Pulak Mutsuddy1, 2*, Mohammed Abdus Salam2 and Prudence Hamade 3
1Former Epidemiologist. Communicable Diseases Control (CDC), Directorate General of Health Services (DGHS), Ministry of Health & Family Welfare and Epidemic Control Preparedness Program (ECPP).
2Former Director, Research Administration; Clinical Science Division (CSD); and Chief Physician, Dhaka Hospital. International Centre for Diarrhoeal Diseases & Research, Bangladesh.
3Senior Technical Advisor. Malaria Consortium, UK.
*Corresponding Author: Pulak Mutsuddy, Former Epidemiologist. Communicable Diseases Control (CDC), Directorate General of Health Services (DGHS), Ministry of Health & Family Welfare and Epidemic Control Preparedness Program (ECPP).
Received date: May 18, 2024
Accepted date: June 07, 2024
Published date: June 20, 2024
Citation: Pulak Mutsuddy, Mohammed Abdus Salam and Prudence Hamade.(2024) “Cholera Epidemic to Covid-19 Pandemic: Impact analysis to strengthen the existing Health System of Bangladesh”. International Journal of Epidemiology and Public Health Research, 5(1); DOI : 10.61148/2836-2810/IJEPHR/063.
Copyright: © 2024 Pulak Mutsuddy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Bangladesh has developed a uniquely successful system to control deadly cholera epidemics, which is embedded in the existing health system. Control of the Covid-19 pandemic situation in Bangladesh was a missed opportunity to become a “role model”, as except case management, most of the required interventions had been similar to those as of the cholera epidemics. The “test and trial” processes from the “cholera control” experiences could be followed in building and delivering pandemic preparedness and response in the initial stages of the Covid-19 pandemic in Bangladesh.
Methods: The study is descriptive in nature and is limited to frequency distributions in tables and figures.
Results:
Aanalysis of 1,714,091 confirmed Covid-19 cases and 28,965 deaths revealed that the young and middle age populations (86.4%) were the most vulnerable and that 80% of the deaths occurred among people older than 50 years. Diabetes Mellitus and Hypertension were the two most co-morbidities (65%) and one quarter of the deaths were associated with 4 to 5 co-morbid chronic diseases. Our verbal autopsy results indicated that majority of the deaths (60%) occurred within 10 days following admission to Intensive Care Unit for ventilation support.
Conclusion:
The need for intensive care posed a huge extra burden for the poor and the middle-income people as the services required out of pockets (OOPs) expenses, suggesting the need for reforms in the existing health system like Public Private Partnership (PPP), an effective, reliable electronic database at each level to be prepared to respond, and mitigate any health crisis.
cholera epidemic; covid-19 pandemic; learning process; co-morbidity; electronic database
1. Introduction:
1.1. Contextual Framework:
Cholera is an acute secretory diarrheal illness caused by Vibrio cholerae, leading to severe dehydration, high fatality rate and has been responsible for many lethal outbreaks in the world. The Ganges delta, particularly Bengal, remained historical epicentre of cholera and Bangladesh is recognised as “cradle of cholera” from the ancient times [1-2]. The first recorded epidemic of cholera occurred in the Southwestern part of Bangladesh in 1817, and since then, numerous outbreaks occured that crossed borders to become global pandemics [3]. According to the World Health Organization (WHO), cholera affects 1.3 – 4.0 million people killing 21,000 - 143,000 people globally, each year. [4].
The first case of the Covid-19, caused by the novel SARS CoV-2 was reported from the Wuhan province of China in December 2019 [5]. The disease rapidly spread to other countries, and the WHO declared it a pandemic on 11 March 2020 [6]. Bangladesh was also an affected country, reporting its first case on 08 March 2020 [7]. The novel coronavirus (nCoV) differs from its predecessors SARS COV-1 and MERS and thus, the early stages of the pandemic were a global learning phase [8]. Bangladesh had a strong record of accomplishment in curbing the severity of cholera outbreaks in the country. It thus had some advantages in dealing with such a big shock in terms of planning, coordinating, intervening, and resources assessments during the initial stage of the pandemic
1.2. Study Background:
Due to the perennial and escalating cholera epidemics in the country, the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) initiated a collaborative pilot project, Epidemic Control Preparedness Programme (ECPP) with the Ministry of Health and Family Welfare of Bangladesh (MoHFW) to control cholera epidemics in the country in the late 1983.
