Aditum Journal of Clinical and Biomedical Research
OPEN ACCESS | Volume 7 - Issue 1 - 2025
ISSN No: 2993-9968 | Journal DOI: 10.61148/2993-9968/AJCBR


Kabwe Chipalo*, Noudjoutoubaye Moun-goss, Mahamat Langaba Achair, Hamza Lakdim, Omar Zerrari, Hatim Abid, Mohammed El Idrissi, Abdelmajid El Mrini
Department of Traumatology and Orthopaedic Surgery, Hassan II University Teaching Hospital, Fez, Morocco.
*Corresponding author: Kabwe Chipalo, Department of Traumatology and Orthopaedic Surgery, Hassan II University Teaching Hospital, Fez, Morocco.
Received: November 05, 2025 | Accepted: November 20, 2025 | Published: November 28, 2025
Citation: Chipalo K, Noudjoutoubaye Moun-goss, Mahamat L Achair, Lakdim H, Zerrari O, Abid H, Mohammed El Idrissi, Abdelmajid El Mrini., (2025) “Neglected Posterior Elbow Dislocations Treated by Open Reduction (About 2 Cases)” Aditum Journal of Clinical and Biomedical Research, 7(1); DOI: 10.61148/2993-9968/AJCBR/118.
Copyright: ©2025. Kabwe Chipalo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Neglected posterior elbow dislocation is an uncommon but disabling condition, particularly in developing countries where delayed presentation is frequent. We report two young adult patients with neglected posterior elbow dislocations managed surgically by different approaches. In the first case, reduction was facilitated by enlarging osteoplasty of the trochlear notch, while in the second case, a triceps V–Y plasty was performed to overcome soft tissue contracture. Both procedures were performed via a posterior approach with careful protection of the ulnar nerve. Stable reduction and satisfactory functional recovery were achieved in both patients. These cases illustrate the therapeutic challenges of neglected elbow dislocations and emphasize the need to adapt surgical techniques according to intraoperative findings. They also highlight the importance of early diagnosis and appropriate management to prevent chronic stiffness and disability.
neglected elbow dislocation, open reduction, triceps V–Y plasty, osteoplasty, case series
Elbow dislocation is the second most common large joint dislocation in adults, after the shoulder [1]. When untreated for more than three weeks, it is considered neglected [2]. This condition is more frequently encountered in developing countries due to reliance on traditional bonesetters and limited access to specialized care [3,4]. Patients usually present with painful stiffness, functional disability, and soft tissue contractures that complicate management [3,6,11].
Closed reduction is generally unsuccessful in neglected dislocations and risks iatrogenic fracture [2,6]. Therefore, surgical intervention is required to restore stability and mobility. Several operative techniques have been described, including triceps lengthening, osteoplasty, and hinged external fixation [5,7–9,12]. The goal is to restore a stable, functional, and pain-free joint [4,10,13].
We report two cases of neglected posterior elbow dislocation managed by different surgical techniques: enlarging osteoplasty of the trochlear notch in one patient and triceps V–Y plasty in the other.
Methods
We conducted a case series of two young adult patients presenting with neglected posterior elbow dislocation. Both underwent surgical treatment under general anesthesia using a posterior approach. In the first case, reduction was achieved after enlarging osteoplasty of the trochlear notch, as described by Essi et al. [5]. In the second case, a triceps V–Y plasty was performed to allow sufficient length for reduction [7,8]. In both cases, the ulnar nerve was identified and protected. Postoperative care included brief immobilization in a posterior splint followed by progressive physiotherapy [9,10,19,20].
Case 1
A 30 year old man came to our Emergency trauma department with a history of trauma to his left elbow 5 months prior after falling on an outstretched hand from an olive tree. Being from a rural area, he was treated by a local bone setter who massaged and immobilised his elbow in extension for 1 month. When he presented to the Emergency trauma departement, the clinical exam revealed a stiff, tender and deformed elbow. The 3 point hueter triangle was altered and the elbow was in a non functional position, with a range of motion of 15° (Extension 45°, Flexion 60°). Pronation was 15° and supination limited to 10°, the ulnar nerve exam revealed no signs of motorsensoriel deficit and the vascular exam was normal.
An X-ray of the elbow with AP and lateral views as seen in Figure 1 revealed a posterior dislocation of the elbow with heterotopic ossifications. The patient was hospitalised and pre-operative bloodwork was done in preparation for a surgical reduction.

