OPEN ACCESS | Volume - Issue -
ISSN No: | Journal DOI:


Shilpa Jasubhai,
Consultant Clinical Psychologist, Ahmedabad, Gujarat, India
Corresponding Author: Shilpa Jasubhai, Consultant Clinical Psychologist, Ahmedabad, Gujarat, India
Received: March 19, 2021
Accepted: March 20, 2021
Published: March 24, 2021
Citation: Shilpa Jasubhai. “Efficacy of Emotional Freedom Technique and Cognitive Behavioural Therapy on Stress, Anxiety, Depression, Short-Term Memory, Psychophysiological coherence and Heart Rate in Indian Adults”. Clinical Psychology and Mental Health Care, 2(4); DOI: http;//doi.org/03.2021/1.10025.
Copyright: © 2021 Shilpa Jasubhai. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
World Health Organization reported depression as the fourth leading cause of mental illness worldwide and one of the leading causes of disabilities among adults. Living with depression may cause sleep deprivation, anxiety, stress and short-term memory loss. This is because the individual’s mind may be occupied with negative thoughts. Depression affects a person’s feelings, thinking, daily functioning, processing speed, memory, and executive functions. National Mental Health Survey of India in 2015-2016 reports that one in 20 Indians suffers from Depression. Earlier research indicated that Cognitive Behavioural Therapy (CBT) represents a superior approach in treating mild to severe depression symptoms, and Emotional Freedom Technique (EFT) received increased attention. The present study is in line with a study conducted in Australia in 2016 by Hannah Chatwin et al. The objective of the current study is to evaluate the efficacy of EFT and CBT in the treatment of stress, anxiety and depression, short-term memory loss, psychophysiological coherence and heart rate in Indian young adults. Subjects (n = 14), selected at random, from Ahmedabad (a metro city) in India, were screened for stress, anxiety and depression using Depression, Anxiety and Stress scale (DASS21) and Beck Depression Inventory (BDI2). They were also screened for short term memory using Digit Span test, which allowed assessments of each participant’s initial complaints of forgetfulness, difficulty in concentrating and confusion. Their psychophysiological coherence score and heart rate were recorded pre- and post- interventions using emWave system. These subjects were randomly assigned to an 8 once a week CBT or EFT treatment program. All participants were screened after 3 sessions, 5 sessions, 8 sessions and 6 months of follow up using DASS21, BDI2 and Digit Span Test. They were also screened after 1 month for stress, anxiety and depression using DASS21 and BDI2. Findings of the study depicted that both intervention approaches produced significant reductions in stress, anxiety and depressive symptoms and concurrent improvement in short-term memory (STM), psychophysiological coherence and heart rate. The EFT treatment produced marked improvement in depression after 3 sessions. After 8 weeks of intervention, the CBT group reported significant improvement in depression and short-term memory, while EFT intervention therapy showed significant improvement in depression state after 1 month and 6 months of follow up respectively. Examination of individual cases showed, clinically significant improvement in stress, anxiety, depression symptoms, short-term memory and psychophysiological coherence across both interventions. The results are consistent with the previous studies by Hannah Chatwin et al. (2016). Present findings suggest that EFT would be an effective intervention therapy in managing stress, anxiety, depression and STM and worthy of further investigation.
Introduction:
Uncontrolled depression and anxiety cause significant impairment in daily functioning, processing speed, memory, and executive function. Depression and long-term anxiety are known to be associated with confusion, forgetfulness or lack of concentration [81]. World Health Organization (2020) reported that depression is the leading cause of disability worldwide affecting women more than men [86]. and 7.5% Indians suffer from major to minor mental illness [55]. The National Institute of Mental health and Neuroscience of India reported in a survey in 2016 that every 6th person needs mental health help and 1 in 20 suffers from depression [68,85]. When a person is in stress, stress hormones are secreted in the brain and the amygdala and other cerebral parts of the brain are activated. Lack of coping mechanism can lead to physical and psychological consequences and can be long-lasting, causing anxiety and depression [65].
The irony of mental health in India was reported by a survey done in 2019 that there is still a stigma attached to mental illnesses. Even educated people are loosely using term ‘Paagal’ with depressed individuals [70]. Women primarily are less likely to receive any help or are discouraged to seek help.
A pilot study on “Effectiveness of Cognitive Behavioural Therapy (CBT) and Emotional Freedom Technique (EFT) in reducing Depression and Anxiety among Adults” was conducted by Hannah Chatwin et al. in 2016 in Australia. The results revealed clinically significant improvement in anxiety and depression with both interventions. While CBT group reported a significant reduction in depression post-intervention, which was not maintained with time, the EFT group reported a delayed effect with a significant reduction in symptoms after 3- and 6-months of follow-ups. The individual cases revealed clinically significant improvements in anxiety across both interventions [39]. After the literature review, no past studies were found in line with Hannah Chatwin et al study comparing CBT and EFT in reducing stress, anxiety and depression in Indian population.
Literature Review
Ali H. Kizilbash, Rodney D. Vanderploeg, Glenn Curtissa (2002), in a study on “The effects of depression and anxiety on memory performance” reported that depression with comorbid anxiety had an adverse effect on immediate recall, amount of acquisition and on the retrieval of newly learned information [1]. Dotson VM, Szymkowicz SM, Kirton JW, McLaren ME, Green ML, et al. (2014) in study reported that depression and anxiety influence cognitive and brain functioning [28]. A study by Louisa Burriss et al (2008) showed positive association between PTSD and general learning and memory impairment [54]. Katherine E. et al (2013), in a study reported that anxiety disrupts both verbal and spatial working memory [51]. Gary Christopher & John MacDonald (2005), in a study on “The impact of clinical depression on working memory” reported that depression affects attention and working memory [38].
Benor et al (2009) conducted a study on effectiveness of CBT and EFT in comparison with the treatment of test anxiety among university students and concluded that WHEE (Wholistic Hybrid Derived from Eye Movement Desensitization and Reprocessing) and EFT showed significant effects in only 2 sessions as compared to 5 sessions needed by the CBT [31]. Gaesser Amy H. & Karan Orv C. (2016) in a pilot study on EFT and CBT to Reduce adolescent anxiety, concluded that EFT is an effective intervention technique to significantly reduce anxiety for high-ability adolescents [36]. Zhang Y, Feng B, Xie JP, Xu FZ, Chen J. (2011) conducted a comparative study on treatment of the PTSD using CBT and acupoint stimulation. Results showed a significantly stronger improvement in CBT with acupoint stimulation [87].
Conal Twomey, Gary O’Reilly & Michael Byrne (2014) and Hofmann S., Asnaani A, Vonk IJ., Sawyer A. and Fang A. (2012) in their research on, effectiveness of CBT for anxiety and depression, concluded multi-modal CBT is effective for anxiety and depression symptoms in primary care and the evidence base of CBT in general is very strong [22,44]. Ragnhild S. H. et al. (2011) conducted a research on effectiveness of CBT on depression and anxiety in primary health care unit and concluded that CBT is potentially more effective for mild to moderate depression and anxiety than usual care [69]. Saeid Pahlavanzadeh, Samira Abbasi, and Nasrollah Alimohammadi (2017), conducted a study on “The Effect of Group CBT on Stress, Anxiety, and Depression of Women with Multiple Sclerosis” and found significant improvement in stress, anxiety and depression after 8 weeks and 1 month [76].
