International Journal of Epidemiology And Public Health Research
OPEN ACCESS | Volume 9 - Issue 1 - 2026
ISSN No: 2836-2810 | Journal DOI: 10.61148/2836-2810/IJEPHR


Keltice Manimbuh Ateghang1, Ndeso Sylvester Atanga2,3, Nkengafac N Fobellah3, Godman Mendem Aying1, Nwakaogor Glory Ugochukwu4,5, and Bernadette Ateghang-Awankem 1*
1 Pan African Health Systems Network, Nussloch. Germany
2 Faculty of Health Sciences, University of Buea, Cameroon
3 St. Monica University Institute, Buea, Cameroon
4Healthy Environment for International Development, Nigeria
5Nnamdi Azikiwe University, Awka Nigeria
*Corresponding Author: Bernadette Ateghang-Awankem, Pan African Health Systems Network, Nussloch. Germany.
Received: November 22, 2021
Accepted: November 30, 2021
Published: December 04, 2021
Citation: Keltice M Ateghang, Ndeso S Atanga, Nkengafac N Fobellah, Godman M Aying, Nwakaogor G Ugochukwu. “Bernadette Ateghang-Awankem”. International Journal of Epidemiology and Public Health Research, 1(5). DOI: http;//doi.org/03.2021/1.1022.
Copyright: © 2021 Bernadette Ateghang-Awankem. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In Sub-Saharan Africa today, finances for health systems can be said to be insufficient. Given the threats posed by covid-19 globally and its intensity in developed countries characterized with the huge loss of lives. Despite the huge available resources and modern health facilities in developed countries, Covid-19 still posed a great threat to the health system. The growing intensity of the Covid-19 pandemic is likely to frustrate Africa's health system due to limited available resources. This research was a quantitative and descriptive research focusing on health financing in Cameroon. Findings from the research showed that poor economic and financial hardships were the leading causes of poor health systems in Cameroon, and also added that the government still spent very little on health financing. The COVID-19 was also assessed to see its impact in Cameroon, which showed that although aid was received from the international community, there was a slowdown in economic activities.
1.1 Introduction
It is often said, “Health is wealth”, but looking critically at some African countries, one can reverse this statement with, “wealth is health”. Because the health systems have truly improved in the past decades, but those of African countries have done so sparsely due to poverty, poor infrastructure and mismanagement of funds.
Looking at Africa today with its very high rate of population growth, it is very important to have a look at the health sector because an increase in population will automatically lead to an increase in the demand for health facilities. This is the reason why it is very important to constantly analyze the sector of public health to see if the services are growing as the population is growing, is the population able to pay for these services? In Sub-Saharan African Countries, one can see that the improvement in the health system has not only led to an increase in political, social and economic welfare of the population, but has also improved the life expectancy and educational performance has as well noticed a positive change. Considering the political instability we are noticing in the world today, because of the health systems being challenged by Covid-19 (especially the SARS-CoV-2 variant), it is a clear indication that a good health system is not only a key factor to human development but also plays a major role to stabilize the society and protect the population (1)
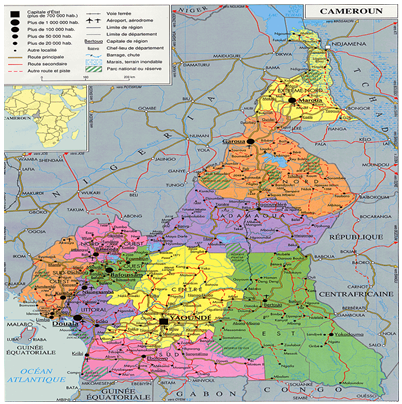
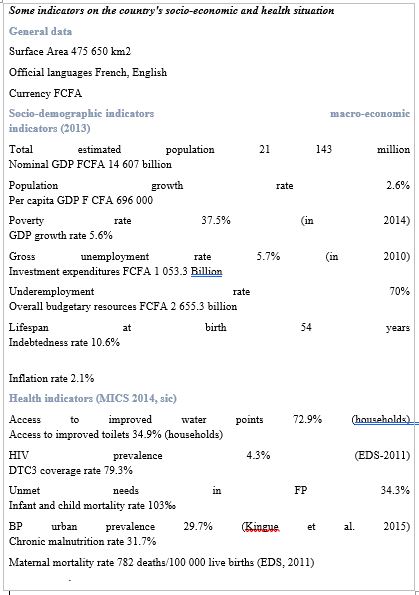
The study area, Cameroon, which lies within the Central African sub region, has a population estimated at more than 27,031,658. The most populated towns in Cameroon are Douala, Yaoundé and Bamenda. Almost half of its populace (44%) lives in rural areas (2). With both high birth and death rates, the demographic distribution resembles a classical expansive population pyramid. Almost two-thirds of Cameroonians are younger than 25 years of age; the average life expectancy at birth is 58.6 years (United Nations Development Programs [UNDP], 2018).
