International Surgery Case Reports
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


Halit Batuhan Demir, Bartu Çetin, Tolga Girgin
Genel Cerrahi Anabilim Dalı, Ege Üniversitesi Tıp Fakültesi, İzmir, Türkiye
*Corresponding author: Halit Batuhan Demir, Genel Cerrahi Anabilim Dalı, Ege Üniversitesi Tıp Fakültesi, İzmir, Türkiye.
Received date: July 12, 2022
Accepted date: July 30, 2022
published date: August 04, 2022
Citation: Halit B Demir, Çetin B, Tolga Girgin. (2022) “Comparison Of Open Surgery and Transoral Approach in Zenker's Diverticulum”. International Surgery Case Reports, 4(3). DOI: http;//doi.org/11.2022/1.1056.
Copyright: © 2022 Halit Batuhan Demir. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Zenker's diverticulum is a true pulsion diverticulum of the esophagus. Symptoms such as dysphagia, a feeling of being stuck with swallowing, weight loss, regurgitation, coughing, aspiration can be seen. All these can lead to serious medical and social problems by reducing the quality of life. If left untreated, it can cause various complications. Therefore, surgical treatment is indicated in all symptomatic patients. In the surgical treatment of Zenker's diverticulum, endoscopic methods applied under general anesthesia have been used frequently in recent years. Endoscopic methods have gained popularity due to the shorter operative time, shorter hospital stay and transition to oral feeding, and low complication rates in selected patients. In this article, in the surgical treatment of Zenker's diverticulum; The open surgical approach and the transoral endoscopic surgical technique were compared. We think that transoral endoscopic diverticulotomy is an effective surgical option that can be safely performed in selected patients and can provide successful results at least in the early period.
Introduction
Zenker's diverticulum is a true pulsion diverticulum in which herniation of the pharyngeal soft tissue occurs through the Killian triangle above the cricopharyngeal muscle. [1] The occurrence of Zenker's diverticulum is attributed to insufficient relaxation of the cricopharyngeal muscle and insufficient opening of the upper esophageal sphincter, while the intraluminal pressure in the oropharynx increases during swallowing. [2] Patients often present with dysphagia, regurgitation, chronic cough, aspiration, and weight loss. [1][3] It is typically common among the elderly. [1]
Although the treatment of Zenker's diverticulum is conservative or surgical, it is recommended for symptomatic patients. [3] In recent years, the treatment of Zenker's diverticulum has changed from open surgery to transoral endoscopic techniques. [4] Within this group, there are two techniques performed via flexible and rigid endoscopy. [1] There is an increasing number of publications suggesting the superiority of the endoscopic stapled diverticulectomy technique.
Endoscopic stapled diverticulectomy
In the endoscopic diverticulectomy technique, intubation is applied to the patient after general anesthesia. The patient is placed in the supine position to perform the transoral procedure. The head is slightly extended, and the patient is placed in reverse Trendelenburg. (Figure-1)

Figure-1: Position of the patient for the transoral approach
Subsequently, the rigid retractor is placed trans orally. (Figure-2) Through the trans orally inserted endoscope, the posterior diverticulum and esophagus are monitored.

Figure-2: Materials used for rigid retractor
2 silk sutures are placed as slings in the midline of the septum via endo stitch. (Figure-3-4) The silks are removed out of the mouth so that traction is applied to these slings.

Figure-3: The image when one suture has been placed in the septum, and the other suture is being placed. In the inferior part, the Zenker's diverticulum is seen, in the superior part, the esophageal lumen is seen.
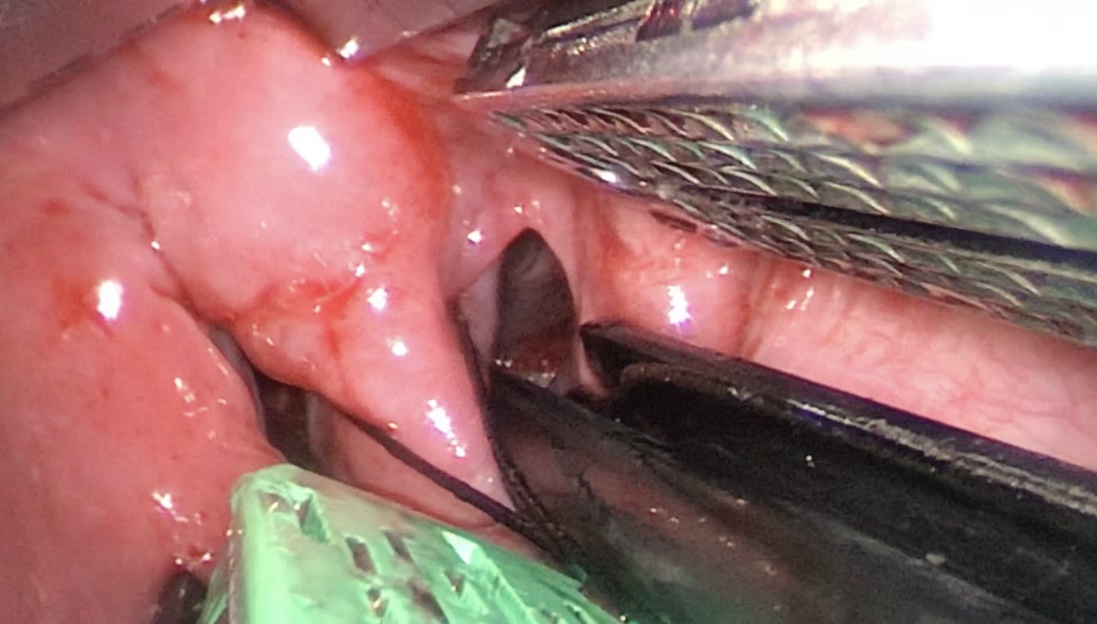
Figure-4: Image during the suspension of Endo Gia stapler with silk sutures and while advancing into the septum
The middle tissue is placed with the Endo GIA stapler in such a way that the septum diverticulum is fully opened into the esophagus and diverticulectomy is performed. (Figure-5-6)