Church et al (2010, 2012 & 2013) conducted various studies to confirm the efficacy of EFT in bringing significant reductions in the symptoms of depression and anxiety. They concluded that Clinical EFT is an evidence based, stable, safe and reliable treatment for psychological and medical diagnosis in primary care settings [17,18,20]. Church et al (2012) in a study “The Effect of Emotional Freedom Techniques on Stress Biochemistry” observed significant improvement in psychological distress and decrease in the cortisol level in one session in the EFT group [19]. Clond M (2016), Church et al (2012) conducted various studies on efficacy of EFT in decreasing symptoms of stress, anxiety and depression. Their conclusions were similar and all of them reported improvement in symptoms, positive health effects and increased mental well-being [21,18]. Donna Bach et al (2019), in a study on “Clinical EFT (Emotional Freedom Techniques) Improves Multiple Physiological Markers of Health”, reported that a positive trend was observed for HRV (heart rate variability), HC (heart coherence) and EFT. EFT combines both cognitive and somatic elements and is effective for both physiological and psychological symptoms [27]. Feinstein, D. (2012) in paper on acupoint stimulation in treating psychological disorders got positive result in few treatments of EFT [32]. In a study on Efficacy of EFT in reducing public speaking anxiety, Jones, S., Thornton, J., & Andrews, H. (2011) concluded that the EFT treatment group showed statistically significant decrease in anxiety. [46]. Kalla Mahima et al (2017) in a study to find out the experience of an EFT practitioner in using EFT technique to support patients with chronic disease, concluded that EFT technique can give promising results to health care practitioners for the psychosocial aspect of chronic disease [48]. Karatzias et al. (2011) investigated the effect of EFT on PTSD and the results showed a positive outcome with voluntary termination of the treatment after an average of 3.8 sessions [49]. Patterson SL. (2016) conducted a pilot study on the effect of stress and anxiety in nursing students” and concluded that EFT can be an effective tool in managing stress and reducing anxiety in nursing students [63]. Meta-analysis of the past studies by Brenda Sebastian & Jerrod Nelms (2016) showed that 4-10 session of EFT was an effective treatment for PTSD [14]. Peta Stapleton et al. (2014) investigated the feasibility of using Clinical Emotional Freedom Techniques to treat Major Depressive Disorder in an Australian adult and positive results were found after eight weeks of therapy [64]. Rowe, J. (2005) in a study on ‘The effects of EFT on long-term psychological Symptoms’ using EFT and got promising results with significant decrease in psychological distress post workshop and after 1-month and 6-months of follow up [72].
Hartmann Ralf et al (2019) conducted a study on heartrate variability as an indicator of clinical state in depression and concluded that change in HRV parameter values correlated with changes in the severity of depressive symptoms [40]. S.D. Edwards (2016) investigated the influence of HeartMath quick coherence technique on psychophysiological coherence and feeling states and reported a significant change in percentages of high psychophysiological coherence, decreased feelings of sadness and increased feelings of peacefulness [74]. A study conducted by Dan Malm et al. (2018), concluded that a mindfulness-based CBT programme improved the health-related quality of life and sense of coherence and reduced psychological distress up to 12 months post atrial fibrillation [26].
However, there was not enough data available to compare EFT to conventional treatment i.e. CBT for stress, anxiety, depression, short-term memory, psychophysiological coherence and heart rate in the Indian population. Further research is needed to establish the relative effectiveness of EFT in the Indian context.
Present Study
The author chose to evaluate the efficacy of CBT and EFT on stress, anxiety, depression, short-term memory and psychophysiological coherence in Indian adults. Present study is based on of her past research in 2018.
The participants were randomly selected and assessed for stress, anxiety and depression. Participants who were screened positive for stress, anxiety and depression were included in the present study and further assessed for short-term memory loss and their physiological coherence and heart rate were recorded. In the initial interview most, participants complained of forgetting names, misplacing things, forgetting specific words and difficulty concentrating. According to past research findings, stress, anxiety or depression could cause forgetfulness, confusion, difficulty in concentration and other problems that disrupt daily mental activities [56]. According to HeartMath research different patterns of heart activity have discrete effects on emotional and cognitive function. The heart rhythm pattern is erratic during stress and anxiety and affects the brain’s emotional processes [29]. The subjects were randomly assigned to an 8 once a week CBT or EFT treatment program. All participants were screened after 3 sessions, 5 sessions, 8 sessions and 6 months of follow up using DASS21, BDI2 and Digit Span Test. They were also screened after 1 month for stress, anxiety and depression using DASS21 and BDI2. Their physiological coherence score and heart rate were recorded pre- and post-interventions using emWave system. The corresponding author has been using the EFT therapy regularly to help clients with a variety of problems like depression, anxiety, OCD, stress, etc. Thus, the author chose to evaluate the effectiveness of CBT and EFT on stress, anxiety, depression, short-term memory, psychophysiological coherence and heart rate in Indian adults.
Stress:
The dictionary meaning of stress is “a state of mental or emotional strain or tension resulting from adverse or demanding circumstances.” [62]. In psychology, stress is a feeling of strain, pressure or a type of psychological pain [81].
Baum, A. (1990) defined stress as any uncomfortable "emotional experience accompanied by predictable biochemical, physiological and behavioral changes [6]. Research by Baum, A. & Polsusnzy, D. (1999), shows that stress can contribute to the development of serious health issues, such as heart disease, depression, obesity, anxiety, insomnia, muscle pain, high blood pressure and a weakened immune system [7]. External stress or internal perceptions can cause an individual to experience anxiety or other negative emotions surrounding a situation, which they believe is stressful [34].
Anxiety:
The dictionary meaning of anxiety is “a feeling of worry, nervousness, or unease about something with an uncertain outcome.” [60]. According to the American Psychological Association (APA) “Anxiety is an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure. People with anxiety disorders usually have recurring intrusive thoughts or concerns. They may avoid certain situations out of worry. They may also have physical symptoms such as sweating, trembling, dizziness or rapid heartbeat.” [2].
The essential features of generalized anxiety disorder according to DSM V are “excessive anxiety and worry about a variety of topics, events, or activities. Worry occurs often for at least 6 months and is clearly excessive. Excessive worry means worrying even when there is nothing wrong or in a manner that is disproportionate to the actual risk” [4].
Depression:
Dictionary meaning of depression is “feeling of severe despondency and dejection.” [61]. According to APA “Depression is more than just sadness. People with depression may experience a lack of interest and pleasure in daily activities, significant weight loss or gain, insomnia or excessive sleeping, lack of energy, inability to concentrate, feelings of worthlessness or excessive guilt and recurrent thoughts of death or suicide.” [3].
According to DSM V Depression symptoms can vary from mild to severe and a person may experience feeling of sadness, loss of interest, changes in appetite, change in sleep, loss of energy, feeling of worthlessness, suicidal thoughts, difficulty concentrating and the symptoms should last for at least two weeks [4].
Short Term Memory:
Short-term memory is the capacity for holding a small amount of information in mind for a short period of time. Short-term memory (STM) is the second stage of the multi-store memory model proposed by Atkinson and Shiffrin [57]. According to Atkinson and Shiffrin (1971) the duration of STM is between 15-30 seconds [5]. According to the Miller’s Law (1956) the number of objects an average human can hold in short-term memory is 7 ± 2 [59].
