
Samson Dires, Waltengus Birhanu*, Hikma Amin, Melat Teklegiorgis, lidya Zewdie
Department of Otolaryngology, Head and Neck Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
*Corresponding Author: Waltengus Birhanu, Department of Otolaryngology, Head and Neck Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Received Date: May 23, 2024
Accepted Date: June 07, 2024
Published Date: June 10, 2024
Citation: Birhanu W, Dires S, Amin H, Teklegiorgis M, Zewdie L. (2024) “Fronto Choanal Polyp, 25 Years Old Ethiopian Male Rare Case Report.”, International Surgery Case Reports, 6(2); DOI: 10.61148/2836-2845/ISCR/072
Copyright: © 2024. Waltengus Birhanu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
Fronto choanal polyp is large, unilateral, solitary polyps that spread from the frontal sinus to the choana. To date, only 4 cases have been reported in the literature.
Case presentation
We report a rare Fronto choanal polyp in a 25-year-old male Ethiopian patient. Endoscopic polypectomy, right side maxillary antrostomy, anterior ethmoidectomy plus Frontal sinusotomy was done. Histopathology results come as inflammatory polyp.
Conclusion
Fronto choanal polyp is a rare type of choanal polyp. Diagnosis is made with the help of nasal endoscopic examination, paranasal sinus computer tomography, and histopathology examination. Endoscopic sinus surgery is a treatment of choice.
choana; frontal sinus; polyp
Background
Choanal polyps are large, unilateral, solitary polyps that spread from the site of origin to the choana. (1, 2 ,3) They can come from different areas of the nose and paranasal sinuses; they usually originate in the maxillary sinus antrum. (1,2,3) The literature has revealed that the nasal septum, sphenoid sinus, frontal sinus, middle turbinate, cribriform plate, and ethmoidal cells are other infrequently observed locations where they may originate.(5,8)Unilateral choanal polyps are frequently initially diagnosed as antrochoanal polyps during initial examinations because they most frequently originate from the maxillary sinus. antrum. One of the most typical signs of choanal polyps is nasal blockage on one side. (2,9)
Endoscopic examination and paranasal sinus CT are necessary in the differential diagnosis of nasal obstruction to identify uncommon diseases such as frontochoanal polyps.
This case report we are going to discuss the clinical presentation of frontochoanal polyps as well as the management of nasal obstruction in a 25-year-old male patient.
Case presentation
This is a case report of a 25-year-old Ethiopian male patient who presented with complaints of right nasal obstruction, right nasal discharge, and swelling in the right nostril. The patient has been experiencing these symptoms for the past one year, with the swelling becoming noticeable two months ago. There is no history of nasal bleeding, headache, visual disturbance, or any other chronic illnesses such as diabetes, hypertension, or cardiac illness.
Nasal endoscopy revealed a pale polypoid mass filling the right nasal cavity, extending to the right choana. However, the origin of the mass could not be identified. The left nasal cavity showed normal findings.
A computed tomography (CT) (Figure 1A&B) scan was performed, which showed a 3cm x 1cm x 3cm lesion having soft tissue attenuating and iso density ipsilateral opacification of frontal sinus and extended caudally into the nasal cavity. No erosion of skull base and lamella papyracia. Another paranasal sinus is free.

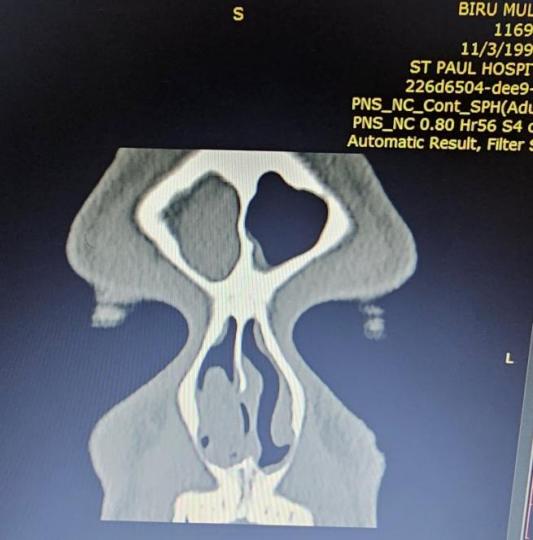
Figure1: computed tomography paranasal sinus.
With possible diagnosis of right frontochoanal polyp the patient operated, under general anesthesia. Intraoperatively there was Polypoid tissue filling the Rt nasal cavity with extension to choana with the attachment site from the Rt frontal sinus posterior wall which medialize the right middle turbinate.