The pilot programme set up a system of collaboration between the ECPP, the Training, Extension, and Communication (TE&C) Division, icddr,b and the Communicable Disease Control (CDC), Directorate General of Health Services (DGHS), Bangladesh in 1985 [9]. The main objective was to build the capacity of the MoHFW in cholera epidemic investigations and interventions throughout the country. To ensure sustainability, the project developed a “Core Group of Experts” (doctors and nurses) within the MoHFW, who underwent training at icddr,b hospital and field visit in the affected areas by the icddr,b expert team.
The encouraging outcomes of the ECPP prompted the MoHFW to initiate its National Control of Dirahhoeal Diseases (CDD) Project in 1989 to reduce the burden of cholera in Bangladesh [10]. The trained “core experts” was engaged in the project to implement the project objectives. The core activities of CDD were the same as under the ECPP of icddr.b. The national surveillance system, DGHS, reported 1,48,4435 diarrhoeal cases and 19,592 deaths from 1985-1990 in the country [11]. The project activities remained operational up to the mid- 1998 and then merged with the first SWAp (Sector Wide Approach) programme - Health and Population Sector Program (HPSP: 1998-2003) under the Primary Health Care Operational Plan (PHC OP). Currently; cholera and other infectious diseases control program are under the CDC OP.
The transmission of Covid-19 is different from cholera, and its management is more complex and challenging; but the existing health system could have used the already tested “Cholera Control” model in establishing one for Covid-19 pandemic.
1.3. Objectives:
The aim of the study is to appraise the ongoing Covid-19 pandemic interventions through a broader perspective to incorporate the successful cholera control initiatives of the MoHFW. We also attempted a gap analysis within the existing health system, identify some shortfalls and recommend strategies to strengthen the country’s health system.
2. Methods:
The CDC, DGHS routinely monitors the epidemic situation routinely throughout the year at its control room, and collects information mainly on health- related emergencies, since 1983.
The study collected Covid-19 information from the District Health Information System-2 (DHIS-2 tracker data) from the first reported case in Bangladesh on 08 March 2020 through 31 July 2022. We also collected information on 227 patients admitted to a private medical college hospital in the Dhaka city (Universal Medical College and Hospital), and conducted 44 verbal autopsies on Covid-19 deaths. Moreover, the study further collected data from 14 Upazila (Sub-district) Health Complexes of the Chittagong District for the same period to assess the community transmission of Covid -19 in rural Bangladesh. The basic data reflects confirmed Covid-19 cases and deaths as reported by the Covid-19 surveillance systems of the Government of Bangladesh (GoB).
The descriptive study is limited to frequency distributions in tables and figures. No advanced analysis was attempted due to the nature of the data quality.
3. Results:
3.1. Covid-19 Pandemic in Bangladesh: Impact on Morbidity:
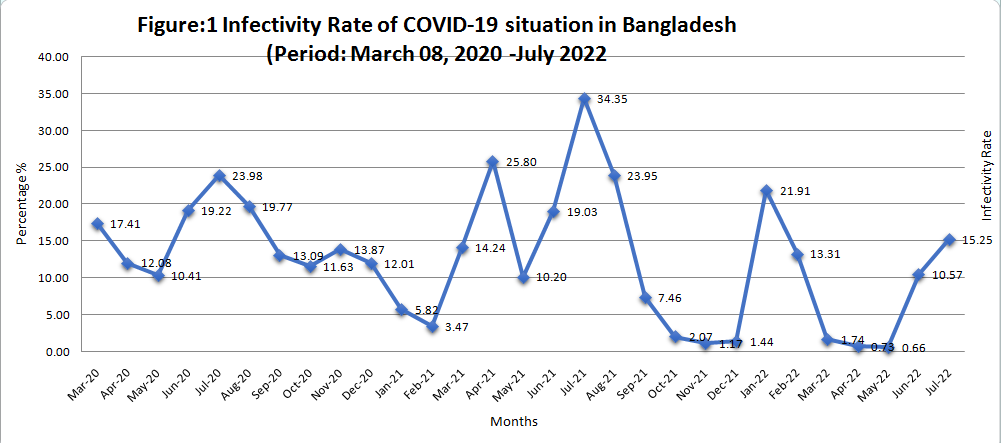
The National Covid-19 surveillance system of the DGHS reported 1,714,091 confirmed cases by using rRT-PCR, GeneXpert and Rapid Antigen tests and 28,965 Covid-19 associated deaths during the study period. The case fatality ratio (CFR) was estimated at 1.69 (Table-1).
