International Surgery Case Reports
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2836-2845 | Journal DOI: 10.61148/2836-2845/ISCR


1Ilo Anthony Chukwudi, 1Chukwubuike Kevin Emeka*, Ilo Chikasi Adaobi, Eze Vivian Olachi 1Anijunsi Livinus Patrick, 1Nwabueze Goodness Ngesochukwu , Mbanefo Genevive Onyinye.
1Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
2Department of Radiology,University of Nigeria Teaching Hospital,Ituku Ozalla Nigeria
* Correspondind Author: Chukwubuike Kevin Emeka, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
Received date: May 17, 2022
Accepted date: May 27, 2022
published date: June 06, 2022
Citation: Ilo A Chukwudi, Chukwubuike K Emeka, Ilo C Adaobi, Eze V Olachi, Anijunsi L Patrick. (2022) “Sigmoid Volvulus in an Elderly Man: A Case Report”. International Surgery Case Reports, 4(2). DOI: http;//doi.org/11.2022/1.1052.
Copyright: © 2022 Chukwubuike Kevin Emeka. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Sigmoid volvulus is an emergency clinical condition in which the sigmoid colon twists around itself and its mesentery causing a closed loop bowel obstruction. We report a case of sigmoid volvulus in a 72-year old man who had primary bowel resection with end to end anastomosis. Case summary: An elderly man presented with a 3-day history of altered bowel habit. Altered bowel habit was characterized by constipation alternating with diarrhea which was said to be frothy. There was associated abdominal distension with abdominal pain which was colicky. He accepted to have had similar symptoms in the past. There was no history of previous abdominal surgery, no trauma, no abdominal mass, no family history of colorectal cancer and no bleeding per rectum. Clinical examination yielded stable vital signs and bowel sounds were hyperactive. Investigations such as plain abdominal x ray, hemogram, serum chemistry were done. Laparotomy with primary bowel resection with end to end anastomosis was performed. The post-operative period was essentially uneventful and patient was discharged home on the 7th day post-op. Conclusion: Sigmoid volvulus is an uncommon cause of bowel obstruction. In the absence of endoscopic facilities for decompression and detorsion at the acute stages in stable patients, bowel resection and anastomosis through laparotomy is an effective modality of treatment.
1. Introduction
Sigmoid volvulus is an emergency clinical condition in which the sigmoid colon twists around itself and its mesentery causing a closed loop bowel obstruction. It is a rare but an important cause of intestinal obstruction. Certain regions of the world such as Africa, Asia and South America are considered endemic regions for sigmoid volvulus [1, 2, 3]. Sigmoid volvulus account for 2% to 5% of colonic obstructions in developed countries and the highest incidence is in the 4th to 8th decades of life with more males affected [1, 4]. The etiology of sigmoid volvulus is multifactorial. There are predisposing anatomic factors which could be congenital or acquired. The congenital predisposing anatomic factor include narrow base of the sigmoid mesentery while an example of acquired predisposing factor is the redundancy of the sigmoid colon from chronic constipation, amongst others. Based on the etiology, sigmoid volvulus may be classified into primary or secondary. Secondary volvulus occurs as a result of other pathologies such as post-operative adhesions and internal herniation. Sigmoid volvulus may also be acute or chronic depending on the duration of symptoms. Abdominal pain, abdominal distension and constipation are the classical symptoms of acute sigmoid volvulus [2]. Plain abdominal radiograph is quoted to be diagnostic of sigmoid volvulus in 57% to 90% of the patients [5, 6]. Barium enema is diagnostic in 20% to 30% of the cases [7]. Diagnosis of sigmoid volvulus may be difficult and diagnosis is only made at laparotomy or autopsy [8]. The definitive surgical procedure for sigmoid volvulus includes resection of the sigmoid colon with or without primary anastomosis. We report a case of sigmoid volvulus in a 72-year old man who had primary bowel resection with end to end anastomosis.