The Per capita income of Cameroon in 2017 was $1,340 making it a low middle income country .The current Health expenditure (CHE) per capita has been on an increase in the last 20 years; US$43, 48, 54 and 64 in the years 2000, 2005, 2010, 2016 respectively “ though out-of-pocket” (OOP) spending has been the main source of payment for health services for majority of Cameroonians throughout this period. The low-income populations are defined as those living below the national poverty level (NPL) of 931 FCFA (1.5 USD) per day. Given this population structure, it is creditable to do a study to know how this population living below NPL meets it Health financial needs amid deadly diseases such as malaria, HIV/AIDS pneumonia and diarrhea among others.
1.1.1 Research aim and Objectives
The main objective of this research was to study the Health Care Financing in Africa: A Case Study of the Health System in Cameroon. To achieve this, the research started by:
-Looking at the health structure of Cameroon's Health System
- Household spending on health was looked at, also making a comparison with other countries to see if the difference was similar.
-A look at the Covid-19 was also done as it was the most recent pandemic affecting the health sector and Cameroon as well.
1.2 Research methodology
The data for this publication came from political documents and grey articles. The documents reviewed provided information on health financing, particularly in Cameroon and SSA. Internet sources such as PubMed, Medline, WHO, Popline, World Bank Database were very relevant, the researcher was not limited to health financing in Cameroon, health financing and financing policies but included other African countries and SSA in particular. Other publications were identified through the references cited in the relevant articles and reports. (3)The researcher reviewed only papers published in English and date restrictions were applied to the search. Also, additional information was obtained from the authors' experiences. These included working experiences from Cameroon
2. Discussion of Results and findings
2.1 Structure of the health system in Cameroon
According to statistics, people living in low-income countries are much more likely to die from a communicable disease than from a non-communicable disease. Despite the worldwide decline, six of the highest 10 causes of death in low-income countries are communicable diseases. Malaria, tuberculosis and HIV/AIDS all remain in the top 10, but all have seen significant declines thanks to international donors who are fighting against their increase. The largest decline among the top 10 causes of death in this group is HIV/AIDS, with 59% fewer deaths in 2019 compared to 2000, or 161,000 and 395,000 respectively (4).
In Cameroon, the Ministry of Public Health is responsible for developing the health policy and ensuring the implementation of these health policies in the country. Although this ministry has achieved a lot for the past decades, weaknesses could still be seen in aspects such as child mortality rates which could be noticeable with mortality rate of 74.8 deaths per 1,000 live births in 2019, when compared with other African countries like Ghana and Rwanda, where there has been a little bit of Health improvement. (5)
The health system in Cameroon comprises of three sub-sectors:
- The sub-public sector consists of public hospitals and the health structures under the care of other ministerial departments (Ministry of Defense, Ministry of Labor, Employment and Social Welfare, Ministry of National Education).
- The sub-private non-profit sector are the hospitals and health structures under religious denominations (Catholic, Baptist, and Presbyterian churches), associations and various non-governmental organizations and not-for-profit organizations.