|
Figure: 1 Trend analysis of Covid -19 cases from 2020-2022, based on monthly test confirmed cases from the HMIS, DGHS. The highest test positivity was observed in 2021 with maximum cases in July, 2021. Test positivity gradually declined after July 2021, and another peak was observed in early 2022. |
Table 1: Average infectivity rate and case fatality rate of Covid-19 variants in Bangladesh over the study period (March 2020 - July 2022)
|
Cov-2 varient and time period |
Duration |
No. Sample Tested |
No. Positive Cases |
Average Infectivity Rate (%) |
No. of deaths |
Case fatality Ratio (CFR %) |
|
Alpha and Beta variant (08 March 2021 to 07 May 2021) |
14 months |
4527804
|
638324
|
14.09 |
11712 |
1.84 |
|
Delta variant (08 May 2021 to 06 December 2021) |
6 months 6 days |
5028686
|
693326
|
13.79
|
16065 |
2.32 |
|
Omicron variant (06 December 2021 to July 2022) |
6 months 25 days |
3402488
|
382441
|
11.24 |
1128 |
0.29 |
|
Total |
29 months |
129,58,978 |
171,4091 |
13.27 |
28,965 |
1.69 |
Our analysis (Table 1) demonstrated that the country faced the serious consequences within a short 6 months’ period following the emergence of a new Delta variant in 2021 contributing 40% of total patients and 55.46% of total deaths.
|
Age Group |
Total Cofirmed Cases |
Percentage (%) |
|
0-14 |
78,496 |
4.6 |
|
15-34 |
654,931 |
38.42 |
|
35-54 |
817,839 |
47.97 |
|
55-74 |
297,460 |
17.45 |
|
75+ |
44,126 |
2.59 |
|
Total |
171,4091 |
100 |
Table 2: Age group distribution of Covid-19 cases in Bangladesh (March 08- July, 2022)
The middle- age group (48%) and the young age group population (38.42%) were mostly affected, which comprises 86.42% of the total confirmed cases in Bangladesh. Conversely, 20% of the patients were older than 54 years. (Table-2).
|
Name of Upazila |
Population |
Samples Collected |
Number of positive |
Sample positivity rate |
|
Satkania |
447871 |
5825 |
1519 |
26.08 |
|
Sitakunda |
460565 |
5425 |
2901 |
53.47 |
|
Boalkhali |
251701 |
7333 |
2257 |
30.78 |
|
Patiya |
548725 |
8662 |
2489 |
28.73 |
|
Anowara |
335461 |
6926 |
1845 |
26.64 |
|
Chandanaish |
268595 |
4235 |
1274 |
30.08 |
|
Fatikchari |
628766 |
12086 |
3422 |
28.31 |
|
Mirersarai |
536153 |
4614 |
1522 |
32.99 |
|
Hatahazari |
495861 |
16294 |
6787 |
41.65 |
|
Lohagara |
351460 |
5091 |
1607 |
31.57 |
|
Sandip |
368419 |
1482 |
948 |
63.97 |
|
Rangunia |
381004 |
6328 |
2599 |
41.07 |
|
Banshkhali |
565313 |
13426 |
1522 |
11.34 |
|
Raozan |
395848 |
10758 |
4755 |
44.20 |
Table 3: Covid-19 situation at upazila level, Chittagong (as on July 2022)
The upazila wise (sub-districts) data showed (Table 3) that the test positivity (26.44%) in the Chittagong district of Bangladesh was double that of the national average of 13.27%.
3.2. Covid-19 pandemic in Bangladesh : Impact on Mortality
The Case Fatality Rate (CFR) in Bangladesh was high (9.8%) at the beginning of the pandemic, which declined over time due to decentralization and expansion of the testing coverage (average 1.6%).