The patient underwent endoscopic sinus surgery with polypectomy, right side maxillary antrostomy, anterior ethmoidectomy plus Frontal sinusotomy was done. (Figure 2) And tissue subjected for histopathology. Patient discharged with analgesic and advised on saline nasal irrigation and appointed after one week.
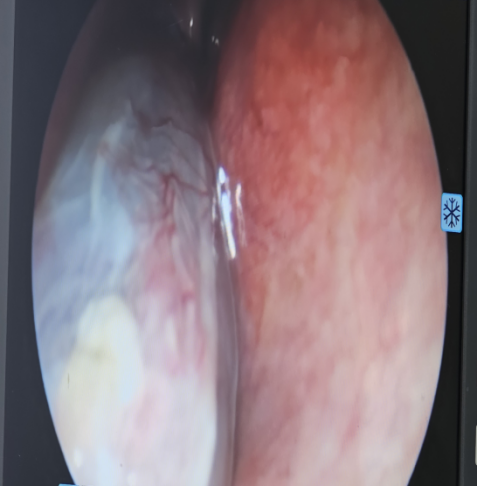
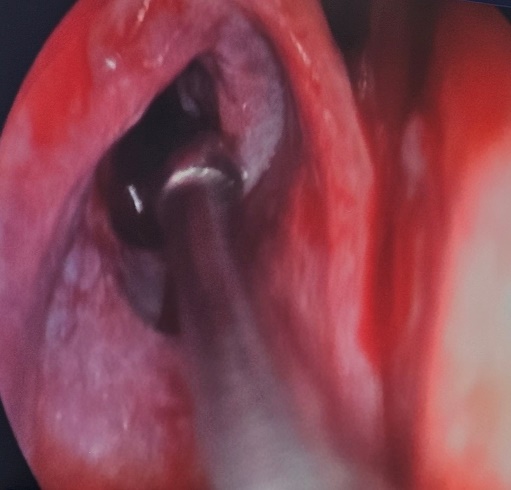
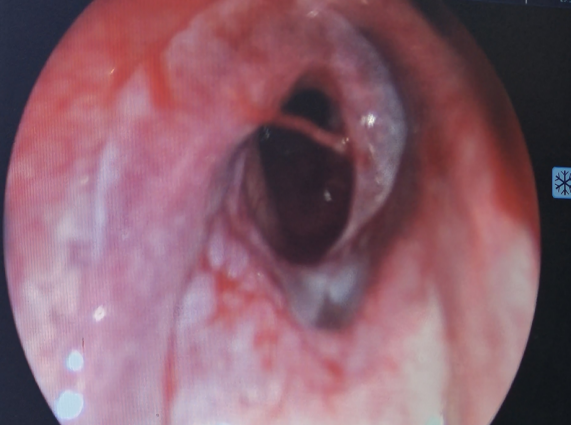
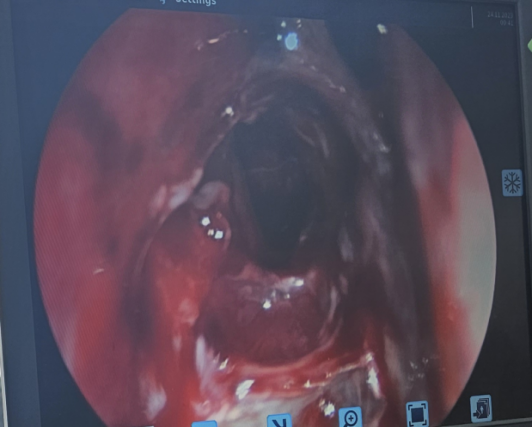
Figure 2: Intra operative finding.