Figure 1: posterior elbow dislocation with osteophytes in the olecranon fossa and trochlear notch
The patient was placed in a lateral recumbent position with the elbow placed on a support. A midline paratricipital posterior approach was used. The ulnar nerve was isolated, the elbow joint was approached from lateral and medial sides with triceps sparing. The olecranon fossa, radial head and trochlear notch contained fibrous tissues and osteophytes which were removed, arthrolysis was then performed. Reduction was obtained but the humeral trochlea could not be lodged perfectly into the trochlear notch. We proceeded to perform an enlarging osteoplasty of the trochlear notch by performing an osteotomy at the base of the olecranon. Two 1.8mm K wires were then passed through the olecranon and the two fragments were distracted by 2mm in order to enlarge the trochlear notch. We then passed a cerclage wire in a figure of 8 loop and filled the defect created by our osteotomy with some of the periarticular fragments we had earlier resected. The elbow joint was then perfectly reduced, peroperative mobilisation of the elbow joint showed a range of motion of 115°(Extension 15°,Flexion 130°). The ulnar nerve was then transposed anteriorly and the elbow joint was stabilised in 90° flexion by an olecrano-humeral K wire. The lateral collateral ligament which was found to have been sectioned was reattached by transosseous sutures, the medial collateral ligament was intact but retracted and was released in order to reduce the joint, we did not need to perform a triceps lengthening procedure in order to achieve reduction. The wound was then washed with saline solution and closed and a posterior above elbow slab was applied. At 3 weeks post operatively the slab and the K wire blocking the elbow joint were removed and the patient was advised to begin physiotherapy.(Figure 2)

Figure 2: Post operative X ray showing a congruent elbow joint
At 6 months post operatively the elbow joint was stable with normal prono supination and a range of motion of 80° (Extension 30°, Flexion 110°)(Figure 3).

Figure 3: X ray at 6months post op revealing a congruent elbow joint
The Mayo elbow performance score was calculated at 80 points which translates to a good functional result.(Figure 4)

Figure 4: Functional result at 6months
Case 2
A 35 year old woman came to our Emergency trauma department with a history of trauma to her left elbow 6 weeks prior after falling on an outstretched hand. She consulted a local hospital after 4 weeks where a reduction under sedation was unsucccesfuly attempted. She was then referred to our structure for further treatment. Her clinical exam revealed a stiff, tender and deformed elbow. The 3 point hueter triangle was altered and the elbow was in a non functional position, with a range of motion of 20°(Extension 40°, Flexion 60°). Pronation and supination movements were 20°, the ulnar nerve exam revealed no signs of motorsensoriel deficit and the vascular exam was normal.
An X-ray of the elbow with AP and lateral views as shown in Figure 5 revealed a posterolateral dislocation of the elbow. The patient was hospitalised and pre-operative bloodwork was done in preparation for a surgical reduction.
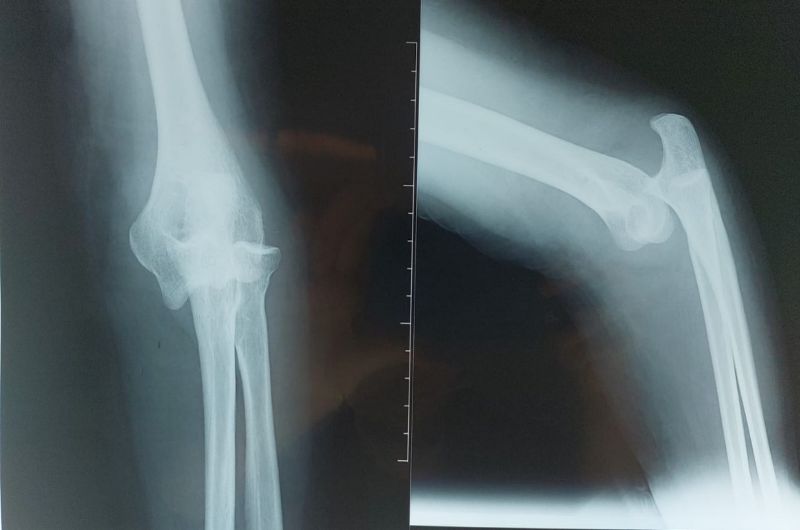
Figure 5: Posterolateral dislocation of the elbow joint
The patient was placed in a lateral recumbent position with the elbow placed on a support. A midline paratricipital posterior approach was used. The ulnar nerve was isolated, the elbow joint was approached from lateral and medial sides with triceps sparing. The olecranon fossa and trochlear notch contained fibrous tissues which were removed, arthrolysis was performed and the articular surfaces presented no irregularities. We then performed a triceps lengthening V-Y plasty which allowed us to achieve a congruent reduction of the articulation. We then used an olecrano-humeral K-wire to maintain stability in a 90° flexion position and proceeded to transpose the ulnar nerve anteriorly. The wound was then closed over a suction drain and the limb was immobilised for 15 days post operatively with a posterior slab. Passive mobilisation was started at 15 days after the removal of the K-wire.(Figure 6)