According to past research findings, stress, anxiety or depression could cause forgetfulness, confusion, difficulty in concentration and other problems that disrupt daily mental activities. (56) S. Nolen-Hoeksema et.al, concluded that a person with depressed mood spends more time on processing negative or depressive information than other forms of information which may affect cognitive functioning and working memory [75].
Psychophysiological Coherence
Doc Childre (1991) is the founder of the HeartMath Institute. Heart rate variability (HRV) is a measure of the beat-to-beat changes in heart rate. The HRV helps to understand the interactions between physiological, mental, emotional and behavioural processes. According to HRV analysis the heart is a sensitive marker for emotional changes, which is reflected in heart rhythm patterns. It reflects a person’s capacity to adapt effectively to stress and environmental demands and is an important indicator of both physiological resilience and behavioural flexibility. Different patterns of heart activity have different effects on cognitive and emotional function of the brain. During stress, anxiety or negative emotions, the heart rhythm pattern is irregular and erratic. HeartMath scientists call this an incoherent heart rhythm pattern. This restricts the ability to think clearly, remember, learn and it affects emotions. When positive emotions are experienced the heart rhythm pattern becomes smooth and harmonious called coherent heart rhythm pattern. According to Rollin McCart, coherence is an optimal physiological state when the heart, mind and emotions are in alignment and which prevents and reduces stress, increases resilience and improves emotional wellbeing. This is called psychophysiological coherence because there is an increased harmony in both the psychological and physiological processes. [29,40,41,54,71].
EFT:
The basic EFT technique was developed in 1995 by Craig and Fowlie as a simplified form of thought field therapy (Callahan, 1985). He described the unique feature of EFT in one statement, “The cause of all negative emotions is a disruption in body’s energy system.” EFT is a blend of Acupuncture and Mind-Body Medicine, both of which have been supported by scientific studies for decades [23].
In simple words EFT is an alternative therapy for emotional distress and physical pain. EFT is the most well-known form of “energy psychology” which combines cognitive and exposure techniques by stimulating the selected acupuncture points (acupoints) by tapping on them. It works by gently tapping on the acupoints while focusing on emotional trigger and repeating a statement of self-acceptance [23,33,47]. This helps in releasing blockages within the energy system which causes negative emotions and physical disorders. These blockages in our energy system cause limiting beliefs and behaviours, various physical, emotional and psychological syndromes, such as low confidence, stress, anxiety or depression [83].
A cognitive approach with acupuncture leads to a change in the behaviour, subconscious thought process and neurochemical bases of the psychological problem. Stimulation of these meridian points is believed to send signals to the limbic system, decrease the activity in amygdala and balance the secretion of stress hormones. Like CBT, EFT thrives on the fact that rather than resistance of a condition, self-acceptance will reduce the suffering [47]. EFT seems to balance disturbances in the meridian system which in turn balances the negative emotions and the physical discomfort attached to it at conscious and sub-conscious level. Thus, EFT reduces the time spent by conventional therapy procedures [23].
The American Psychological Association (APA) in a review in 2012, stated that EFT therapy met the criteria for evidenced-based treatments, but the mechanisms behind EFT are not understood [73].
CBT
Aaron Beck (1960) is considered the father of CBT and his theories are widely used in treating depression and anxiety [10]. Beck Institute states CBT as a time-sensitive, structured, present-oriented psychotherapy directed toward solving current problems and teaching skills to modify dysfunctional thinking and behaviour [66]. Based on the CBT concept, CBT helps an individual to understand the connection between thoughts, feelings and behaviour, and teaches the effective coping strategies for dealing with different problems throughout life [16].
According to the National Health Service (NHS) of England, “CBT is based on the concept that your thoughts, feelings and behaviour are interconnected, and constantly influence one another.” CBT deals with current problems, rather than focusing on past issues [67]. This is another common factor between EFT and CBT.
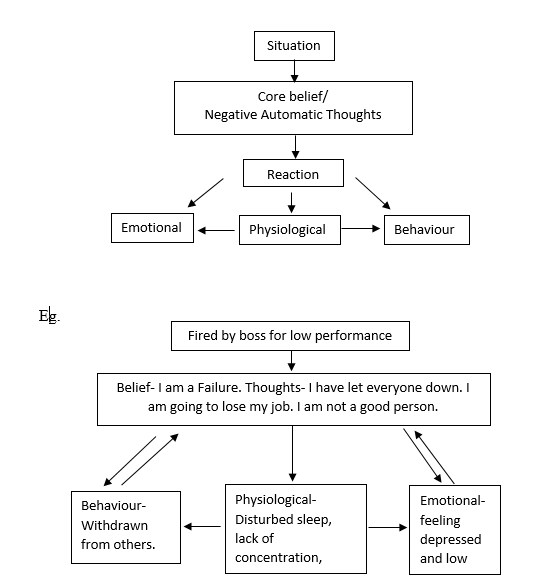
The cognitive Model [12].
Our pattern of thinking makes us perceive the world in a specific way. According to Aaron Beck the perceptions and interpretations of depressed persons are distorted. Depressed individuals are occupied in "cognitive errors," (50) such as negative and fearful thoughts and biased information processing. (69) These errors in thoughts are automatic and the individual believes them to be true. CBT focuses on altering these automatic thoughts. In simple words CBT is a focused, short term and structured method to treat a variety of mental health disorders. (33)
Hypothesis:
Material:
Method:
Participants:
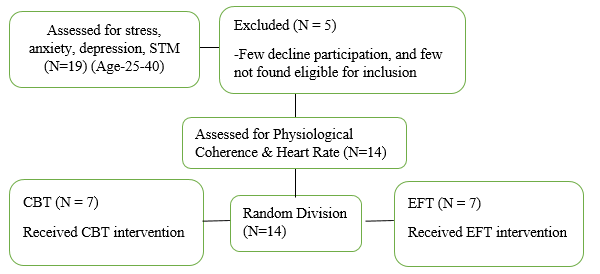
19 participants in the age group of 25 to 40 years were randomly selected from general population in Ahmedabad, India and were screened for stress, anxiety, depression, short-term memory and their psychophysiological coherence scores were recorded using Beck Depression Inventory - second edition (BDI-II) (8), Depression, Anxiety, Stress Scales 21 (DASS-21) (53), Digit Span Test (45) and emWave Pro system respectively [29].
Due to personal reasons some of the participants dropped out and few were not eligible for inclusion. Ahmedabad being a conservative city there is a stigma attached to seeing a psychologist. Male don’t volunteer for research work so easily, especially when a researcher is a female. Thus, there was a difference in the gender equality.
BDI II (Aaron Beck, 1996) is a revised version of BDI is designed for individuals aged 13 and over. Based on DSM 5 it measures the severity of depressive symptoms such as hopelessness and irritability, feeling of guilt or feelings of being punished, as well as physical symptoms such as fatigue, weight loss, and lack of interest in sex. BDI II contains 21 questions. Participants were asked to specify on a 4-point Likert scale the extent to which they had experienced negative emotional states of depression during the past week [10].