|
Age Group |
Male |
Female |
Total |
|||
|
|
No. |
Percent |
No. |
Percent |
No. |
Percent |
|
0-10 |
44 |
0.24 |
39 |
0.37 |
83 |
0.29 |
|
11-20 years |
107 |
0.58 |
75 |
0.72 |
182 |
0.63 |
|
21-50 |
2,973 |
16.05 |
2,798 |
26.84 |
5771 |
19.94 |
|
51-60 |
3980 |
21.49 |
2704 |
25.94 |
6684 |
23.09 |
|
60+ |
11,417 |
61.64 |
4,808 |
46.12 |
16,225 |
56.05 |
|
Total |
18,521 |
63.99 |
10,424 |
36.01 |
28.945 |
100 |
Table 4: Age and gender distribution of Covid-19 deaths in Bangladesh (March 2020- October, 2022)
Table 4 demonstrated that 72% of all deaths occurred among those aged 50 years, and above; predominately in males (nearly 64%).
|
Co-morbid condition with chronic diseases |
Deaths |
Survivors |
||
|
Number |
Percentage |
Number |
Percentage |
|
|
None |
1 |
2.29 |
43 |
23.50 |
|
Single chronic disease |
4 |
9,09 |
41 |
22.40 |
|
2 chronic diseases |
15 |
34.09 |
45 |
24.59 |
|
3 chronic diseases |
13 |
29.55 |
37 |
20.22 |
|
4 chronic diseases |
4 |
18.18 |
15 |
8.20 |
|
5 chronic diseases |
3 |
6.82 |
2 |
1.09 |
|
Total |
44 |
100 |
183 |
100 |
Table 5: Co-morbidity associated with Covid- 19 cases in Bangladesh
Among the 44 verbal autopsies conducted and 183 survivors investigated, 64% of deaths had 2-3 chronic conditions and another 25% had four or more co-morbid diseases. On the other hand, 23.50% of the survivors had no co-morbid diseases (Table-5). Diabetes Mellitus (DM) and Hypertension (HTN) were the leading co-morbidities associated with deaths (75%).
|
HCT findings of lung involvement |
Deaths (n=44) |
Survivors (n=183) |
||
|
Number |
Percent |
Number |
Percent |
|
|
No involvement |
0 |
0 |
9 |
4.92 |
|
Less than 10% |
2 |
5.5 |
14 |
7.65 |
|
10-30% |
3 |
8.3 |
45 |
24.59 |
|
31-50% |
10 |
27.8 |
43 |
23.50 |
|
51-70% |
6 |
16.7 |
29 |
15.85 |
|
71-80% |
9 |
25 |
12 |
6.56 |
|
80+% |
6 |
16.7 |
6 |
3.28 |
|
Not done |
8 |
18.18 |
25 |
13.66 |
|
Total |
44 |
100% |
183 |
100% |
Table 6: Helical Computed Tomography (HCT) findings of lung involvement in Covid-19 cases and deaths
Lungs were involved in all fatal cases; more than 50% of the lungs were affected in 58.4% of the fatal cases older than 50 years. Among the survivors, only 4.9% did not have evidence of lungs involvement and another 26.7% had greater than 50% lungs involved (Table-6). About 60% deaths occurred within 10 days of hospitalization, while 70% of the survivors were released from hospital within 10 days of admission. (Table-7).
|
Duration of Hospitalisation (Days)
|
Deaths |
Survivors |
||
|
Number |
Percent |
Number |
Percent |
|
|
1 - 5 Days |
12 |
27.27 |
54 |
29.51 |
|
6 - 10 Days |
14 |
31.82 |
74 |
40.44 |
|
11 – 15 Days |
8 |
18.18 |
36 |
19.67 |
|
16 – 20 Days |
5 |
11.36 |
9 |
4.92 |
|
21 – 25 Days |
3 |
6.82 |
4 |
2.19 |
|
26 – 30 Days |
2 |
4.55 |
3 |
1.64 |
|
Over 30 Days |
0 |
0 |
3 |
1.64 |
|
Total |
44 |
100 |
183 |
100 |
Table 7: Length of stay (days) in hospital of the fatal cases and survivors
4. Discussion:
Bangladesh has had a uniquely sucessful experience in controlling deadly cholera epidemics using its CDD programme of GoB. Adoption of a similar programme based on learning from the past within the existing health system could help the country in better control Covid- 19 pandemic. The health system failed to recover from the initial major shock of the pandemic to make an early and coherent action.
The failure to establish a nation-wide reliable systemic surveillance system resulted in gross under-reporting of cases and deaths throughout the pandemic, as in cholera epidemic situation. In appraising the demand side perspectives, we observed the limitations of Covid-19 testing was not patient-friendly; there was also a lack of an effective awareness and preventive response programme, resource constraints, lack of “tracing and testing” that facilitated the risk of community transmission.