Figure-5: Image of transection via Endo Gia stapler
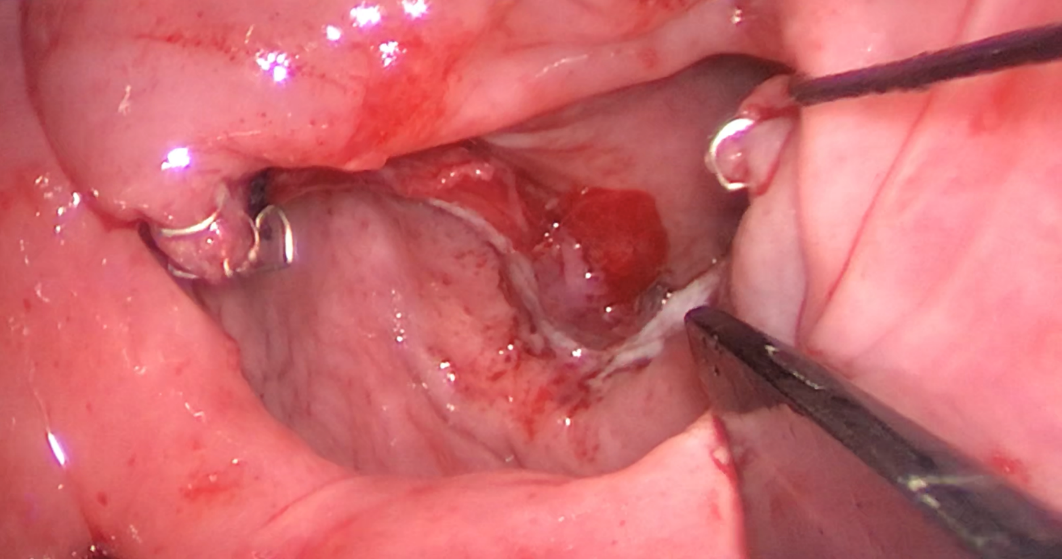
Figure-6: Post-transection with Stapler
Material and Method
All patients who were operated for Zenker's diverticulum between 2010 and 2021 in the upper gastrointestinal surgery clinic of Ege University General Surgery Department were retrospectively reviewed from the electronic database. Patients under the age of 18, patients whose data could not be accessed, patients who did not have sufficient follow-up period, or who gave up follow-up visits were excluded from the study. The patients in the study were divided into two groups those who underwent open surgery and those who underwent stapled diverticulectomy. Demographic data (age, gender), pre-operative symptoms (vomiting, dysphagia, regurgitation), presence of post-operative complications, duration of hospitalization, diverticulum size, and long-term recurrence status of all patients included in the study were transferred to an Excel file and analyzed. Then, these two groups were compared in terms of the above-mentioned data. During the follow-up period of the patients, their symptoms were questioned by telephone interview.
Results
A total of 12 patients were included in the study. Staple diverticulectomy was performed in 6 of 12 patients by open surgical technique, and in the other 6 patients by endoscopic technique. The patients who underwent open surgery were operated on using a cervical incision. Three of the patients who underwent stapled diverticulectomy with the endoscopic technique had previously undergone open surgery in another center for Zenker's diverticulum. In the endoscopic method, the approach in all patients was transection via Endo GIA Stapler after suspending the septum with 2 suspension sutures.
The mean ages of the patients who underwent endoscopic and open surgical modalities were 69(61-84) and 68(53-81), respectively. Of the patients who underwent open surgery, 5 were male and 1 was female. Of the patients who underwent endoscopic stapler diverticulectomy, 4 were male and 2 were female. Of the patients in the group who underwent open surgery, 1 had preoperative vomiting, 3 had dysphagia, and 2 had regurgitation. Meanwhile, in the endoscopic stapled diverticulectomy group, 4 of the patients had dysphagia and 2 had preoperative regurgitation before the procedure. The mean hospitalization duration of patients who underwent endoscopic stapler diverticulectomy was 3.66 (2-6), while it was 8.66 (6-13) in the open surgery group. The mean diverticulum size of the patients who underwent open surgery was 3.28 cm (2.8-4.2). The mean diverticulum size of the patients who underwent endoscopic stapler diverticulectomy was 3.7 cm (2.2-5.5). No postoperative complications occurred in either group. Patients who underwent open surgery were followed for an average of 3 years. The mean follow-up period of the patients who underwent endoscopic stapler diverticulectomy was 16 months. None of the 12 patients who underwent surgery developed a relapse. No active complaints were detected in the patients who were called and questioned for the study. One patient who underwent endoscopic stapler diverticulectomy died due to Covid pneumonia at the end of the 12-month follow-up period.
|
|
Open (n:6) |
Endoscopic (n:6) |
|
Age |
68 |
69 |
|
Gender -Male -Female |
5 1 |
4 2 |
|
Diverticulum diameter |
3.28cm |
3.7cm |
|
Active complaints -Vomiting -Difficulty swallowing -Regurgitation |
1 3 2 |
0 4 2 |
|
Duration of Hospitalization (days) |
8.66 |
3.66 |
|
Follow-up duration (months) |
36 |
12 |
|
Recurrence |
0 |
0 |
Discussion