2. Case Summary
A 72-year old man trader presented with a 3-day history of altered bowel habit and abdominal distension. Altered bowel habit was characterized by constipation with alternating diarrhea which was said to be frothy. He subsequently developed abdominal distension which was progressive and associated with abdominal pain. The abdominal pain was sharp in nature, colicky and did not radiate to any part of his body. There were no known relieving and aggravating factors. No history of vomiting and no passage of blood in stool. Patient has been having similar symptoms in the last 2 years. There was no tenesmus, no change in caliber of stool or passage of pellet like stool. There was a negative history of chronic cough, weight loss, drenching night sweat or fever, no jaundice. No preceding abdominal surgery, trauma, abdominal mass and no family history of colorectal cancer. He is a known hypertensive on Amlodipine 10mg for 2 years though not complaint with his medications. On account of the above symptoms, he presented to the accident and emergency unit of the teaching hospital for expert care. On examination by the general surgery unit, an elderly man in no obvious distress, anicteric, not cyanosed, not febrile. Respiratory rate was 20 cycles per minute, pulse rate 80 per minutes, blood pressure 150/95 mm Hg, temperature 36.5 0C. Chest was clinically clear. Abdomen was distended; moved with respiration, non-tender and bowel sounds were hyperactive. Digital rectal examination showed an empty rectum and there was no palpable rectal mass. A working diagnosis of large bowel obstruction secondary to intra-abdominal mass was made. Results of the investigations are as follows: Plain chest/abdominal x ray showed dilated bowel loops and no air under the diaphragm (figure 1). Serum chemistry, serology and hemogram were all within normal limits. An abdominal ultrasound was also done but was not diagnostic of sigmoid volvulus. Abdominal computed tomography (CT) scan was not done due to paucity of funds. The patient was optimized and was taken to theatre for laparotomy. Intra-op, massively dilated sigmoid colon with volvulus was seen (figure 2 and 3). However, the sigmoid colon was not gangrenous (viable). Detorsion of the sigmoid volvulus, resection of the redundant sigmoid colon with primary anastomosis were performed (figure 4). Post operatively, the patient had an uneventful recovery and was discharged home on the 7th day post-op.
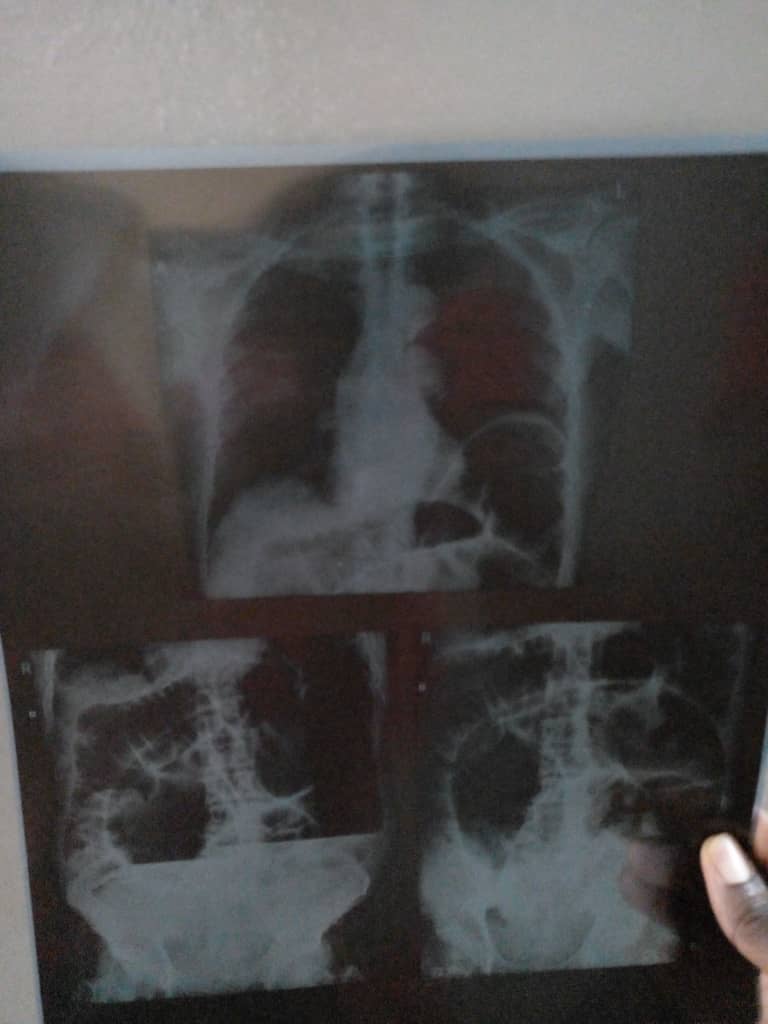
Figure 1: Plain chest/abdominal radiograph

Figure 2: Massively dilated sigmoid colon

Figure 3: Lateral view of the sigmoid volvulus with collapsed small intestine.