At the initial stage, the Institute of Epidemiology, Disease Control and Research (IEDCR, an independent institute under the DGHS) could but did not follow the established guidelines of the control room reporting approach of the CDC, DGHS that existed within the health system. In recognition of the problem, the health authority responded quickly by ‘decentralizing’ testing facilities and setting up of a 24/7 Integrated Control Room (ICR) for Covid-19 surveillance throughout the country.
The infection rate was very high due to the limited test coverage and tratment facilities, which remained almost the same throughout 2020. This is true for most infectious disease epidemics in the initial stages, when the communities are not generally prepared to make an appropiate response in case reporting. We observed that the infection rate was highest in mid-2021 when the more contagious Delta variant from the neighboring country (India) emerged through the Port of Entries (PoEs), as there was a lack or absence of a reliable screening system in the border areas. The country could not cope with the overwhelming situation, as 40% of total cases and more than half of deaths (55.46%) recorded within the shortest period (6 months); over 29 months of the study period.
The health system was in a limbo, due to lack of resources, coordination, case management, hospital beds and ICU facilities. People were desperate to secure a hospital bed throughout the country [12]. Based on cholera epidemic experiences [13-14], make-shift treatment centres were initially established by investing huge resources, but were prematurely closed due to low case reporting in 2020 [15]. The only successful intervention in coordination with other ministries was to contain the Wuhan (China) migrants under institutional quarantine in the initial stage of the pandemic. The health authorities could not establish institutional quarantine for sucessive pressure of migrants at all PoEs. Also, they did not have the ability to introduce effective home quarantine interventions [16].
Community engagement plays a crucial role in preventing transmission of outbreaks/ epidemics, which was demonstrated during cholera epidemics [17]. The success of this intervention was almost ignored in the initial stage of the pandemic but finally some interventions were established following the “Cholera Control model” like establishing of flue corners, swab collection, bed allocation for Covid patients, designated Covid-19 hospital, and an enhanced reporting system. The exception was the executive policy decisions by the Honarable Prime Minister for quick procurement of Covid-19 vaccines, incentives for the front line fighters, vulnerable groups, and her continous vigilance over the pandemic situation [18]. However, the community engagement was very insignificant, as the upazila and sub-upazila administration is under the Ministry of Local Government, Rural Development & Co-operative (MoLGRDC), where the MoHFW has less control. The health sector made sporadic attempts at individual and community levels but not in a coordinated way to get the desired results.
Cholera epidemiology demonstrated that there would be around 10 mild or sub-clinical cases in the community for each confirmed case of cholera that may develop overt disease later. [19-20]. Therefore, it is easy to monitor the area around the confirmed cases and initiate measures for prevention of infection transmission. However, in case of Covid-19, no such epidemiological data were available, although wearing masks, quarantine issues and social distancing had been advocated to limit transmission [21-22]. These measures were difficult to implement and monitor in terms of population density, average household size and living space sharing in our country context [23]. The health authority has no control over monitoring the activities at the household level, especially in case of these imposed interventions [28]. Such behavior- change interventions are a continuous process requiring significant efforts and long-term investments. The health authorities could not expect instant results within the short-run in the pandemic situation. Experiences from cholera epidemics showed that behavior change interventions such as the use of safe drinking water and WASH took time to establish and did not have immediate outcomes but over time of nearly four decades. Of course, we believe there were some positive effects and little changes occurred but we have to allow more to get expected results [24].
The verbal autopsy study revealed that lungs were immediately affected in all the fatal cases. These findings corroborate with findings of other studies - the more the age, the more the extent of lungs involvement. [25]. All fatal cases had pronounced respiratort distress, were admitted to the Intensive Care Unit (ICU) and 80% of them needed Continuous Positive Airway Pressure (CPAP) or Bilevel Positive airway pressure (BiPap).