The DASS 21 scale (Lovibond, S.H. & Lovibond, P.F., 1995) is a set of three self-report scales designed to measure the negative emotional states of depression, anxiety and stress. ‘Participants were asked to specify on a 4-point scale the extent to which they had experienced negative emotional states of depression, anxiety, and stress during the past week. Each of the three DASS-21 scales contains 7 items, divided into subscales with similar content. The development of DASS-21 was based on the assumption that difference between the stress, anxiety and depression experienced by normal subjects and clinical patients is mainly of degree [53].
Digit span was originally devised by Jacobs (1887). Short term memory span has been measured through the recall of digit sequences. The span indicates an ability to retain meaningless material that appears to be unrelated to thinking [45]. Digit-span task measures working-memory's number storage capacity. Participants are presented with a series of digits (e.g., '8, 3, 4') and must immediately repeat them. The longest list of numbers a person can remember is that person's digit span. The participants were asked to repeat the digits in the given order in the forward digit-span task and in the backward digit-span task the participant had to reverse the order of the numbers [80].
EmWave system was developed by Doc Childre in 1991. Emwave system accurately records the heart rhythms and heart rate variability and translates coherence information into graphical display on the computer screen. The ear sensor was attached to the earlobe of each participant. The ear sensor detects the pulse easily. They were asked to keep their eyes closed and not to move or talk while the recording was going on. The recording was done for 4 minutes. The psychophysiological coherence score and heart rate were recorded pre- and post- interventions. [29,77].
14 participants (10 female and 4 male) who were screened positive for stress, anxiety and depression were included for the study. They were asked to sign the consent form and provide demographic information. Then they were tested for short term memory using digit span and their psychophysiological coherence score and heart rate were recorded. The participants were then randomly assigned to 8 once a week EFT (N=7) or CBT (N=7) therapy program. They were screened for stress, anxiety and depression after 3 sessions, 5 sessions, 8 sessions, after 1 month and 6 months using DASS 21 and BDI II. Participants were screened for STM using digit span test post interventions and after 6 months. Their psychophysiological coherence score and heart rate were recorded pre- and post- interventions. The results were analysed using ‘t’ test.
Procedure:
Eight, once a week individual therapy session was conducted for both EFT and CBT programs by the researcher. A similar structure was used for both the interventions. Participants were contacted after 1 month and 6 months post intervention to complete the same questionnaires.
EFT Intervention:
The procedure involved participants to focus on a distressing thought, create an intensity rating, initiate a setup phrase, and then complete the tapping sequence using acupressure points. Psychological Reversal means energy in the body is disturbed. It is self-defeating, negative thinking which often occurs subconsciously and may be outside one’s awareness. It should be neutralized with affirmative statement for cognitive shift.
At the beginning of each session participants were asked to rate their subjective level of discomfort on the scale of 1 to 10. Then based on emotional difficulty being experienced a setup phrase was initiated. The affirmative statement of acceptance of the difficulty was repeated 3 times while tapping on "Karate Chop" point, as per Craig’s EFT manual. e.g. “Even though I have this Problem, I deeply and completely accept myself”. The sequence of tapping points- TH, EB, SE, UE UN, UL, CB, UA, Gamut procedure and WR was taught and the participants were asked to get tuned into emotional discomfort while tapping on the meridian point and repeating the affirmative statement. The whole cycle was repeated till the subjective level of discomfort reduced to zero level. After the 1st round the setup phrase was rephrased as, “Even though I still have some of this remaining problem. I deeply and completely accept myself”. [24].
At the end of each session, they were given home plan and asked to give feedback for the session. Home plan included tapping sequence, thought journal, affirmation statement and breathing exercise.
CBT Intervention:
The CBT session was conducted using conventional CBT program. The aim of the intervention was to modify distorted thinking, dysfunctional behaviour, and distressing feeling by teaching coping strategies. In simple words the goal was to replace negative thoughts with productive behaviour.
The CBT program involved identifying and challenging the harmful automatic thoughts, restructuring negative automatic thoughts, core beliefs and scheduling and monitoring activities. Participants were given different worksheets like Alternative Action Formulation, Functional Analysis and Longitudinal Formulation and were asked to maintain a thought journal as home plan. [66].
At the beginning of each session participants were asked to rate their subjective level of discomfort and describe their feelings of this week, compared to earlier weeks. They were, then, asked to name the main problems they faced during the week and the plan for the session was discussed. To create a bridge between the last and present session they were asked whether anything unusual happened during the week which they would like to share. This was followed by discussing self-help assignments. After prioritizing the issue, the problems were discussed one by one. The truthfulness of their thoughts and beliefs in the difficult situation were assessed. New skills to modify their negative thinking and behaviour and solving problems on their own were taught. They were asked to summarize and write down important points in their own words and home plan activities were scheduled until the next session. At the end of the session, they were asked to give a feedback for the session and were asked to rate their subjective level of discomfort. Home plan activities included affirmation statement, thought journal, breathing exercise and worksheets like Alternative Action Formulation, Functional Analysis and Longitudinal Formulation.
In each consecutive session at the beginning the home plan was reviewed for both the intervention therapies. After 8 weeks of intervention participants were asked to continue home plan activities.
Statistical Methods:
The statistical analysis was done using small samples t test and within subject t test. A statistical significance in t test indicates whether the difference between the averages of two groups most likely reflects a “real” difference in the population from which the groups were sampled. We are interested in finding out (i) changes in subjects’ scores before the treatment and after the treatment (ii) whether there was any significant difference between the two-intervention therapies (iii) whether there was an improvement in stress, anxiety, depression, memory, psychophysiological coherence and heart rate post intervention [37,79].
Results:
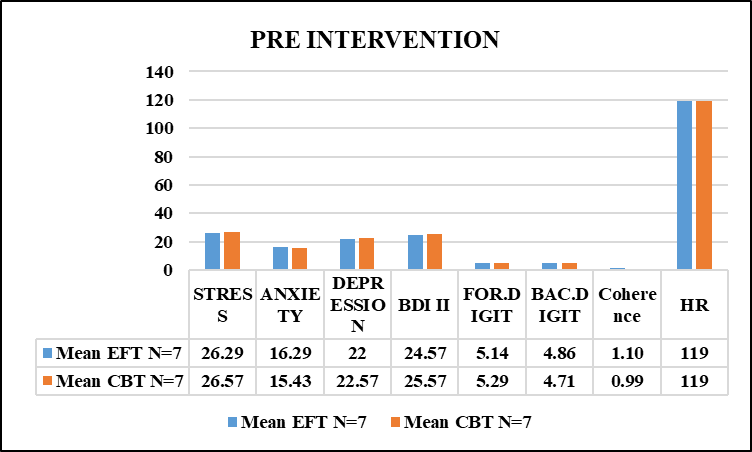
Graph 1 Pre-Intervention
The total sample size was 14, consisting of 1o women and 4 men between the age group of 25 – 40 years. Pre-test results show no statistically significant difference in both intervention groups. Average depression score in both the groups on BDI II scale was 24.57 (EFT) and 25.57 (CBT) respectively, which is in the moderate range and on DASS 21 scale was 22 (EFT) and 22.57 (CBT) respectively, which is in the severe range. Average anxiety score in both the groups was 16.29 (EFT) and 15.43 (CBT) respectively, which is in the severe range. Average stress score in both the groups was 26.29 (EFT) and 26.57 (CBT) respectively, which is in the moderate range. The forward digit span score in both the groups was 5.14 (EFT) and 5.29 (CBT) respectively. The backward digit span score in both the groups was 4.86 (EFT) and 4.71 (CBT) respectively. The psychophysiological coherence score in both the groups was 1.10 (EFT) and 0.99 (CBT) respectively and heart rate was 119 in both the groups.
