Khalid A K Elmajri 1* and Fathy Abdolmejed 2
1Department of ophthalmology, teaching Alwahda hospital ,The Omer Almuktar University, Derna, Libya.
2Department of ophthalmology, Tobruk medical center, Tobruk medical University –Tobruk, Libya.
*Corresponding Author: Khalid A K Elmajri, Department of ophthalmology, teaching Alwahda hospital ,The Omer Almuktar University, Derna, Libya.
Received Date: October 15, 2022
Accepted Date: Novemmber 24, 2022
Published Date: March 04, 2023
Citation: Khalid A K Elmajri and Fathy Abdolmejed. (2023) “Trachoma Diseases in conflict-affected areas - Derna city eastern part of Libya Review of Their Prevalence, Distribution, and Disease Burden”, Ophthalmology and Vision Care, 3(1); DOI: http;//doi.org/03.2023/1.1035
Copyright: © 2023 Khalid A K Elmajri. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
AL thought fighting trachoma does not require much hardware. Even during the civil war, annual drug distribution was still implemented by village networks. Trachoma and 16 other neglected tropical diseases together afflict 1 billion people worldwide, but most are “a forgotten disease of a forgotten people who live beyond the end of the road”. Those with trachoma are “not a population with a loud voice—or any voice. Politicians and policy makers don't fall over trichiasis patients on their way to work”. The Following years of civil war, in much of countries many people faces a lack of water and poor sanitation. The poor hygiene conditions mean that diseases such as trachoma - the world's leading infectious cause of blindness. [2, 50]
Introduction:
AL thought fighting trachoma does not require much hardware. Even during the civil war, annual drug distribution was still implemented by village networks. Trachoma and 16 other neglected tropical diseases together afflict 1 billion people worldwide, but most are “a forgotten disease of a forgotten people who live beyond the end of the road”. Those with trachoma are “not a population with a loud voice—or any voice. Politicians and policy makers don't fall over trichiasis patients on their way to work”. The Following years of civil war, in much of countries many people faces a lack of water and poor sanitation. The poor hygiene conditions mean that diseases such as trachoma - the world's leading infectious cause of blindness. [2, 50]
Too many people in this part of the world are still suffering as a result of trachoma – with conflict a major barrier to them getting the treatment they need. to help people living in conflict-affected areas – for example in Somalia and Afghanistan - to protect them from this painful, blinding disease. which has been ravaged by several years of civil war and where many face an inadequate water supply and poor sanitation - conditions that help trachoma thrive. [2, 8]
Trachoma, one of the world’s oldest diseases, is an infectious condition spread by flies and contact with eye discharge from a person with infection. It starts as a bacterial infection and if it is left untreated, scar tissue can develop in the eyelid, turning eyelashes inwards. With every blink, eyelashes painfully scrape the surface of the eye and can cause irreversible blindness. It is one of a collection of conditions known as neglected tropical diseases (NTDs). [6]
The neglected tropical diseases (NTDs) are a group of chronic, disabling, and disfiguring conditions that occur most commonly in the setting of extreme poverty, especially among the rural poor and some disadvantaged urban populations. [51]
