Orthopaedic Research and Surgery
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2994-8738 | Journal DOI: 10.61148/2994-8738/JORS

Karthikeyan T
Physiotherapy Center, NIMHANS, Bangalore, Karnataka, India
*Corresponding Author: Karthikeyan T, Physiotherapy Center, NIMHANS, Bangalore, Karnataka, India
Received date: May 30, 2021
Accepted date: June 16, 2021
Published date: June 18, 2021
Citation: Karthikeyan T. “Therapeutic Effects of core stabilization yoga and back care education for nonspecific low back pain’’. J Orthopaedic Research and Surgery, 2(3); DOI: http;//doi.org/03.2021/1.1014.
Copyright: © 2021 Karthikeyan T. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Non-specific low back pain is defined as low back pain not attributable to a recognizable, known specific pathology (eg, infection, tumour, osteoporosis, lumbar spine fracture, structural deformity, inflammatory disorder, radicular syndrome, or cauda equina syndrome. Studies have proved that yoga and core stabilization are individually effective in the relieving low back pain.
Objectives:
To find out the effects of yoga, back care education and core stabilization in non- specific low back pain.
Method:
45 Subjects with Non-specific low back pain aged between 30-45 years selected from outpatient department in clinical settings and randomized to back care education (n=15) (control group), Yoga (n=15) and Core Stabilization Exercises (n=15). The outcome measures used are Oswestry Disability Index and Visual Analogue Scale. The study was carried out for duration of 3month.
Results:
The ODI scores were reduced from 29.43±6.29 to 26.93±6.06 in group A, from 31.33±3.53 to 26.26±4.04 in group B and from 27.80±3.80 to 15.93±3.99 in group C. the other outcome of VAS scores were reduced from 7.00±0.75 to 5.46±0.64 in group A, from 7.20±0.67 to 4.53±0.52 in group B and from 6.80±0.77 to 2.80±0.68 in group C. There was a statistically significant difference found between the base line to post-test scores in all the three groups.
Conclusion:
The author concluded that the Core stabilization exercises found to be the most effective in treating Non-specific low back pain than yoga and back care education.
Introduction
Non-specific low back pain is defined as low back pain not attributable to a recognizable, known specific pathology (eg, infection, tumour, osteoporosis, lumbar spine fracture, structural deformity, disorder, radicular, or syndrome. Low back pain is a very common problem in industrialized countries, affecting over 70% of the working population. In India, occurrence of low back pain is alarming, nearly 60% of Indians have significant back at sometime of their lives. Many people have their first episode of low back pain in their late teens or early twenties and these episodes frequently reoccur throughout adult life. For individuals younger than 45 years, Non-specific low back pain represents the most common cause of disability and is generally associated with a work-related injury [1].
Anatomy and biomechanics of low back
Each area of the spine is composed of stacked bony vertebral bodies with interposed cushioning pads called discs. The vertebral bodies provide protection for the spinal cord and nerve roots. Between each vertebral body, the disc serves as a shock absorber, giving you the flexibility to move. Each disc consists of a jelly-like fluid filled centre or nucleus surrounded by a stiff ligament-like outer ring called annulus [2].
Biomechanically, the movements of the lumbar spine consist of the cumulative motions of the vertebrae, with 80-90% of the lumbar flexion/extension occurring at the L4-L5 and L5-S1 intervertebral disks. The lumbar spine position most at risk for producing LBP is forward flexion (bent forward), rotation (trunk twisted), and attempting to lift a heavy object without-stretched hand. Axial loading of short duration is resisted by annular collagen fibers in the disk. Axial loading for a longer duration creates pressure on the annular fibrosis and increased pressure to the end- plates. If the annulus and endplate are intact, the loading forces can be adequately resisted. However, compressive muscular forces may combine with the loading forces to increase intradiscal pressure that exceed the strength of annular fibers [3].
Repetitive, compressive loading of the disks in flexion (eg. lifting) puts disks at risk for an annular tear and internal disk disruption. Likewise, tortional forces on the disks can produce shear forces that may induce annular tears [4].
In lumbar flexion, the highest strains are recorded within the interspinous and supraspinous ligaments, followed by the intracapsular ligaments and ligamentumflavum. In lumbar extension, the anterior longitudinal ligament experiences the highest strain. Lateral flexion produces the highest starins in the ligaments contralateral to the direction of bending. Rotation generates the highest strains in the capsular ligaments. Pathophysiology of low back pain [5].
Causes of NSLBP generally are attributed to an acute traumatic event, but they may also include cumulative trauma as an etiology. The severity of an acute traumatic event varies widely, from twisting one’s back to being involved in a motor vehicle collision. NSLBP due to cumulative trauma tends to occur more commonly in the workplace.
NSLBP alters in relation to poor postures and physical activities like twisting and lifting, bending, extending or poor exercises. It is aggravated or worsened by activity and relieved partially by rest without radiating to the lower limbs.