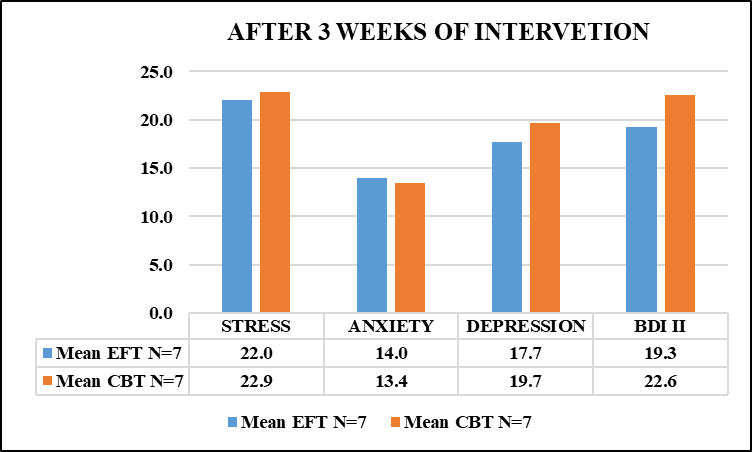
Graph 2 After 3 weeks of Intervention
After 3 sessions, average depression score in both the groups on BDI II scale was 22 (EFT) and 22.9 (CBT) respectively, and on DASS 21 scale was 14 (EFT) and 13.4 (CBT) respectively, which is in the moderate range. Average anxiety score in both the groups was 17.7 (EFT) and 19.7 (CBT) respectively, which is in the moderate range. Average stress score in both the groups was 14 (EFT) and 13.4 (CBT) respectively, which is in the moderate range. There was no significant difference found in reduction of stress, anxiety and depression between both intervention therapies after 3 weeks. 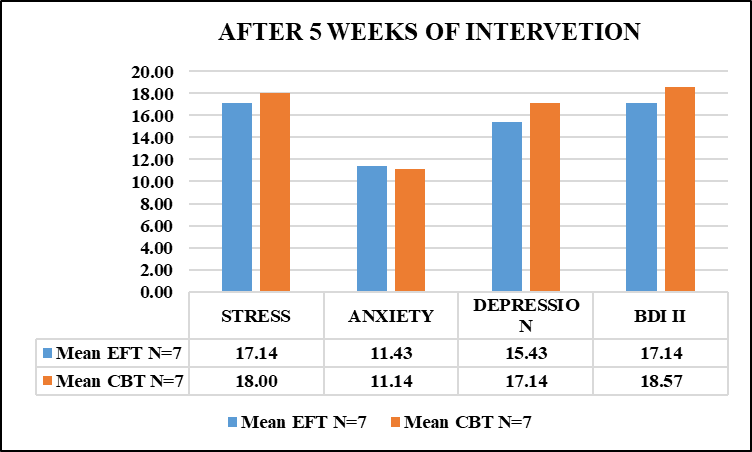 Graph 3 After 5 weeks of Intervention
Graph 3 After 5 weeks of Intervention
Average depression score after 5 sessions in both the groups on BDI II scale was 17.14 (EFT) and 18.57 (CBT) respectively, which is in the range of borderline clinical depression and on DASS 21 scale was 15.43 (EFT) and 17.14 (CBT) respectively, which is in the moderate range. Average anxiety score in both the groups was 11.43 (EFT) and 11.14 (CBT) respectively, which is in the moderate range. Average stress score in both the groups was 17.14 (EFT) and 18 (CBT) respectively, which is in the mild range. There was no significant difference found in reduction of stress, anxiety and depression between both intervention therapies after 5 weeks. 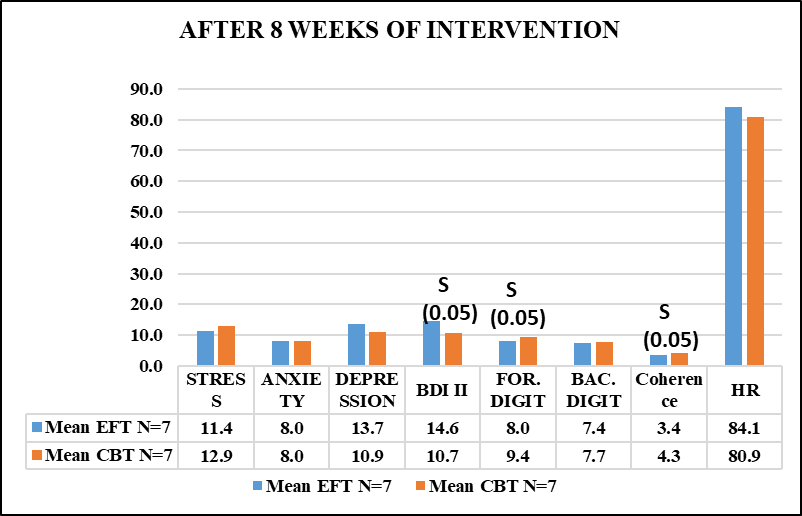
Graph 4 After 8 weeks of Intervention
Average depression score after 8 sessions on BDI II scale in both the groups was 14.6 (EFT) which is in the range of mild mood disturbance and 10.7 (CBT) which is in the normal range. The result is statistically significant at 0.05 level. Participants who received CBT therapy showed better results than participants who received EFT therapy. On DASS 21 scale average depression score was 13.7 (EFT) which is in the moderate range, and 10.9 (CBT) which is in the mild range. Average anxiety score in both the groups was 8.0, which is in the mild range. Average stress score in both the groups was 11.4 (EFT) and 12.9 (CBT), which is in the mild range. Average forward digit span score in both the groups was 8.0 (EFT) and 9.4 (CBT) respectively. The result is statistically significant at 0.05 level. Average backward digit span in both groups was 7.4 (EFT) and 7.7 (CBT) respectively. Average psychophysiological coherence score in both the groups was 3.4 (EFT) and 4.3 (CBT) respectively. The result is significant at 0.05 level. Average heart rate in both the groups was 84.1 and 80.9 respectively. There was a significant reduction in depression and improvement in forward digit span and psychophysiological coherence in CBT group post intervention. There was no significant difference found between two therapies in reduction of stress, anxiety, heart rate and improvement in backward digit span.