when WHO began to focus on eliminating trachoma. So far, the disease has been virtually wiped out in Morocco, Oman, Burma, Vietnam, the Gambia, and Ghana, though monitoring of the disease continues. However, neglected tropical diseases are finally getting more attention. WHO published a new report on the topic in 2010. This February partners in alliance with WHO committed US$785 million to target ten neglected tropical diseases until 2020; the Bill & Melinda Gates Foundation pledged $363 million of that. Worldwide, 325 million people, especially children and women, are at risk of trachoma, and 41 million have active infections, according to US-based International Trachoma Initiative (ITI). [2, 3, 5]
Trachoma flourishes in dirty environments and close quarters in Asia, Africa, South America, the Middle East, and Australia. ITI estimates that trachoma is endemic in 53 countries. Infections can be transmitted through dirty hands, towels, and flies. Repeated infection leads to roughening of inner eyelids. More than 8 million people around the world suffer from trichiasis, the final stage of trachoma when entropion (in-turned eye lashes) causes scratching of the cornea and leads to blindness. Trachoma is preventable and treatable with antibiotics, improved hygiene and sanitation, and simple surgery before the disease becomes too advanced. Yet it was largely overlooked until 1997 .In Libya , the fight against trachoma has gained momentum for several reasons, including funding from and coordination among key international partners, donors, and the Libyan Government.Over the years, Eye care Foundation of the Netherlands, Seva Foundation and Orbis of the USA, Swiss Red Cross, Norwegian Church Aid, Christoffel Blinden Mission of Germany, and Lions International, among many others, have all supported eye care in Libya . With their help, eye hospitals and dozens of eye centres and clinics with trained staff have been established across Libya. [45, 46, 48]
The highest prevalence of active trachoma and trichiasis was seen in the African Region. Trachoma data were available from 18 countries with a further eight countries suspected of having trachoma but without data. The disease was predominantly located in the savannah areas of East and Central Africa and the Sahel of West Africa. [15, 46]
Prevention and treatment for trachoma is fairly inexpensive and simple through surgery, antibiotics, face washing, and environmental cleanliness, a strategy known by the acronym SAFE. At earlier stages, eye infections can be treated with oral antibiotics taken once a year, usually for several years. Years of repeated infection can cause the inside of the eyelid to scar so severely that the lashes scar the cornea. The new report also shows for the first time the full burden of illness, disability, and deaths caused by NTDs, finding it in the same order of magnitude as the "Big Three" diseases: HIV/AIDS, tuberculosis and malaria. [9, 25, 39]
Methodology/Principal Findings:
Design: Retrospective case series. Participants: Retrospective analysis of medical records from ophthalmology department –teaching alwahda hospital for 3757 file from November 2019 to jun 2020 in . Methods: Grades of trachoma diagnosis were according to the criteria designed by libyan Ophthalmological Society . The general state of health, age, gender, case history, and the laboratory investigations of patients were recorded: Manifestation of corneal and conjunctiva.
Result:
A total of 3757 patients were examined during 3 months, 127(3.38%)(95%CI 2.85-4.01%) of them were diagnosed with trachoma (Figure1 ). Of these, 64(50.4%) were male and 63(49.6%) were female.
Most of participants 120(94.5%) were Libyan, 118(92.9%) were live in Derna (Table 1)
Few of patients have chronic disease. 19 (14.9%) have hypertension and 18(14.2%) have Diabetes (Table 2).
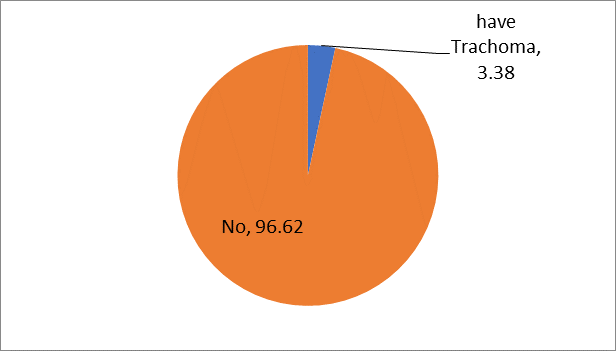
Figure 1: prevalence of Trachoma
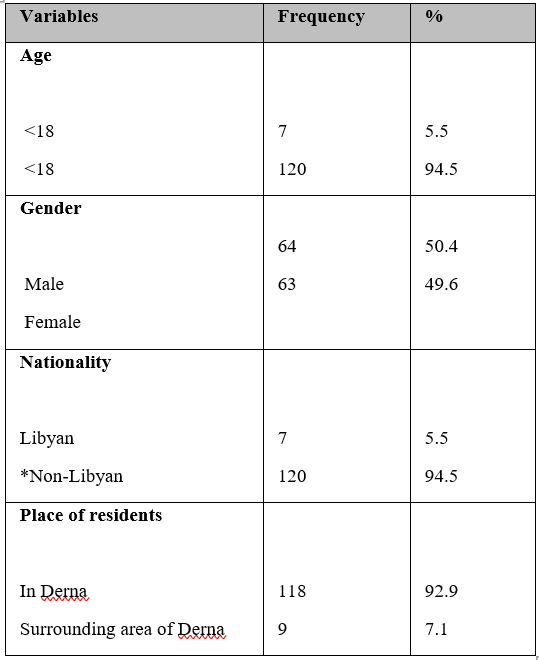