- The sub-sector of traditional medicine which is an important part of the system should not be ignored. It should be noted that herbal medicines also play an important role in the health sector in most African countries and Cameroon in particular. (5)
The health system in Cameroon is also structured in three levels, with each having administrative, sanitary formation and structures and dialogue structures.
(I) Central level. Central Services of the Ministry Public Health: These services coordinate, regulate and develop ideas, methods and policies within the field of health.
(II) Intermediate level: These structures are depicted overall by the reference hospitals, University teaching hospitals, regional hospitals, and agencies under their control. These structures are also depicted and assimilated by the regional hospitals. This intermediate structure has other units such as. Structures of CENAME: These structures are units depicted by the CAPP (Center Pharmaceutical provide provincial) and therefore, are the pharmacies within the general hospitals and its headquarters, structure of care and others.
(III) Peripheral level:
These are body Structures depicted by the district health services, they implement the national programs. Have other structures within it such as, structures of care which is represented by the district hospitals, medical centers and district health centers, Structures of SYNAME depicted by the pharmacies for health coaching courses of the previous levels, further as non-public pharmacies
Structures for dialog: These are the COSADI, COGEDI, COSA and COGE. Source: conceptual framework of the D/S viable revised (MSP). In all, the main financing of the state-run hospitals comes from the state budget, other major donors are the local authorities, NGOs, and the international community. (5) Spending on Health in Cameroon
Government.
In 2016, of the health expenditure per capita of $64 spent, estimated that Out-of-pocket spending accounted for 70% while domestic public spending, voluntary health insurance, aid accounted for 13%, 9% and 6% respectively and other sources accounted for just 2%.
Statistics show that the state budget of Cameroon still allocates less than 5% of its spending on healthcare, considering a population of about 27,031,658, this is a clear indication that the health sector still lacks in quite a number of factors ranging from infrastructure, equipment and personnel.
According to the Abuja conference in 2001, African leaders agreed to pledged to allocate at least 15% of their national budget to the health sector (6), but to how far this agreement has been effectuated is still a question of the day This 5% is below the World Health’s Organization (WHO) standard of 10 %, thus clearly indicating that the health cost is mostly covered by the Households (out of pocket payment), NGOs and donor organization in Cameroon and most African countries. Critically looking at African countries and their high level of corruption, it could be said that about 1% of this budget will end up in the pockets of administrators, thus making the situation hard for the population to be provided with the much-needed health care systems. This low government spending could be linked to the low per capita income following the economic crisis between 1986 and 1995. Another major reason is the presence of strong organizations such as the Catholic and protestant church whose solidity was made reliable back in the colonial periods. (7)
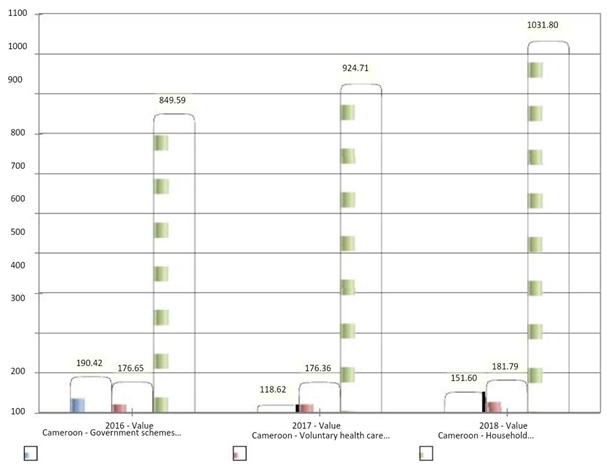
Graph A: A Cameroons Case over a three years’ period https://apps.who.int/nha/database/ViewData/Indicators/en (4)
Graph A: Cameroons health expenditure over a three years’ period in million current US$