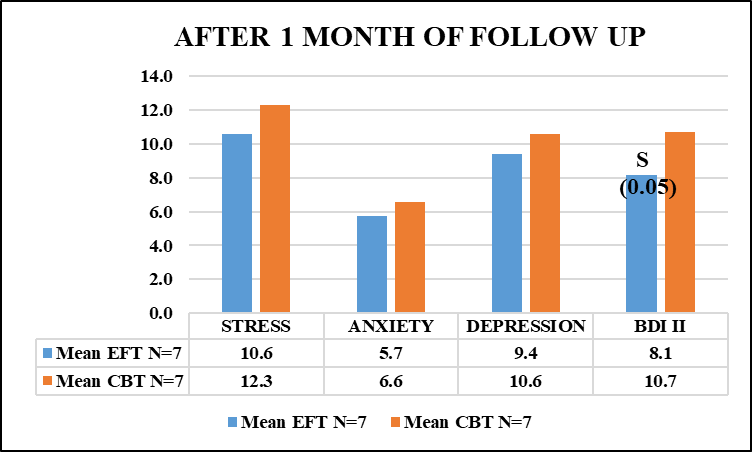
Graph 5 After 1 Month of Follow Up
Average depression score after 1 month of follow up in both the groups on BDI II scale was 8.1 (EFT) which is in the normal range and 10.7 (CBT) which in the range of mild mood disturbance. The result is significant at 0.05 level. On DASS 21 scale average depression score was 9.4 (EFT) which is in the normal range and 10.6 (CBT) which is in the mild depression range. Average anxiety score in both the groups was 5.7 (EFT) and 6.6 (CBT), which is in the normal range. Average stress score in both the groups was 10.6 (EFT) and 12.3 (CBT), which is in the mild range. Participant who had received EFT therapy showed significantly better result in reduction of depression on BDI II scale after 1 month of follow up. Both the groups were asked to continue the home plan.
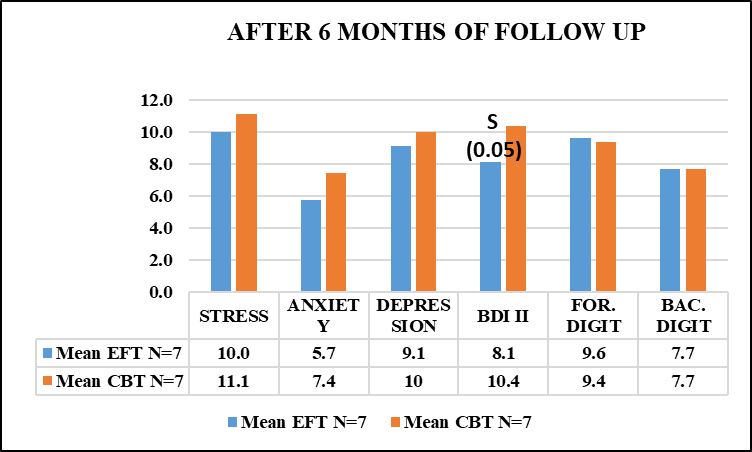
Graph 6 After 6 Month of Follow Up
Average depression score after 6 months of follow up in both the groups on BDI II scale was 8.1 (EFT) and 10.4 (CBT) which is in the normal range. The result is significant at 0.05 level. On DASS 21 scale it was 9.1 (EFT) which is in the normal range and 10 (CBT) which is in the mild depression range. Average anxiety score in both the groups was 5.7 (EFT) and 7.4 (CBT), which is in the normal range. Average stress score in both the groups was 10.0 (EFT) and 11.1 (CBT) which is also in the normal range. Average forward digit span score in both the groups was 9.7 (EFT) and 9.9 (CBT) respectively. Average backward digit span score in both groups was 7.7. After six months, the average scores on BDI II, DAS 21 and digit span remained more or less same across both the groups.
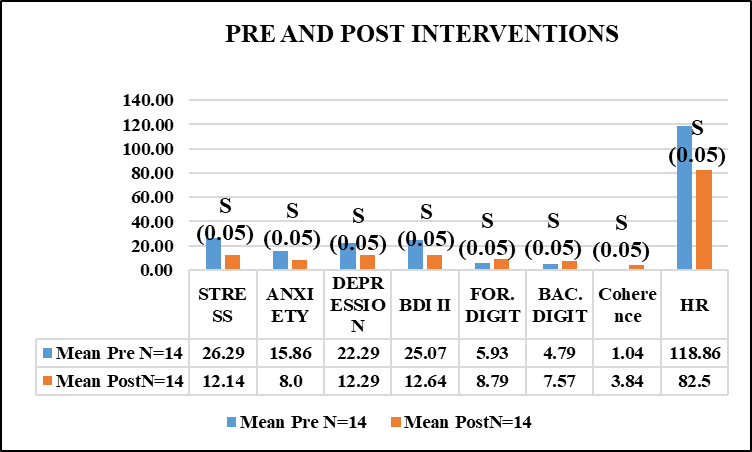
Graph 7 Pre and Post Intervention
There was a statistically significant improvement at 0.05 level in stress, anxiety, depression, forward digit span, backward digit span, psychophysiological coherence and heart rate post interventions in all the participants.
Discussion:
Observationally, after 3 weeks of intervention, there was a reduction in depression on BDI II scale in EFT group from moderate to borderline clinical depression. The result support the past studies by Benor et al. (2009) where EFT showed significant effects in only 2 sessions as compared to 5 sessions for the CBT and by Church et al (2012) where EFT showed a significant improvement in psychological distress and decrease in the cortisol level in one session. [13,19]
Observationally, after 5 sessions there was a reduction in stress, anxiety and depression across both the groups. The Results support the findings of Zhang Y et.al. where CBT with acupoint stimulation showed significantly stronger improvement [87].
One of the subjects who was 34 years old Female, had severe stress, anxiety and depression pre intervention, showed noticeable improvement with EFT intervention therapy after 5 weeks. Her stress score came down in the range of mild, anxiety score and depression score on DAS 21came down in the moderate range and on BDI II depression came down in the range of mild mood disturbance. Results support the study done by Benor et al (2009) where EFT showed significant effects in only 2 sessions as compared to 5 sessions needed by the CBT to reduce anxiety in university students [1]. The subject did not show much improvement after 8 sessions of EFT but after one month of follow up the subject became normal and the score across all the tests were in normal range i.e. < 10. Her scores on BDI II, DAS 21 and backward digit span remained same after 6 months of follow up. There was an improvement in forward digit span after 6 months of follow up compared to a score after 8 sessions. Her psychophysiological coherence was 1.2 and heart rate was 122 pre intervention. According to the HeartMath Institute our feelings and emotional stress affect our heart rhythm pattern and make it appear erratic and irregular. After the 8 sessions her psychophysiological coherence was 4.6 and heart rate was 92. Higher heart-coherence levels indicate positive emotional state which is reflected in the pattern of the heart’s rhythm. This shift in the heart rhythm plays an important role in promoting higher cognitive functions and emotional stability. The result supports the study done by Hartmann Ralf et al (2019) where he concluded that change in HRV parameter values correlated with changes in the severity of depressive symptoms [40, 41, 71]
E.g. Heart Rhythm pattern of the participant mentioned above.