Table 1: Socio-Demographic Characteristics of the Study Patients (N=127)
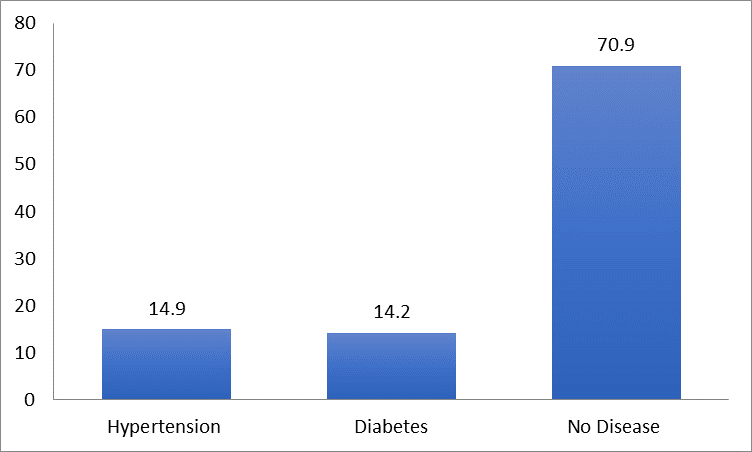
Table 2: Patients suffer from chronic disease
Conclusions/Significance:
This study demonstrated a strong association between trachomatous trichiasis and relative poverty, suggesting a bidirectional causative relationship possibly may exist between poverty and trachoma. Implementation of the full SAFE strategy in the context of general improvements might lead to a virtuous cycle of improving health and wealth. Trachoma is a good proxy of inequality within communities and it could be used to target and evaluate interventions for health and poverty alleviation.
Discussion:
Conflict is a complex multidimensional issue that encompasses not only deprivation of material possessions but also wider issues such as nutrition, health and education [32,33]. Many different approaches have been taken to measuring “conflict ”, both in absolute and relative terms [34]. In general, these involve a survey methodology to capture estimates of income or consumption and methods that take into account broader issues of health and education such as the Multidimensional socioeconomic Index [34].
In this study we compared individuals with trichiasis to matched controls from within the same communities in Amhara Region, Ethiopia using three different measures of relative poverty: Asset Index, Self-Rated Wealth Index and Peer-Rated Wealth Index. These measures allow us to understand whether people with TT were relatively poorer than their neighbours, even within these very poor communities. We performed a PCA of household assets to stratify the participants into economic groupings. The variance explained by the first principle component was similar to the range reported in other similar studies (between 11% and 27%) [19,20,27,36]. The asset index used in this study is probably a reasonable proxy for consumption expenditure as we collected data on a sufficiently broad set of asset indicators that are capable of capturing living standards and wealth inequalities based on local values [37].
Participant and Household Characteristics:
The age distribution, gender profile and literacy status of the trachoma cases in this study were comparable other studies of trachoma patients elsewhere in Sub-Saharan Africa [31,38–40]. This suggests that the results are probably generalizable for this region of libya at least. The households of trichiasis cases were significantly less well off than controls in terms of ownership of almost all asset indicators measured. Consistent with the literature, trichiasis cases had significantly smaller and more crowded households [6,41]. Cases had less latrine access and more kept their cattle within the house, which is consistent with observations that active trachoma is associated with poor sanitation access [41–43]. These differences reflect a gap in the implementation of the “E” component of the SAFE strategy, which needs on-going emphasis in this region.
Trachoma and Poverty:
We have found clear evidence from each measure that even within trachoma-endemic communities individuals and households affected by trachoma are significantly economically poorer than those that are not. Within endemic communities some individuals or families appear to be more severely affected by the disease and develop sight-threatening complications. This raises the important question of whether the association between conflict and trachoma arises from a general state of impoverishment or whether there are a number of critical factors that primarily drive the relationship that might be amenable to focused intervention. The data we present here suggest that the relationship between conflict and trachoma could possibly be bidirectional.