Histopathology result comes as inflammatory polyp, section shows partly respiratory epithelium and partly stratified squamous epithelium lined polypoid tissue supported by inflamed & edematous subepithelial stroma with areas of inflammatory cell infiltrate consisting of eosinophils admixed with plasma cells and lymphocytes. (Figure 3)
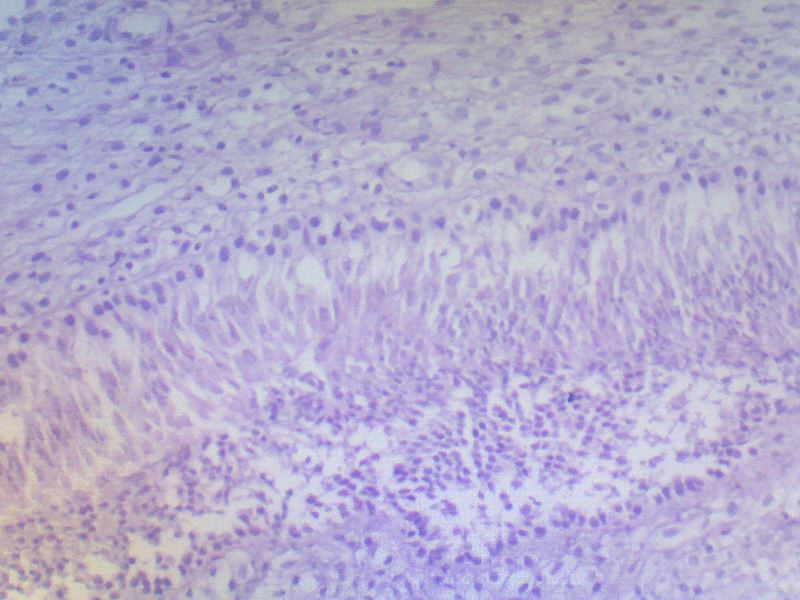
Figure 3: Histopathology.
Discussion
Anthro-choanal polyps, the predominant form among choanal polyps, represent approximately 3-6% of nasal polyps in adults and a substantial 28% in children. 2,4 Their formation often involves chronic inflammation and obstruction within the maxillary sinus, prompting the development of cystic structures. Under the influence of gravitational forces, turbulent airflows, and negative pressure within the maxilla, these polyps begin to extend from the lateral wall of the nose into the nasal passage and choana. 4,9,10.
The primary complaint associated with choanal polyps typically revolves around ipsilateral nasal obstruction. 1,3 However, patients may also present with a symptom including nosebleeds, snoring, headaches, postnasal drip, and anosmia (inability to smell). In more advanced cases where the polyps extend to the oropharynx, difficulty swallowing may also be reported.1,2,9.
To effectively diagnose choanal polyps and differentiate them from other nasal pathologies, endoscopic examination and paranasal sinus CT scans are indispensable. While anterior rhinoscopy aids in identifying common causes of nasal obstruction, it often falls short in revealing underlying osteometal complex and posterior nasal cavity pathologies. 12
Frontochoanal polyps, although rare, necessitate thorough endoscopic examination and paranasal sinus imaging for accurate diagnosis. Detection typically occurs through CT scans, while MRI or CT imaging is instrumental in determining the precise location and extent of the polyps. 8 Paranasal sinus CT scans typically reveal soft tissue involvement in a single sinus with extension to the choana, although biopsy remains crucial for definitive diagnosis.
Treatment of choanal polyps invariably involves endoscopic sinus surgery, serving both diagnostic and therapeutic purposes. Surgical intervention aims to meticulously remove the polyps and cleanse the affected area. Importantly, excising the sinus ostia from which the polyps originate is imperative to forestall recurrence. Literature reports a recurrence rate of approximately 25%, underscoring the significance of comprehensive surgical management and post-operative care to mitigate this risk.3
Despite their rarity, frontochoanal polyps do not deviate significantly from the treatment protocols applied to other choanal polyps, emphasizing the importance of tailored surgical approaches and meticulous follow-up care in achieving favorable outcomes.2
Conclusion
Frontochoanal polyps is a rare condition. Usually, patients presented with unilateral nasal obstruction. Endoscopic examination and paranasal sinus CT scans are important to rich a diagnosis of frontochoanal polyps. Endoscopic surgery is the treatment of choice, and it can provide immediate relief of symptoms with minimal morbidity.
Declarations
Ethics approval and consent to participate.
There are no ethical concerns about this case report.
Consent for publication.
Written informed consent was obtained from the patient to publish this case report and accompanying images. A copy of the written consent form is available for review by the journal's editor-in-chief.
Availability of data and materials
The corresponding author has all the data and materials for this case report.
Competing interests
We declare that there are no competing interests.
Funding
We received no financial support for this case report.
Authors' contributions
Waltengus Birhanu: writing, Editing, Review, and patient follow-up. Samson Dires: reviewing the original draft, and Supervision. Hikma Amin: writing, editing, and patient follow-up. Melat Teklegiorgis: writing, reviewing, editing, and patient follow-up. Lidya Zewdie: writing, editing, and patient follow-up.
Acknowledgments
Not applicable

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org