Figure 6: Post op X ray showing congruent elbow joint stabilised by a K wire
At 6 months post operatively the elbow joint was stable with normal prono supination and a range of motion of 90° (Extension 20°, Flexion 110°)(Figure 7). The Mayo elbow performance score was calculated at 85 points which translates to a good functional result.
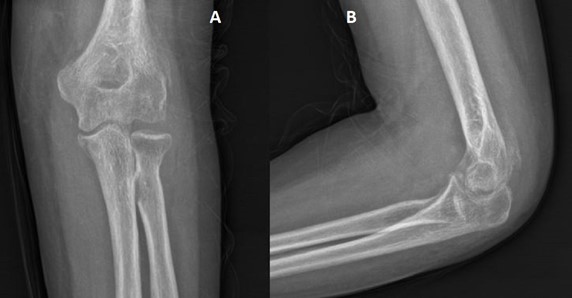
Figure 7: X ray at 6months showing a congruent elbow join.
Results
Both patients achieved stable reduction and regained functional mobility of the elbow. At final follow-up, each patient reported pain-free use of the limb and satisfactory performance of daily activities. No neurological complications were observed, and radiographs confirmed maintained reduction and joint congruity [4,6,12,14].
Discussion
Neglected elbow dislocations remain a therapeutic challenge, especially in settings where patients present late [3,4,6,11]. Closed reduction is rarely successful, and open surgical management is required [2,6]. The primary goals are restoration of stability, congruity, and mobility sufficient for daily activities [4,10].
Several techniques have been described. Speed [7] and Campbell [8] proposed posterior approaches with triceps V–Y plasty, providing good exposure and reducing tension during reduction. Naidoo [6] emphasized the importance of open reduction, as closed attempts carry risks. Essi et al. [5] described enlarging osteoplasty of the trochlear notch, useful when chronic remodeling prevents smooth reduction. Jupiter and Ring [9] advocated hinged external fixation for stability and early mobilization, but this technique is not always feasible in low-resource contexts. Other studies have reported favorable outcomes with open reduction and ligamentous repair in neglected cases [15–17,19,20].
Our two cases demonstrate that both triceps V–Y plasty and osteoplasty of the trochlear notch are effective options for neglected elbow dislocations. Both allowed stable reductions with functional outcomes, supporting the idea that tailored approaches are needed depending on intraoperative findings.
Limitations This study is limited by the small number of cases and relatively short follow-up. Functional outcomes were not assessed using standardized scoring systems, which restricts comparison with larger series [6,11,20].
Conclusion
Neglected posterior elbow dislocation is a surgically demanding condition that can be successfully managed with tailored techniques. Osteoplasty of the trochlear notch and triceps V–Y plasty are practical options in resource-limited settings. This case series highlights the importance of adapting surgical strategy to intraoperative findings and emphasizes early recognition to prevent long-term disability.
What is already known on this topic
- Neglected elbow dislocations are difficult to treat and usually require open surgery [2,6].
- Various surgical techniques, including triceps plasty and external fixation, have been described [5,7–9].
- Outcomes depend on chronicity, tissue contracture, and surgical approach [3,4,10].
What this study adds
- Demonstrates the effectiveness of enlarging osteoplasty of the trochlear notch in an adult patient [5].
- Confirms triceps V–Y plasty as a reliable method to facilitate reduction in chronic cases [7,8].
- Highlights that tailored techniques can achieve satisfactory results in resource-limited settings [19,20].
Competing interests
The authors declare no competing interests.
Authors' contributions
Kabwe Chipalo and Noudjoutoubaye Moun-goss were responsible for patient management, data collection and drafting the original manuscript. Mahamat Achair Langaba, Hamza Lakdim, Omar Zerrari, Hatim Abid, Mohammed El Idrissi and Abdelmajid El Mrini were responsible for editing and reviewing the manuscript. All the authors have read and approved the final version of the manuscript.
Acknowledgements
The authors would like to thank the patients and their families for consenting to the publication of these cases. We also acknowledge the contribution of the orthopaedic nursing and physiotherapy teams at the Hassan II University Teaching Hospital for their dedicated care and rehabilitation support.





Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org