Conflict may contribute to trachoma. This study provides evidence that even within superficially homogeneous endemic communities relative poverty plays a major part in the vulnerability of families to scarring disease. Firstly, trachomatus cases were females mor than males in age group less than 18 years which may be do to more attention from the family to young children rather than adults in unstable situation as in civil wars . where the main family job is daily labouring and from families with no or lower formal education. Both of these factors have a major influence on income and health awareness, which in turn increase the vulnerability of the family to trachoma. Consistent with this, studies from Malawi, Tanzania and Ethiopia identified that children from lower socio-economic households had a higher prevalence of active trachoma than their counterparts indicating an association between poverty and active trachoma [10,44,45]. Secondly, previously described risk factor associations for active trachoma such as crowding and poor access to latrine, characterized the households of the trachoma cases in this study. Such conditions are believed to promote the transmission of Chlamydia trachomatis within endemic communities, sustaining higher prevalence levels. Poorer households and communities may be less likely to have either the resources or the awareness to access treatment and sustain a sufficiently hygienic environment to control trachoma [8,17,46,47].
Trachoma may also contribute to conflict . Poor health frequently results in loss of productivity through disability and diversion of resources [11]. Trachoma and its associated visual impairment probably lead to a loss of income, exacerbating pre-existing poverty in a “vicious cycle” [12,13]. Previously healthy and productive adults can be rendered dependent on others, unable to work or fully care for themselves due to pain, photophobia or visual impairment [13]. We found clear evidence of reduced activity and participation among trichiasis cases. Trichiasis cases were less likely than the controls to participate in productive household activities, outdoor activities (shopping/marketing, fetching wood and water) and agricultural activities (farming, animal husbandry and processing agricultural products).
Study Strengths:
This study comprehensively assesses the relationship between trachoma and economic poverty using four different measures, with a robust process to select suitable community controls. The asset index quantifies the long-term economic welfare of trachoma affected communities, which is important as trachoma and its sequelae are probably related to long-term SES [19,20]. The asset index has the practical advantage that it is much less affected by recall or measurement bias during data collection [19]. Most of the housing characteristics, utilities and durable assets were collected through direct observation minimizing miss-measurement. Broad ranges of asset data were collected increasing the power of the study in the following ways. Clumping and truncation, potential problems that can arise with PCA of asset data and compromise its suitability for defining socio-economic strata, did not occur when all asset indices were combined into a single index. This indicates that the data from this study is sufficient to measure economic status and effectively infer inequality between different socio-economic strata and that in this region assessment of economic status by asset measurement requires a wider pool of parameters, particularly including agricultural assets. Encouragingly, the asset based poverty measure was moderately and strongly correlated with the self-rated and peer-rated wealth measures.
Although a community based screening method was used to identify trichiasis cases, it is possible that some cases might have been missed, which could potentially introduce non-response bias. Similarly, it is possible that some potential controls were not listed by the sub-village administrators. Self and peer-rated wealth are subjective measures, which might have suffered from the tendency to favour ranking households in the middle of the distribution. The activity participation data relied on the participant’s recall ability on what s/he had done in the last week. Finally, our results suggest that a bidirectional relationship may possibly exist between trachoma and poverty. However, the authors recognise that inference about causality is speculative as it is not possible to draw firm conclusions from a cross-sectional observational study such as this.
Conclusions:
In this study we found a clear association between trichiasis and conflict situation by prevalence measures. These data are anticipated to be useful in advocacy and to support programme leaders and funders to secure resources to promote trachoma prevention linked to socio-economic development in trachoma-endemic communities. Implementation of the full SAFE strategy in the context of general improvements might lead to a virtuous cycle of improving health and wealth. Trachoma is a good proxy of inequality within communities and it could be used to target and evaluate interventions for health and poverty alleviation. Improved health potentially leads to improved productivity and income.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org