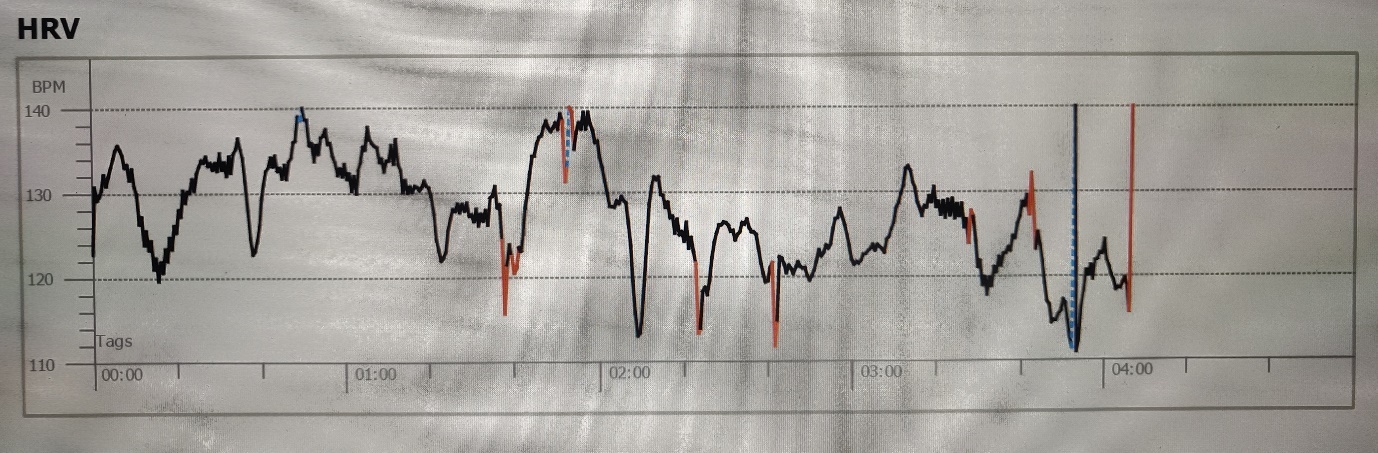
Pre-Intervention - Coherence-1.2 Heart rate-122
During stress, anxiety and negative emotions, the heart rhythm pattern is irregular and erratic. This restricts the ability to think clearly, remember or learn and it affects emotions [71].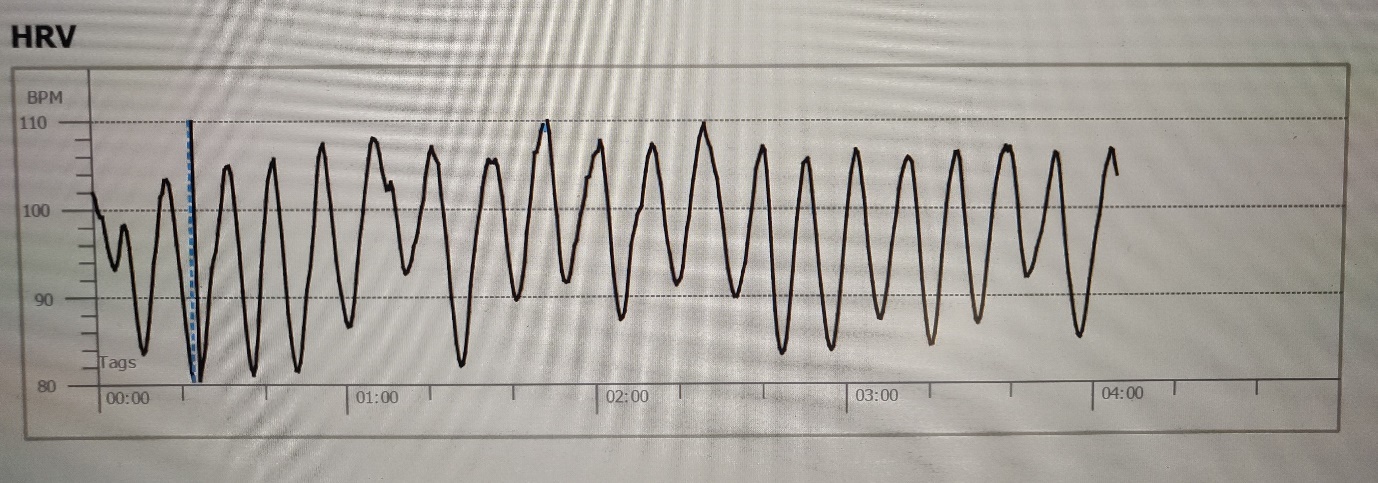 Post-Intervention - Coherence-4.6 Heart rate-92
Post-Intervention - Coherence-4.6 Heart rate-92
When the positive emotions are experienced the heart rhythm pattern becomes smooth and harmonious. This is called psychophysiological coherence state [71].
At 8 weeks, the CBT intervention group reported significant improvement in depression on BDI II scale, forward digit span and psychophysiological coherence. Depression score came down from borderline clinical depression to mild mood disturbance on BDI II scale and from moderate to mild depression on DASS 21 scale. Findings are highly consistent with prior studies like Hannah Chatwin et al. (39), Hofmann et al [44], Ragnhild S. H. et al [69], Conal T. et al [22] and Saeid Pahlavanzadeh et al [76] where they concluded that CBT is potentially more effective for mild to moderate depression and anxiety than the usual primary care treatment.
After 8 weeks of therapy the range of depression in EFT group came down from borderline clinical depression to mild mood disturbance. The results support the findings of Peta Stapleton et al. [64], where they reported improvement in the participants having major depression with 8 sessions of EFT. The stress score in both groups was in the mild range.
There was significant improvement in forward digit span with CBT intervention. Result supports the study by Fatemehsadat A. et al (2015) [31]. There was a significant reduction in depression and improvement in psychophysiological coherence in CBT group post intervention. Results support the study by Hartmann Ralf et al (2019) which concluded that change in HRV parameter values correlated with changes in the severity of depressive symptoms and Dan Malm et al. (2018) which concluded that a mindfulness-based CBT program improved the health-related quality of life, sense of coherence and reduced psychological distress up to 12 months [40, 26].