2.1.1 NGOs and other organizations.
Quite a good external financing source exists in SSA, looking at the case of public enterprises it should be noted that some have their own health facilities and those without owned facilities use private for-profit facilities for their workers. The public social insurance, National Social Insurance Fund (NSIF) abbreviated as (CNPS) in French renders good services, but unfortunately does not yet include health coverage to it insured but covers claims responsibility in areas of, accidents at work, family benefit, invalidity, old-age, and death. Other companies have internal schemes which, like in some African countries, are obligatory- but in most cases they are voluntary. (7)
All in all, the sub-sector of private health providers, who complement and often compete with government suppliers, consist of non-profit religious missions and NGOs, for-profit providers, private clinics, pharmacies, drug retailers, and traditional healers. The bulk of non-profit facilities are operated by the Catholic and Protestant Health Services, who formerly operate about 179 facilities, Religious missions and NGOs finance a small part of their activities from donations in the form of staff, drugs, and equipment from their denominations.
Mutual health also plays an important role in sub-Saharan Africa, which treats quite a variety of diseases and offers outstanding services such as free X-ray, generic drugs, Surgery coverage of birth among others, provided at integrated health centers, religious and in public hospitals. This system requires an annual contribution of 15,000FCFA covering 75% of the hospital cost to a maximum 290,000FCFA for 4 persons. (8)
2.1.2 Household expenditure on health in Cameroon
Looking at the SSC and their economy, it could be said that most of the masses rely on agriculture to earn a livelihood. Putting Cameroon at the forefront of discussion, the majority of its inhabitants are below the National Poverty Level (NPL). Matched with unstable economic and political crises present in this country, it is evident that the household’s income has really reduced as many of the inhabitants have abandoned their Regions affected, hence leaving behind their primary sources of income to seek refuge in the francophone regions. This is a clear indication that this population is going through tougher times to finance their health bills, therefore a huge amount of out-of-pocket payment (OOP).
This low rate of financial security and medical attention - in time of need - leads us to the majority of the population, who are under NPL, leaving from “hand-to-mouth” and having higher chances of getting sick. Most of these people go through various processes in order to finance their bills. These include, personal savings from jobs done or from little economic activities such as farming and petty trading. A good number take loans from micro financial institutions (MFIs) or from “njangi” houses with very little interest rates (10FCFA per 1000 FCFA) others borrow from family members, friends and neighbors to finance their health bills. Still, other important sources include contributions from family members and close relatives which is mostly based on the principle of reciprocity in the sense of give-and-take which is mostly practiced in Africa in large and extended family circles (9).
https://apps.who.int/nha/database/ViewData/Indicators/en
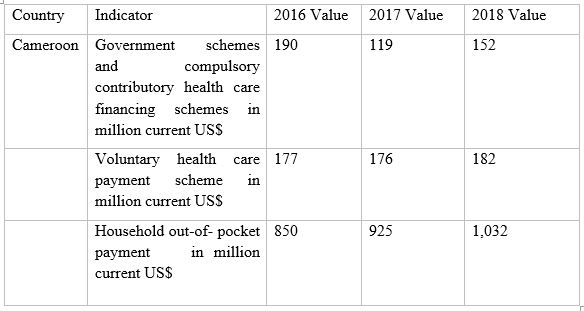
Table A: Tabular presentation of Cameroon's Health schemes in Million current US$.