Typical physical findings are non-specific, including restricted range of motion of the spine, tight hamstring muscles, paravertebral muscle spasms, muscular trigger points, tenderness.
Yoga
The evidence based nonspecific low back pain managed through complementary and alternative medicine (CAM) therapies
Mechanism of yoga
The mechanism of action responsible for Yoga’s potential positive effect on back pain are physical movement, relief of physical and mental stress and enhanced body awareness to reduce maladaptive movements and posture. Yoga may decrease the pain and/or dysfunction of person with back pain through one or more of three major path ways; physical functioning of the back, cognitive appraisal about back pain and general affect and stress [6].
Core Stabilization
The core is defined as thalumbo-pelvic-hip complex. The core is where our centre of gravity is located. The core can be described as a muscular ‘box’ with the abdominals in the front; transversusabdominis, rectus abdominis, internal obliques and external obliques. The paraspinals; erector spinae, quadratuslumborum, multifidi, deep transversospinalis and the gluteals form the back of the ‘box’, the diaphragm as the roof and the pelvic floor and hip girdle musculature as the bottom [7].
Diaphragm and the Pelvic floor: Their primary contribution to lumbar stability is through co-contraction with the abdominals to increase intra-abdominal pressure, thus creating a rigid cylinder or an anatomical back brace to decrease the load on the spine.
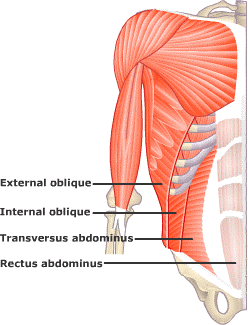
Fig no. 1. Core muscles.
Core Stabilization: it is described as the ability to control the position and motion of the trunk over the pelvis and leg to allow for optimum production, transfer and control of force and motion to the terminal segment in integrated kinetic chain activities.
Core Stability Exercises: It is described as a spectrum of exercise approaches that have the common goal to improve lumbo pelvic control, restoration of the ability of the neuromuscular system to control and to protect the spine from injury or re-injury. In general, it can be divided into two main groups:
Those that aim to restore the co-ordination and control of the trunk muscles to improve control of the lumbar spine and pelvis.
Those that aim to restore the capacity (strength and endurance) of the trunk muscle to meet the demands.
Importance of Core Training:
A strong core is the basis for all human movement.
If the core is strong and stable, all other movements are more efficient and more effective.
Poor core stability means that power is wasted. Instead of forces being applied by arms or legs to the movement, it is absorbed by a weak, sloppy trunk.
A strong core reduces the stress on particular muscle groups and joints.
Poor core stability increases the likelihood of injury in these areas. Excess stress is placed on these areas if the trunk is weak.
Back Care Education
One of the important parts of Non-specific low back pain treatment is the back care education. This includes modification in activities of daily living, ergonomic back care and the do’s & dont’s.
Studies have proved that yoga and core stabilization are individually effective in the relieving low back pain.
Objectives
To find out whether yoga ,core stabilization and back care education is more effective in treating non- specific low back pain.
Methodology
Study Design:
A Comparative Experimental study.
Settings
Physiotherapy unit, NIMHANS, Banglore.
Population: Subjects with Non-specific low back pain between 35-45 years of both sexes.
Selection Criteria
Inclusion criteria:
i.e. Moderately disabled
Subjects willing to participate
Exclusion criteria:
Others
Sampling Method and Sample Size:
Sampling Method: Simple Random Sampling
Sample Size: 45 subjects
Duration of study- 3 month
Materials Required: Mat
Outcome Measure: - Oswestry Disability Index and Visual Analogue Scale.
Procedure:
45 non- specific LBP subjects will be selected according to the selection criteria and an informed consent will be obtained from them. Investigator assessed with oswestry disability index and visual analogue scale and their respective scores documented.
The selected subjects will be randomly divided into 3groups A, B, C with 15 subjects in each group.
Group A- The Control group:- these subjects advised with back care education. They provided with hand-outs having the following:-
|
S.no |
Do’s |
Don’ts |
|
1 |
Proper weight lifting
|
Sleep in the prone position
|
|
2 |
Sitting with buttocks tucked under
|
Rise from sitting position suddenly
|
|
3 |
While driving push the seat forward to raise the knees and decrease the lordosis
|
Bend over a wash basin
|
|
4 |
Turn to side and then get up
|
Wear high heels
|
|
|
|
Use of too high chair
|
Use soft mattress.
Subjects asked to come to the department for follow up in every seven days and their oswestry disability index and visual analogue scale score recorded.
Group B: - These subjects allocated for Yoga-based therapy. Five yoga asanas in all should be practiced. The subjects priorly educated about its benefits in relieving their back pain and the techniques of each asana will be demonstrated and the do’s and don’ts instructions given. The protocol which followed is given below:-
Breathing exercises, Pawanmuktasana, Bhujangasana, Paschimottasana Setubandhasarvangasana and Sputa matsyendrasana.
Each asana repeated five times with the ‘hold time’ of the pose of minimum 30 seconds and maximum of 90 seconds except for the Pawanmuktasana and Paschimottasana which have the ‘hold time’ of minimum of 5-10 seconds as taking deep breathes in these positions is difficult.

