recovery. The remaining 16 survivors experienced persistent deficits such as spasticity, weakness, walking impairments, and issues with bowel and bladder function. [18] In our case, the patient exhibited moderate residual weakness in the lower limbs along with bladder and bowel dysfunction.
Conclusion
Bacterial meningitis can lead to complications involving spinal cord dysfunction, which may arise from factors such as cord compression, vasculitis, autoimmune myelopathy, or direct cord infection (myelitis). When evaluating a patient with meningitis, it is essential to promptly consider the possibility of spinal cord lesions. These lesions are associated with a poor prognosis and have the potential to cause lasting neurological impairments ranging from moderate to severe. However, timely management significantly improves the outcome.
Acknowledgements
Not applicable.
Authors and Affiliations
Gastroenterology and Hepatology department, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
Abdelmoneim Elhadidy & Abdelmoneim Elorbany& Emad Balah
&Samir Elsherbiny & Sayed Gamal.
Clinical pharmacy department, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
Nermeen El Ghandour
Clinical Pathology and Microbiology, Damietta Fever and Gastroenterology hospital, Ministry of Health and Population, Egypt.
Amira Hodiehd
Authors’ contributions
All authors are responsible for the modification and giving final approval of the manuscript. Abdelmoneim Elhadidy was a contributor in writing the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no funding for this study.
Availability of data and materials
Please contact the corresponding author for data requests.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org