The above statistics shows that the household has been spending so far enormous when it comes to health, OOP. (4)
3. Health Expenditure Compared with other African countries
Methods used, panel knowledge, from the institute for health Metrix and Analysis, on domestic government health expenditure in forty-six countries in sub- Saharan Africa from 1995 to 2015. A regression model was used to examine the factors affecting government health disbursal, and urologist decomposition was used to assign the factors' contributions to the explained variance in government health finance disbursal. (10)
Results: Although the expansion rate in government health finance payment in this geographical area has been positive overall, there are still major variations across subgroups. Between 1995 and 2015, government health finance payment in the geographical region grew by six.7% (95% uncertainty intervals [UI]: six.2% to 7.0%) every year, whereas in the Southern continent it grew by solely four.5% (UI: 4.5% to 4.5%) every year. Further-more, per-person government health (11), national income and additionally the share of government mercantilism were completely associated with government health mercantilism. The results from the decomposition, however, showed that individual country characteristics created up the simplest proportion of the explained variation in government health mercantilism across desert African countries. These findings highlight that a country’s policy choices are very important to determine how vibrant the health sector is. (12)
|
Country |
Indicators |
2017 Value |
2018 Value |
|
Cameroon |
Current health Million Cameroon expenditure NCU by financing schemes |
709,973 |
758,664 |
|
|
Government schemes and compulsory Million contributory NCU health care financing schemes |
69,050 |
84,249 |
|
|
Household out-of-Million pocket NCU payment |
538,267 |
573,392 |
|
|
Current health Million expenditure NCU by financing schemes |
241,060 |
257,177 |
|
Gabon |
Government schemes and compulsory Million contributory NCU health care financing schemes |
152,836 |
150,989 |
|
|
Household out-of-Million pocket NCU payment |
60,642 |
59,444 |
|
|
Current health expenditure Million by Health NCU Care Functions |
241,060 |
257,177 |
https://apps.who.int/nha/database/ViewData/Indicators/en
Table B: comparison of health expenditure between Cameroon and Gabon
4. Looking at Covid-19 and its impact in Cameroon.
COVID-19 which originated from the Wuhan city of China in December 2019 was announced as a pandemic by the WHO on March 11, 2020, it affected the world globally with Cameroon included (14). In Cameroon, the first COVID-19 case was recorded on March 6th, 2020, on a French national which alerted the nation to intensify measures toward fighting the Virus. (15). Some underdeveloped countries have been able to respond to this Pandemic positively while the developed countries have been fighting without end to come out of the Pandemic. (16). Reasons accountable for this could be related to higher rate of intensity of the Virus in developed nations which even led to the exhaustion of emergency facilities. This COVID-19 exposed the global inequality in the health sectors and has triggered the need for government and non-state health practitioners to work together towards finding solutions in combating Pandemic. It has also created the need for a unique global transformation of the health system to preempt any future pandemics
Concerning Cameroon`s population, with an estimated prevalence rate below 6%. (17), the vulnerable population has been really affected by this Pandemic beginning with very limited testing centers for COVID-19, which is coupled with the crisis in some of the regions making it difficult for some of the population in the suburb areas to move to test centers. Looking at bigger towns, challenges ranged from having access to clean water to washing their hands which is part of the preventive measure to stop the spread. To this effect, shopping for water to comply with measures is burdensome as the populations of these areas are mostly living below the minimum wage level. These preventive measures and more were already rooted in the minds of the population due to the Ebola crisis of 2014 which gave the population a pre-knowledge on handwashing and sanitization methods in times of crisis like this. (18),
Effects of the COVID-19 could also be seen in areas of mental health due to social distancing associated with distance learning. This lack of peer contact promotes stress factors in the educational system coupled with the fact that most could not get the necessary facilities needed for distance learning. Hence much family and parental support was needed towards moving Freely during this Pandemic, thus family life has also noticed a change in routine as parents are expected to spend more time with children to help, guide and orientate them. (19). On the other hand, the country received a lot of aid in terms of finance and non-financial which went a long way to calm down the tension in the country and also gave room for activities to get back on track.
The lockdown in Cameroon which went operational from the 18th of March 2020 affected economic activities especially the transport sector. It experienced a closure of borders. However, some of the restrictions were quickly removed. Bars and restaurants could be open from 6pm. Schools witnessed a pause in activities like the FENASSCO games and other important activities which brought social gathering together. (20). This population and governments which were already overwhelmed with problems affecting the –the Anglophone crisis, Bokhara attacks, climates change issues and others- could not really maintain the lockdown for a longer period of time.