Fig no 2: Pawanmukttasana

Fig no.3: Suptamatsyendrasana
Group C: - These subjects assigned for Core Stabilization Exercises regime. The subjects will be priorly educated about its benefits in relieving their back pain and the techniques of the exercises will be demonstrated and the do’s and don’ts instructions given. The protocol is given below:-
Lumbo-pelvic stabilization i.e. correct contraction of the core muscles taught first in quadrapod position followed by prone lying, supine lying, sitting and standing.
Bridging
Bird-dog exercise.
The contraction of the core muscles in each of the above exercises should be held for 10 seconds with ten repetitions of each exercise. The normal breathing with the contraction should be assured.
In week 4 exercises continued with addition of 5 seconds holding time i.e., 1st week - 6 reps,2nd week -9 reps,3rd week -12 reps and 4th week -15reps with 5-10 sec hold

Fig no. 4: Bird-Dog Exercise

Fig no.5: Bridging
The first session of both yoga and core stabilization exercises supervised, to make sure that the subjects have understood the technique of performing their respective asanas and exercises.
After the first session, group B and C subjects given hand-outs with pictures and clear details and instructions of yoga asanas and core stabilization exercises respectively. They will be called to the department once after 1month and their oswestry disability index and visual analogue scale score will be taken.
Results
Group A (Back Care Education)
Group B (YOGA)
Group C (Core Stabilization Exercises)
|
Age in
years |
Group A |
Group B |
Group C |
|||
|
No |
% |
No |
% |
No |
% |
|
|
30-35 |
8 |
53.3 |
9 |
60.0 |
9 |
60.0 |
|
36-40 |
5 |
33.3 |
3 |
20.0 |
5 |
33.3 |
|
41-45 |
2 |
13.3 |
3 |
20.0 |
1 |
6.7 |
|
Total |
15 |
100.0 |
15 |
100.0 |
15 |
100.0 |
|
Mean ±
SD |
30.60±4.12 |
30.87±4.49 |
29.93±3.78 |
|||
Table 2: Age distribution of patients studied
|
ODI% |
Group A |
Group B |
Group C |
P value |
|
Pre |
29.43±6.29 |
31.33±3.53 |
27.80±3.80 |
0.134 |
|
Post |
26.93±6.06 |
26.26±4.04 |
15.93±3.99 |
<0.001** |
|
P value |
<0.001** |
<0.001** |
<0.001** |
- |
Table 3: Comparative evaluation of ODI% in three groups of patients studied
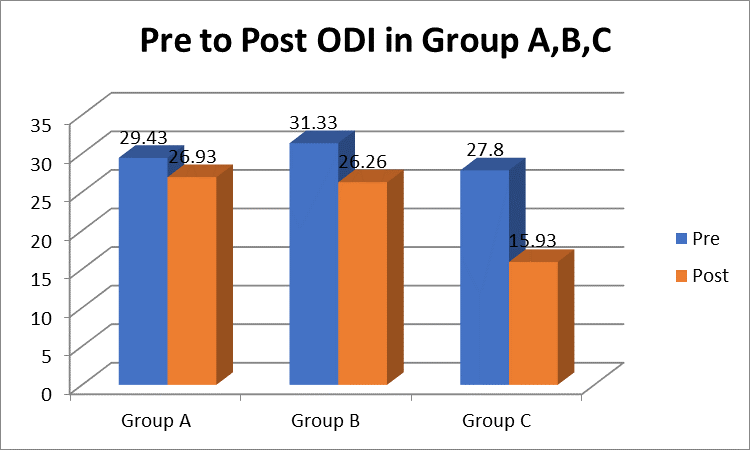
Fig 3: Pre to post ODI Score in Group A, B, C
Group A
The pre-test mean score of ODI 29.43and the post-test means score 26.93. Finally, 2.5 score level obtained reduced from pre to post of ODI.
Group B
The pre-test mean ODI 31.33 and the post-test mean 26.26. Finally 6.26 score level obtained reduced from pre to post of ODI.
Group C
The pre-test mean 27.80 and the post-test mean 15.93. Finally 11.9 score level obtained reduced from pre to post of ODI.
|
VAS |
Group A |
Group B |
Group C |
P value |
|
Pre |
7.00±0.75 |
7.20±0.67 |
6.80±0.77 |
0.341 |
|
Post |
5.46±0.64 |
4.53±0.52 |
2.80±0.68 |
<0.001*8 |
|
P value |
<0.001** |
<0.001** |
<0.001** |
- |
Table 4: Comparative evaluation of VAS in three groups of patients studied