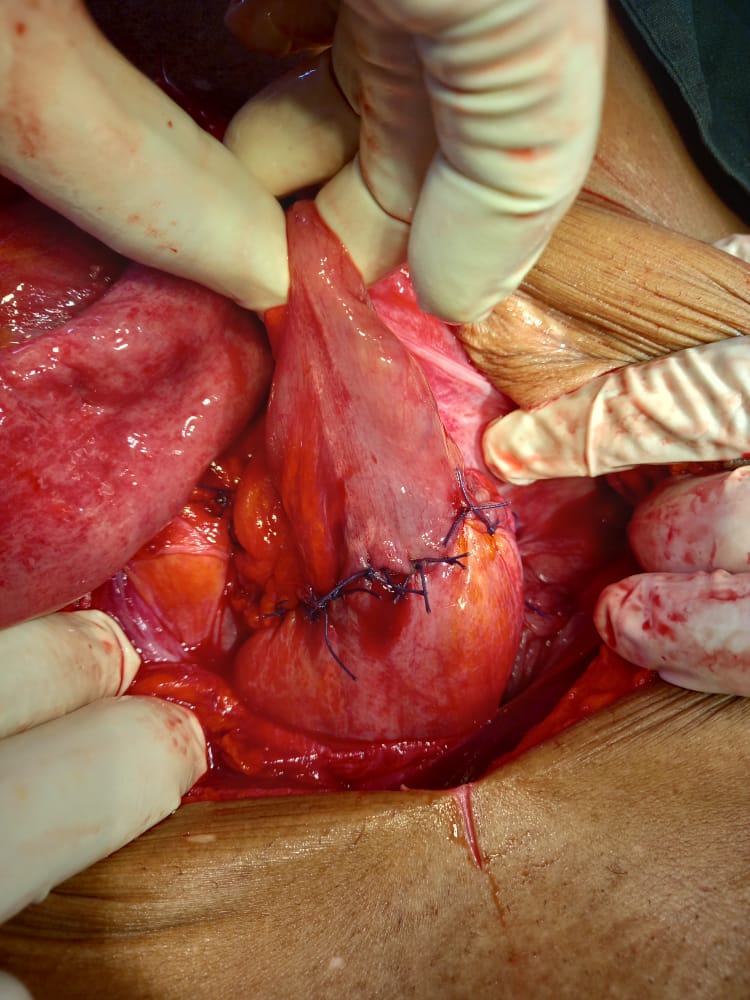
Figure 4: Anastomotic site
3. Discussion
The term volvulus is derived from the latin word “volvere” which means “to roll” [9]. Von Rokitansky first described sigmoid volvulus in 1836 [1].
Anatomically, the sigmoid colon is that part of the large intestine that is located distal to the descending colon but proximal to the rectum. Similar to the transverse colon, the sigmoid colon has a mesocolon around which twists can occur. Sigmoid volvulus is the most common type of colonic volvulus. The “volvulus belt” (Middle East, Africa, the Indian subcontinent, Turkey and South America) has been documented as the areas where volvulus is often reported [10].
The natural history of sigmoid volvulus is spontaneous detorsion or it may progress to impaired blood supply leading to bowel ischemia, necrosis and perforation with the possible attendant morbidity and mortality [11]. Intermittent sigmoid volvulus can occur with recurrent episodes of abdominal pain. Obstruction of the intestinal lumen occurs when the degree of sigmoid twist exceeds 1800 and 3600 respectively [Shepherd].
In the present case report, the patient is an elderly African male. Elderly males are more affected with sigmoid volvulus. The increased risk of sigmoid volvulus in the elderly may be due to the associated risk factors such as chronic constipation, immobility (bedridden) and neuropsychiatric disorders seen in the elderly [12]. Although sigmoid volvulus is more common in the elderly population, sigmoid volvulus has also been reported in neonates, infants and older children [13, 14]. The index patient being discussed is a male. Other series on sigmoid volvulus also reported this male predominance [15, 16]. Irregular bowel behavior and high fiber diet seen in males may explain more occurrences in males. This high fiber produces lots of flatus and bulky stool that elongates and dilates the sigmoid colon which may subsequently lead to volvulus. Sigmoid volvulus is more common in Africans and the explanation for this could be the nature of the diet and narrow base of sigmoid mesentery in African population. A long sigmoid colon with long mesentery, but with a narrow base is likely to predispose to sigmoid volvulus [17]. The index patient had abdominal pain, abdominal distension and constipation. Hassan et al also reported exact same symptoms [18]. Perrot et al documented a triad of abdominal distension, low abdominal crampy pain with constipation and vomiting [19]. Vomiting is usually a late symptom. There may be previous history of similar symptoms which resolved spontaneously. Our patient also gave a history of similar symptoms in the past. It is important to note that the clinical presentation of sigmoid volvulus may be acute with peritonitis and shock especially in late presenters and in such cases the prognosis is poor [19]. The finding on digital rectal examination in patients with sigmoid volvulus varies. The rectum may be empty like in our index patient. However, there may be fresh blood in the rectum especially when there is associated pathology such as enteric fever [20].
There are different modalities for the treatment of sigmoid volvulus depending on the facilities available and expertise and experience of the surgeon. In developed countries, an initial endoscopic decompression and detorsion is practiced for stable patients. Subsequently, laparoscopic sigmoid resection is performed. In our setting, laparotomy with resection of the redundant sigmoid colon is performed. This is what was done for the index patient.
Outcome of management of sigmoid volvulus is generally good. However, one study from Ethiopia documented more morbidity and mortality in patients who had bowel resection and anastomosis for gangrenous bowel [21].
4. Conclusion
Sigmoid volvulus is an uncommon cause of bowel obstruction. In the absence of endoscopic facilities for decompression and detorsion at the acute stages in stable patients, bowel resection and anastomosis through laparotomy is an effective modality of treatment.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org