The reaction of the population to this Pandemic shows quicker measures being taken by the older persons to adhere to preventive measures as they are well informed on the higher risk of being infected with this Virus and the consequences associated with it. Also men have been seen as respecting less social distancing due to carrier reasons and the need in providing for their families. (15).
Countries affected have been greatly organized. For example, India has widely switched its purchase method to online shopping as the lockdown period was relatively longer with higher infection. Plastic waste recyclability has also increased as many measures were being taken to keep cities and villages clean. (21)
The slowdown in economic activities due to social distancing. Looking at Cameroon with a population mostly surviving from their daily earnings. Implementing lockdown was really a dilemma to most of the urban population.
5. Recommendations to remedy the health financial issues in SSC
In the past years’ sickness, like infectious guinea worm, and other infectious diseases, have almost been eliminated through the adoption of effective solutions at the community level, and with outside support. Immunization campaigns are now successfully tackling polio and measles. Nonetheless, AIDS continues to decimate the population of Africa, which has 11% of the global population but 60% of the world's people infected with HIV. More than 90% of the 300-500 million cases of malaria detected in the world each year are in Africa-and the majority are children
2.2 Increase government spending on health
One key reason for Africa's health problems is that basic sanitation desires are still mostly unmet, says the report “Only fifty-eight of individuals living in Black Africa have access to safe water drinkable water.” If the governments of these countries make a greater attempt to improve on these issues, their population will rarely go sick, and so will the expenditure on health also drop considerably.
2.3 Reduction in corruption at the implementation level
Corruption still poses a major obstacle to development in African countries. This does not leave the health sector apart, given that the budget allocation in the health sector is generally low, and getting the right people to implement this small amount effectively will go a long way toward improving the health expenditure in the SSC.
2.4 Awareness on Digital health should be improved upon.
Technological advancement has touched the SSC to an extent, provided this improvement is applied judiciously in the health sector, health expenditures would really notice a significant reduction. Here, aspects of the reliability of digital health should be made impressive in the minds of the population. Data protection should also be considered as a good basis of building this system within the health sector. A relevant example from Cameroon is GiftedMom, associate app and SMS service that permits pregnant ladies and new mothers to remotely consult with from: |visit| refer to |talk over with |sit down with} health specialists for check-ups and obtain advice on prenatal care. Such measures not only reduce transportation cost but also helps in the minimization of risk of being infected in times of corona.
2.5 Health support schemes ought to be created on the market
Community value sharing schemes have provided thirty-five of Mali's fifty-seven community health centers with employees trained to deliver babies and do emergency caesarean operations-thus, creating competent medical specialty care in the market to thousands of ladies. The United Nations agency couldn't have antecedently afforded it.
2.6 Conflict Resolution
While other countries are busy looking for and implementing disaster risk reduction strategies in their countries, most African countries are today characterized by intertribal wars, ranging from the Boko-haram insurgent attacking from Nigeria to the northern regions of Cameroon, the Anglophone crisis in the English speaking regions of Cameroon etc. Had all the effort and resources applied to these conflicts fuel these conflicts were invested in the health sector, Africa would have been one of the best, today, in the provision of health facilities.
6. Conclusion
This research was out to investigate health financing in Africa taking Cameroon as a case study. From the material presented so far, the Household still provides more than half of the financing on health and the rates have always been increasing and are still increasing. This research paper has also attempted to analyse the health structure of Cameroon, which is the same in most SSC, the spending organs on health, a view on household expenditure on health, a comparison on health financing within the SSC and most especially recommendations to curb some of these situations. At this stage one could say that African countries still need a lot of effort to be able to meet standardized, affordable medical facilities and health insurance schemes. I plus point could be given to countries like Rwanda which have been able to pool resources to from several sources to ensure the coverage of the majority of the population through prepayment mechanism, Others are Egypt, with very low maternal mortality rate, Sierra Leone whose governments expenditure on health is above 16% of its total GDP. It is now left for the whole world to see into it, if the health condition in African countries is up to standards for more is still to be done to improve this sector
1.1 Appendix














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org