Another subject, who was a 40 years old male, had severe stress and anxiety and moderate depression pre intervention. He showed noticeable improvement with CBT intervention therapy after 8 sessions. His stress score came in the range of normal and anxiety and depression in mild range. There was a marked improvement in STM span after 8 sessions. Even after continuing the home plan there was no further improvement seen in the subject after 1 month and 6 months of follow up. A mild anxiety and mild mood disturbance were observed after 6 months of follow up. There was no further change in STM span.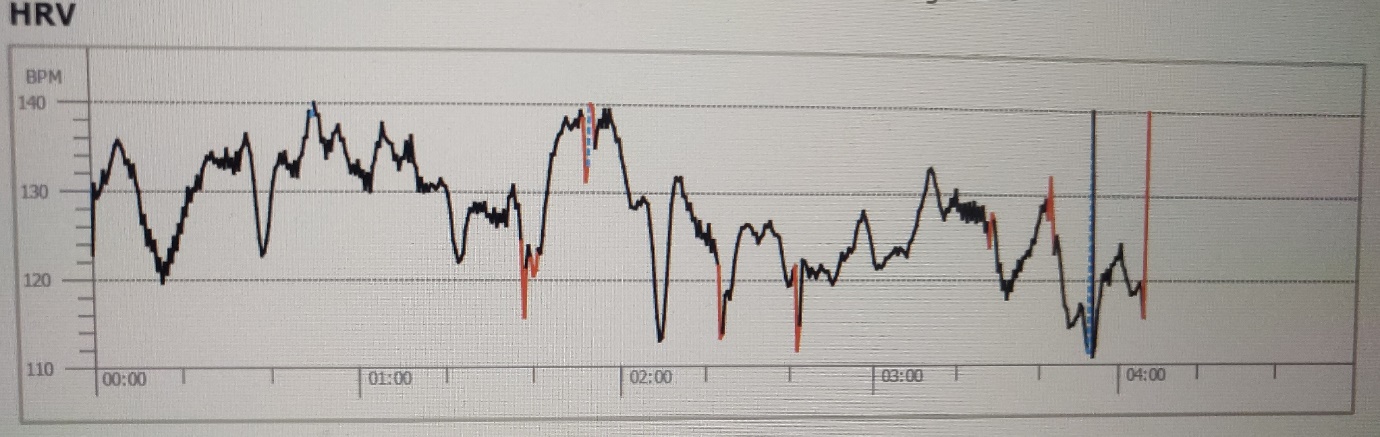
Pre-Intervention - Coherence-1.1 Heart rate-120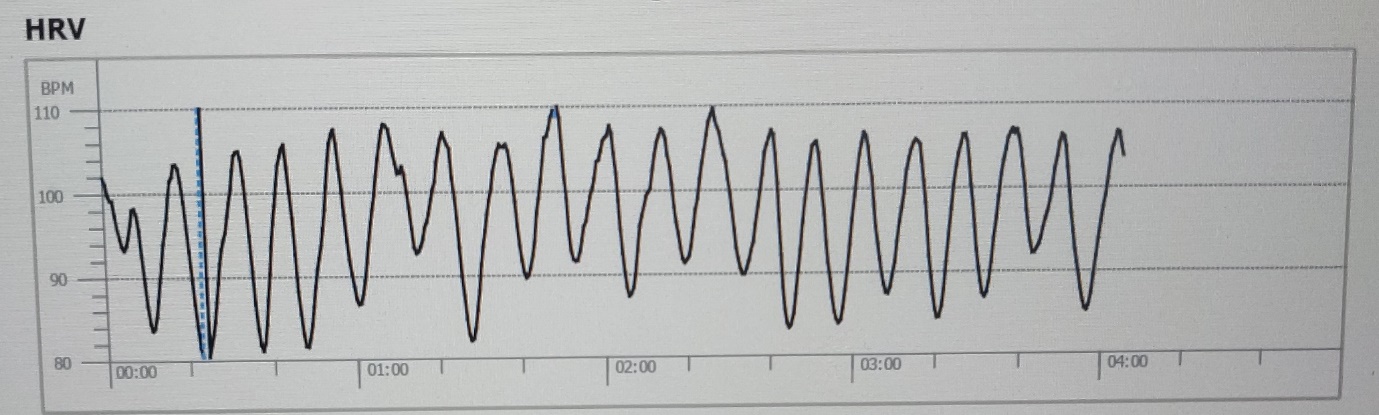
Post-Intervention - Coherence-4.6 Heart rate-82
His psychophysiological coherence was 1.2 and heart rate was 120 pre intervention. After the 8 sessions his psychophysiological coherence and heart rate improved drastically. It came down to 4.6 and 82 respectively. The result supports the study done by Hartmann Ralf et al (2019) where he concluded that change in HRV parameter values correlated with changes in the severity of depressive symptoms [40,71,84]
After 1month of follow up, the EFT group significantly showed further improvement in depression and scores across all the tests were within normal range. The CBT group reported a significant reduction in depression after 8 sessions, while EFT group reported a delayed effect. Results support the study conducted by Hannah Chatwin et al [39].
After 6 months of follow up, the results were more or less similar to 1 month of follow up where EFT group showed significantly better results in depression score and scores across other tests were within the normal range in EFT group. There was no further improvement in CBT group.
The individual cases revealed clinically significant improvements in stress, anxiety and depression across both the interventions. Results support the study conducted by Hannah Chatwin et al [39]. There was a significant improvement in the short-term memory post interventions. There is limited research available on the effect of depression, anxiety and stress on short term memory and corelation between psychophysiological coherence, heart rate, depression, stress and anxiety. In a study Tallie Z. Baram and UC Irvine, reported that acute stress activated selective molecules called corticotropin, which disturbed the processing of receiving and storing memories [82]. It may be concluded that reduction in stress, anxiety and depression symptoms can improve the STM memory loss. The finding needs further validation.
The overall results indicated that a slightly greater effect was achieved by the CBT group in terms of depression scores post-intervention. Findings are highly consistent with prior studies that confirmed efficacy of CBT, such as Hannah Chatwin et al [39]. and Hofmann et al [44]. The results are also consistent with past studies that confirmed the efficacy of EFT, such as Church D [20], Jones, S. et al [46], Kalla Mahima et al [47, 48], Patterson SL [63], Sebastian et al [77] and Rowe J [72].
Thus, we can conclude that both the intervention therapies showed significant improvement in managing stress, anxiety, depression, STM span, psychophysiological coherence and heart rate. EFT intervention therapy can be an effective tool as a primary care treatment. The participants were able to build mental resilience and were able to cope with the life situations post EFT intervention.
Thus, we can conclude that EFT can be a promising tool for treating stress, anxiety and depression and improving STM, psychophysiological coherence and heart rate in the Indian population. Scientifically established comparative studies between EFT and CBT in Indian population for treating stress, depression, anxiety, STM, psychophysiological coherence and heart rate are yet to be conducted.
Conclusion:
The current study is in line with the pilot study by Hannah Chatwin (39) to examine and compare the effectiveness of CBT and EFT in reducing depression and anxiety among adults. The results indicated that a significant (p<0.05) effect was achieved by the CBT group in terms of depression, forward digit span and psychophysiological coherence scores post-intervention, while EFT group reported a delayed effect with a significant (p<0.05) reduction in symptoms after 1 and 6 months of follow-up. The results are consistent with the previous study by Hannah Chatwin et al [39]. The analysis of individual cases in both intervention groups revealed clinically valid improvements in depression, anxiety, and stress scores, STM span, heart rate and psychophysiological coherence scores post-intervention. Our emotions and thoughts can impact our brain. Stress, anxiety and depression can overload our minds and cause distraction and disinterest in your surroundings. This interferes with day-to-day activity and affect memory and concentration. Identifying and treating emotion triggers, stress, anxiety and depression by support, counselling and lifestyle changes, can significantly improve a quality of life, memory, psychophysiological coherence and heart rate [30].
The present study showed that a highly standardized CBT program had a favourable influence on stress, anxiety, depression, STM, psychophysiological coherence and heart rate, as compared to EFT group post interventions. The findings of the present study indicate that EFT may be an effective treatment approach for anxiety and depression and supports the finding of Patterson SL [63]. After the above study the researchers strongly recommend that EFT is of paramount importance as a pivotal tool in managing stress, anxiety, depression, STM, Psychophysiological coherence and heart rate in the Indian population. A direct control of emotional state or its control through cognitive processing are both indeed useful and have equally strong effect in correcting behaviour, physiological symptoms and improving memory.
Limitation and Recommendation:
Had the sample size been large enough, the effectiveness and variability of EFT and CBT interventions would have been more apparent. Further research on efficacy of CBT and EFT in reducing depression, anxiety and stress symptoms in a larger sample from varied cultures would provide more valuable inputs. A research on the relationship between stress, anxiety and depression with STM and the cognitive function, would provide more insight.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org