Although the study was limited to a few verbal autopsy cases, we may assume that the situation produced a management and resource crisis throughout the country. The critical care protocol was under enormous pressure and the situation posed a big challenge in dealing with such emergencies within the existing resources. The health authorities did not pay the needed attention before the pandemic seriously in developing a comprehensive Critical Care Management protocol [26]. We observed that 60% of deaths occurred within 10 days after hospitalization. Although our study did not cover the socio-economic status of the patients, we can still assume, it was extremely difficult to afford the supporting cost for ICU in the private sector. This is a huge extra financial burden for the poor and the middle-income people to bear from Out of Pocket (OOPs) expenses to invest in health, especially when many people faced notice of termination from their jobs during the pandemic period. The recent study by BNHA (Bangladesh National Health Accounts) findings revealed that the OOPs to buy health services have increased in the recent years [27]. The only sustainable alternative under such situations would be the long-waited reforms – the Public Private Partnership (PPP) in accordance with the 2012 guidelines [28]. However, the health authority failed to handle the issue, or properly addressed the governance issues, which has deepend with more crises. It is encouraging to note that the Asian Development Bank (ADB) has initiated implementation of a PPP project within the health sector [29]; a pipeline project is being developed (2022-2027) that addressed the PPP issues.
The study revealed that more than 80% of deaths occurred among patients older than 50 years and that the probability of death increased with increasing age [30], although the yonger people (86.39%) are more vulnerable to Covid-19 infection. The reason may be the increased mobility of the young people for their earnings or household needs, and may pay less attention to the suggested health guidelines. The older age group may be infected through cross-infection with other family members and had higher risk of death due to reduced immunity and/or comorbid conditions. The male preponderance in cases and deaths can be explained by their greater exposure to outer environment as reported in other studies. [31-32].
In our study, about 2/3rd of the deaths were associated with chronic comorbidities, most notably diabetes mellitus and hypertension (65%), a finding similar to other studies [33-34]. We also observed that 23.50% survivors did not have any comorbidity, and it was alarming to note that a quarter of deaths (25%) were associated with 4-5 comorbidities. It was evident that co-morbidity played a vital role as risk factors of both morbidity and mortality as in other studies [35]. People with underlying long-term non-communicable diseases (NCDs) such as hypertension, diabetes mellitus, cardiovascular disease, chronic respiratory disease and cancer had a higher risk of developing severe and fatal disease. Therefore, it should be a priority to address the basic protective measures such as screening and management of chronic diseases at the primary (community clinic level) and secondary level (sub-district level) through the PHC approach [36]. The NCD Operational Plan (OP) of the DGHS has some limited focus on the issue [37], but needs more attention for an effective long term care (LTC) plan in terms of resources and drug availability as in other countries [38], as the aging populations is rapidly growing in Bangladesh [39].
4.1. Conclusion and recommendations:
Our analysis strongly suggests the need to develop and provide an effective package of interventions for prevention of infectious diseases and their effective management using the existing “Cholera Control model”. The health authorities failed to use the lessons learnt initially from the sucessful project investment during the pandemic. In addition, given the magnitude of the problem of data availability, quality and reliability, our study concentrated on limited focus on morbidity and mortality findings and identified some gaps that should be addressed in dealing similar situations in the future.
Based on the study findings, we recommend strengthening the existing health system: (a) recognise the importantance of community participation in tracing early cases in the community; (b) the role of inter-ministerial/inter-departmental co-ordination for implementation and monitoting. The MoHFW should lead as a front liner; (c) initiate the PPP approach in accordance with the guidelines and contracting out the critical care management and specific diagnostic facilities within the private health facilities with due diligence; (d) consider the transition of disease patterns, aging factors, and pre-disposing factors which have impact on COVID-19 cases and deaths, NCD challenges should be properly addressed through community- based PHC approach.
The Covid-19 pandemic has demonstrated that it is time to implement the long awaited reforms to the existing health system. The MoHFW should come forward to secure and think seriously about a “health protection scheme” for the entire population of Bangladesh [40]. In addition, as a benefit to the existing SHR, HMIS; an effective, reliable, electronic database at each service delivery level will allow the health service to be prepared to respond, and mitigate any health crisis. Finally, vaccination coverage should continue and there should be continued research & deveopment (R&D) into the health system.
Data Availability:
The data used for analysis of this study may be requested from the corresponding author upon request
Conflicts of Interest:
The authors declare that they have no conflicts of interest
Acknowledgement:
We are greatful to the HMIS, DGHS staff members, who provided us the needed information from time to time. We are thankful to the Universal Medical College Hospital, Dhaka city for providing access to their patient database. Also, greatful to Mr. Ahsan Sadiq, International Consultant, Canada and Troyee Mutsuddy, University of Manchester, UK who has provided their busy time to edit the menuscript.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org