Fig 3: Pre to post VAS Score in Group A,B,C
Group A
The VAS pre-test mean score 7.00 and the post-test mean 5.46. Finally 1.54 score level obtained reduced from pre to post of VAS.
Group B
The pre-test mean score of VAS 7.20 and the post-test mean 4.53. Finally 3.2 score level obtained reduced from pre to post of VAS.
Group C
The VAS pre-test mean 6.80 and the post-test mean 2.80. Finally 4.0 score level obtained reduced from pre to post of VAS.
Discussion
The present study was conducted to see the significant difference between the Back care education, Yoga and Core Stabilization exercises on NSLBP using ODI and VAS as the outcome measures for a duration of one month..
Demographic data
The mean age of all the 3groups have not shown any significant difference which indicates that the groups were homogenous and comparable.
ODI and VAS scores
In this study the pre-test values of ODI and VAS scores showed no significant difference between the 3groups. Due to the homogenous nature of the basal value, the post-test values were comparable.
All the 3groups have shown decrease in pain and disability which reveals all the 3 techniques i.e. back care education, yoga and core stabilitization exercises were beneficial in relieving NSLBP.
Core Stabilization
Group C underwent core stabilization exercises has shown a significant difference in the pre and post-test scores of both ODI and VAS. Core stabilization aims to restore the co-ordination and control of the trunk muscles to improve control of the lumbar spine and pelvis. It also aims to restore the capacity (strength and endurance) of the trunk muscle to meet the demands [10].
Similar study was done by where they had concluded that core stabilization exercises are effective in treating chronic low back in his study concluded that core stabilization exercises improve muscle activation patterns in chronic LBP patients. have studied that there are ample evidences that individuals with chronic LBP lack proper recruitment of core muscles and exhibit core weakness [8]. Patients with back pain also seem to over-activate superficial global muscles whereas control and activation of deep spinal muscles is impaired. Thus, core stability exercises have strong theoretical basis for treatment and prevention of LBP. It also improves function in patients with LBP.
No single muscle can be identified as being more important for spinal stability than another during a range of trunk movement tasks. Therefore, current study assesses the group of muscles or the effect of exercises on pain and disability as a whole and not done separately. These results suggest that core stability exercise program can effectively reduce back pain and disability in mechanical low back ache subjects.
Yoga
Group B underwent yoga as their intervention, has also shown a significant difference in the pre and post-test scores of both ODI and VAS. Yoga includes physical exercise coupled with the focus on special breathing techniques to increase awareness. The yoga postures work to release tight superficial back muscles, increase circulation to the injured area, and decrease inflammation. Similar study where they concluded that yoga was more effective than a self-care book for improving function and reducing chronic low back pain. Likewise, have studied that yoga intervention in a predominantly minority population with chronic low back pain was moderately feasible and may be more effective than usual care.
However, in this study yoga has proved to be less effective than the core stabilization exercises which is because yoga asanas are more about stretching the muscles of the body to reach the final positions that are effective, some people might not be flexible enough to stretch their bodies to attain the actual asanas. Whereas, core stability exercises are easy to perform and does not involve a lot of stretching. Yoga is an overall involvement of the body muscles where in core stabilization exercises concentrate on the core muscles only which are mainly responsible for spinal stability which in turn is necessary to alleviate and prevent NSLBP [8].
Back Care Education
Group A was given back care education which included the do’s and don’ts, correct lifting, driving, standing techniques and also to correct and maintain a correct posture to reduce and further prevent NSLBP. Similar study group instruction in physiotherapy for low back pain is safe, generally successful, and highly acceptable to patients [9].
In this study, this group has shown least difference in the pre and post-test scores of ODI and VAS, when compared to the yoga (group B) and core stabilization exercises(group C) groups. Education alone may work in a preventive rather than curative. This was because this group was not incorporated with any kind of exercises.
Conclusion
After analysing the results of this study, it can be said that the core stabilization exercises are effective in reducing NSLBP.
The research hypothesis made before the study was done has been proved correct. Also the objectives of the study is met proving:-
Core stabilization exercises to be more effective than Yoga in treating NSLBP.
Core stabilization exercises are superior to Back-care education in treating NSLBP.
Yoga is superior to Back-care education in treating NSLBP.












Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org