Zenker's diverticulum is a pulsion diverticulum in which the pharyngeal tissue herniates through the Killian triangle in the hypopharynx. [5] Treatment is recommended in symptomatic patients. Open surgery has been replaced by flexible or rigid endoscopic techniques in recent years, though treatment methods are varied. [2] There are numerous studies suggesting the superiority of one method over another. A study by Chang et al suggested that endoscopic diverticulectomy is a safer and better alternative to open surgery in the treatment of the Zenker’s. [6] They attributed this situation to the fact that the stapler cuts the septum after suturing it with a stapler in endoscopic diverticulectomy, preventing saliva leakage and hemorrhage occurrence greater compared to other techniques. [6] Ultimately, endoscopic stapler diverticulectomy has a shorter duration of the procedure, faster oral intake duration, and shorter duration of hospitalization compared to open surgery. [7] Likewise, in our study, it was found that patients who underwent endoscopic diverticulectomy had a shorter duration of hospitalization compared to those who underwent surgery through an open cervical incision. (3.66-8.66)
Recurrence after surgery for Zenker's diverticulum is not common. [8] The risk of recurrence after surgery ranges between 4.2% and 18.4%. [4] Open surgery was conventionally recommended for revision in patients with recurrence, but endoscopic approaches have also been defined for recurrence surgeries in recent publications. [8] [9] In a study by Kedem et al., patients who underwent endoscopic diverticulectomy for the first time and who underwent endoscopic diverticulectomy as revision surgery were compared. No significant difference was found between the two groups in terms of duration of the procedure, technical difficulties, hospitalization, and complications. [8] In another study by Berger et al., no significant difference was found between open surgery and endoscopic approach in patients with recurrence, and both approaches were reported to be appropriate. [9] In our study, 3 patients had undergone surgery due to recurrence. All three patients underwent diverticulectomy via an endoscopic stapler. It was found that there were no complications in all three patients and no recurrence was observed in the follow-ups. Moreover, the hospitalization durations of these three patients were similar to those who underwent other endoscopic stapler diverticulectomy.
A total of 11% complications were observed in open surgery, although the complication rates vary. These complications were recurrent laryngeal nerve injury in 3%, leakage or perforation in 3%, and surgical site infection in 2%. [10] Meanwhile, in the endoscopic stapler diverticulectomy technique, the mean complication rate was 7%, with 2% tooth damage and 2% perforation. [10] On the other hand, the presence of a diverticulum or septum in the radiological images taken after the surgery in patients who underwent endoscopic treatment should not be considered an indicator of recurrence. [10] In our study, meanwhile, all of the patients were discharged without any complications.
Nowadays, transoral endoscopic stapled diverticulectomy is performed more commonly compared to conventional open surgery. [3] Similarly, in our clinic, endoscopic stapler diverticulectomy has been performed more frequently in recent years. Hence, the follow-up period of the patients who underwent open surgery in our study was longer than the patients who underwent endoscopic surgery.
Conclusion
With the developing technology, endoscopic methods have started to replace open surgery in the treatment of Zenker’s diverticulum. In numerous studies, it has been revealed that endoscopic diverticulectomy causes less morbidity, has a shorter duration of hospitalization and its recurrences are similar to open surgery. Likewise, in recurrent cases, the transoral endoscopic diverticulectomy method can be performed as its safety has been proven and its complications are similar to open surgery.
Additional Note: I would like to thank Prof Dr. Sinan Ersin, Prof Dr. Özgür Fırat, and Associate Dr. Taylan Sezer for their contributions.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org